In late 2025 the United States launched bilateral negotiations for health aid as part of the “America First” Global Health Strategy.The agreements were negotiated after the elimination of the US Agency for International Development (USAID) in early 2025 and raise concerns that health aid is being inappropriately leveraged to extract terms beneficial to the US in negotiations around natural resources and access to sensitive health data from recipient countries.
The agreements with Ethiopia, Kenya, Mozambique, Nigeria, and Uganda were briefly posted to the State Department’s Freedom of Information Act Library on March 13, 2026, under the Case-Zablocki Act, which requires timely public disclosure of concluded international agreements. However, days later they were removed after the New York Times reported that the US had explicitly linked a $1 billion health package to access to Zambia’s minerals. Rwanda and Liberia’s agreements were never officially released and became publicly available only through leaks. The original agreements can be found on this page, which will be updated as other verified agreements become available.
The following is a detailed human rights assessment of the text of the bilateral health Memoranda of Understanding between the US and Ethiopia, Kenya, Mozambique, Nigeria, Rwanda, Liberia, and Uganda.
Reproductive Rights
All seven agreements require partner governments to provide the US government with broad access to data and information to monitor compliance with the Helms Amendment, a US law that prohibits US foreign assistance from being used to pay for abortion as a method of family planning or to motivate or coerce a person to practice abortion.
US foreign aid has been subject to Helms Amendment restrictions since 1973 and rights organizations have, for decades, documented its harmfuleffects.
The US government has made efforts in recent years to strengthen oversight over aid recipient compliance with the Helms Amendment. In May of 2025 the State Department launched a new scheme to ensure compliance with the Helms Amendment, which included training and individual attestations that staff were informed of the US’ government restrictions on abortion funding and that they understood the consequences for their organization if they were to violate those terms.
The terms outlined in the bilateral health agreements being signed and negotiated with the US government today escalate these compliance measures to include broad access to surveillance data without clear safeguards. In all agreements, failure to provide this access can result in “changes to planned assistance and/or discontinuation of the agreement,” meaning if they fail to comply countries could lose anywhere from US $124 million over five years in the case of Liberia to $1.8 billion in the case of Nigeria for HIV, TB, malaria, maternal and child health, laboratory systems, clinical commodities, and health workforce support that populations depend on for life-sustaining care.
By making a broad package of health aid contingent on broad and potentially invasive surveillance of Helms compliance, the agreement could encourage a more restrictive regulation of abortion than national law mandates and give rise to further violations of the right to health care. The Helms Amendment has previously been incorrectly interpreted as an absolute prohibition and a complete ban on abortion, without exception, including cases of rape, incest and/or risk to the life of the mother or fetus. This additional layer of surveillance may create pressure for administrators in countries like Mozambique, for example, that allows for abortion up to 12 weeks’ gestation, and up to 16 weeks in the case of risks to health of the mother or fetus, to effectively ban abortions altogether in violation of domestic law in order to avoid risking a loss of national health funding.
The Helms Amendment only applies specifically to the use of US funds for abortion care, unlike the “global gag rule,” which is a regulatory requirement that has been imposed through regulation under the Trump administration as well as past Republican administrations requiring foreign nongovernmental organizations receiving US global health assistance to certify that they do not use their own non-US funds for abortion. However, a lack of clarity and consistency in how these regulations are communicated, combined with the high stakes of health funding that could be lost if recipient countries do not provide the data requested by the US, could lead to overcompliance to avoid risking any loss of funds.
In the agreements with Mozambique, Rwanda, and Liberia, the countries commit to the provision of “any data” requested by the US to monitor compliance with the Helms Amendment without explicit privacy safeguards. The agreement with Uganda goes so far as to allow US officials to conduct unannounced spot checks at health facilities and clinics.
Nigeria’s agreement provides the U.S. Government with “regulated” data access for auditing purposes, but offers no clarity on the nature, scope and safeguards of this regulatory framework. Ethiopia’s includes in the preamble that “Participants affirm their right to protect personal data relevant to this MoU as provided in their domestic laws.” Kenya’s agreement stipulates that the audited information shared would be “subject to existing laws and regulations of Kenya and concurrence of the Office of Data Protection Commissioner.” Uganda’s agreement includes a broader stipulation that data activities under the MoU comply with the Data Protection and Privacy Act domestic and the National Data Governance Framework, which presumably would include data collected for Helms compliance monitoring.
Access to safe, legal abortion is a human right. Furthermore, research has shown that when abortion is banned or restricted, the number of abortions does not decrease. Abortions just move underground. This increases the risk both of unsafe procedures and that people who seek care will face criminal sanctions. The rate of unsafe abortions is nearly 45 times higher in countries with highly restrictive abortion laws than in countries where abortion is legal and unrestricted. By banning foreign assistance for abortion, the Helms Amendment contributes to the toll unsafe abortion has on the rights and lives of women in low- and middle-income countries.
Conditionality Puts Life-Sustaining Treatment at Risk
All seven agreements contain co-funding provisions that condition U.S. funding on meeting domestic health expenditure benchmarks, specific health outcome metrics like HIV-reduction targets, and demonstrating adherence to various other obligations, including Helms Amendment compliance. If partner countries fail to satisfy these conditions, the agreements give the US authority to reduce or cease funding, endangering critical health care services and medications for millions of people.
While co-funding and outcome requirements are standard in such agreements, the conditionality structures raise serious concerns. In no case do they adequately protect against sudden and harmful reductions in the availability and accessibility of health care that may negatively impact the effective enjoyment of the right to health, especially for marginalized groups. Nigeria’s agreement includes that the US will attempt “best efforts” to provide one year’s notice of any such reductions, while the Ethiopia, Rwanda, and Mozambique agreements require only “best efforts” to give 180 days’ notice. Nigeria’s agreement requires a mandatory joint review in the case of performance shortfalls before any co-financing adjustments are made. Uganda’s agreement includes the strongest procedural safeguards stating that funding adjustments would trigger a mandatory root-cause analysis, “should be a measure of last resort,” and subject to joint review by a Joint Health Steering Committee alongside a 180-day remediation process.
The Foundation for AIDS Research has additionally raised concerns that the metrics upon which funding is conditioned suffer from “fundamental flaws that ultimately undermine accountability and oversight.” In their assessment, the outcome metrics are too imprecise to be meaningful, process metrics are inconsistent and contradictory, performance provisions are ambiguous, and data confidentiality rules block independent oversight.
Long-term, Open-Ended Health Data Sharing
The agreements reveal significant gaps in the protection of health data. Six of the seven agreements require that governments negotiate broad data-sharing arrangements. Across the agreements, the scope, duration and legal safeguards governing these future data-sharing arrangements vary with key details deferred to subsequent negotiations. Only Mozambique’s agreement does not explicitly provide for a future data-sharing agreement but refers to US government’s plans to support a shared “health data exchange” and “health data record.”
The average lifespan of these agreements ranges from five to ten years, while Rwanda’s is for twenty-five years. The agreements signed by Liberia and Nigeria specify that the planned arrangements will incorporate elements of an “Appendix 5”, which is not included in the available text. The vague terms of the agreements mean there are reasonable concerns that health-related data to be shared could cover both individual-level and aggregate health data from national health information systems. This could also include sharing patient-level data such as HIV status, treatment adherence, viral loads, and maternal health records.
Uganda’s agreement expressly requires that data activities comply with the Data Protection and Privacy Act and the National Data Governance Framework, and Ethiopia’s includes in the preamble that data provided through the agreement is subject to personal privacy protections under domestic law. Kenya’s agreement is more limited, specifying that only information shared for audit purposes is subject to Kenyan law and concurrence by the Office of the Data Protection Commissioner, without extending these protections to the broader data-sharing agreements.
All seven agreements give the US the right to directly access data through audits to monitor compliance with US laws. Six of the agreements requires partner countries to provide the US government access to any data including on-site data and other information needed to conduct audits in up to five percent of randomly selected health facilities, clinics, labs, or programs identified by the US government, while Mozambique’s agreement require such audits up to four percent. Failure to comply with the requirement could result in the discontinuation of the agreement and withdrawal of aid.
In countries such as Liberia and Mozambique that lack binding comprehensive data protection laws, these provisions raise serious concerns about patient privacy where individuals may not receive any notice of data access or have meaningful ability to consent or seek redress.
The Committee on Economic, Social and Cultural Rights - the UN treaty body that monitors implementation of the International Covenant on Economic, Social and Cultural Rights - has affirmed that “the right to have personal health data treated with confidentiality” is a core component of the acceptability of health care, an element of the right to health. Overly broad information sharing conditions in these agreements may give rise to violations of these governments’ obligations to protect this right.
Biological Specimen and Pathogen Sharing without Benefit Sharing
The agreements with Rwanda, Ethiopia, Uganda, Nigeria, and Mozambique all reference unilateral specimen sharing arrangements as a condition of continued health funding. This means that these countries are committing to provide the US with “specimens, samples, sequencing data, and any other associated data related to novel and emerging infectious diseases with epidemic or pandemic potential.” The terms of the specimen sharing arrangements have not been made publicly available. However, according to a leaked draft template of the agreement, the US can then share the specimen and data with up to ten “non-U.S. Government U.S. entities” with the capability to develop diagnostics or other medical countermeasures. If countries fail to provide these resources, they could lose all funding included in the agreement. Only Uganda’s agreement includes protections against sudden termination of funding as a result of failure to share specimens.
The leaked draft template of the agreements indicates that there is no guarantee that countries will receive, in return, equitable access to diagnostics, vaccines, or treatments developed from their own biological resources in ways that maximize their availability and affordability.
The leaked template states that if a “medical countermeasure is developed primarily from specimen and related data shared under this Agreement,” then the US government will “prioritize” requests for the countermeasure by the government that shared the specimen and/or data after the US’ domestic needs and “subject to the availability of funds and the applicable law.” This means, essentially, that if diagnostics, vaccines, or treatments are developed based on biological resources or data provided by Rwanda, Ethiopia, Uganda, Nigeria, or Mozambique, for example, there is no guarantee that these countries will have access to them. As Emily Bass, a journalist and HIV/AIDS expert and activist, points out, an agreement to “prioritize” requests is essentially meaningless and the term “primarily developed” allows wide room for interpretation considering that medical interventions generally are developed from multiple inputs. The leaked template further states that the US will make “best efforts” to make the medical countermeasure available to the requesting country “at prices equal to or below those paid by the U.S. Government,” again, essentially making no commitments.
These provisions undermine the sovereign rights over biological resources and sequence information, recognized under the 1992 Convention on Biological Diversity. By conditioning foreign health aid on specimen-sharing obligations that flow exclusively to the US and up to ten non-government US private entities, with no reciprocal data access, no technology transfer, and no enforceable benefit-sharing, these agreements replace the Convention on Biological Diversity’s multilateral equity framework with an extractive bilateral arrangement.
It also goes against the principles of the 2010 Nagoya Protocol to the Convention on Biological Diversity. Parties to the Protocol are advised to take into consideration the need for expeditious access to genetic resources and expeditious fair and equitable sharing of benefits arising out of the use of such genetic resources, including access to affordable treatments by those in need, especially in developing countries. Rwanda, Mozambique, Nigeria, Kenya, Liberia, Ethiopia, and Uganda are all parties to the Nagoya Protocol.
These provisions also risk undermining the potential in ongoing discussions to develop an Annex to the 2025 WHO Pandemic Preparedness Agreement, which was adopted by WHO member states on May 20, 2025, to improve international coordination and cooperation on the prevention of, preparation for, and response to future pandemics. Core to the treaty was the creation of a Pathogen Access and Benefit-Sharing System (PABS), which will be overseen by the WHO and facilitate the equitable distribution of vaccines, therapeutics, and diagnostics to low- and middle-income countries for any pathogen that causes a pandemic emergency in exchange for these countries’ sharing access to pathogen data.
The 2001 Doha Declaration on TRIPS Agreement and Public Health affirms countries’ “right to protect public health and, in particular, to promote access to medicines for all” to prioritize public health over intellectual property protections. Specimen sharing agreements are good opportunities to incorporate intellectual property measures such that public health is prioritized. However, these bilateral agreements with the US miss this opportunity.
During the Covid‑19 pandemic, wealthy governments hoarded health technologies and blocked efforts to ease intellectual‑property rules while pharmaceutical companies refused to share technologies, leaving low‑ and middle‑income countries without timely access to lifesaving healthcare goods. These bilateral deals risk reinforcing some of those inequalities by forcing countries to surrender crucial pathogen data with no assurance they will be able to obtain the resulting health products.
Absence of Prevention and Community-Based Care
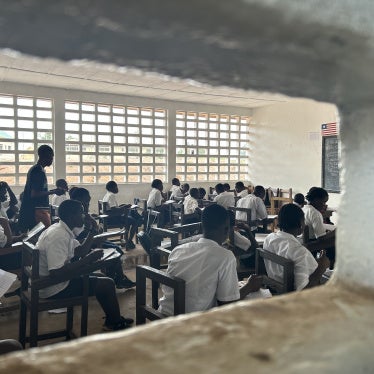
These bilateral agreements were negotiated after the government eliminated USAID in January 2025, which overwhelmingly impacted the community-based organizations doing outreach to the marginalized populations that are disproportionately burdened by new HIV infections. These bilateral agreements, which are meant to replace all US health aid to the aid recipient, were negotiated without the involvement of civil society partners or other major global health actors and directs aid only to the recipient government. This is in contrast to previous aid arrangements that included consultation with implementing partners and other multilateral actors like the Global Fund, and represented a range of aid recipients including governments and non-governmental organizations. Community-based organizations have often been the only access point to safe care for populations that face criminalization by their own governments, such as in Uganda or Nigeria, where same-sex conduct is punishable by life imprisonment in Uganda and up to 14 years imprisonment under federal law in Nigeria.
The new agreements do not fill the gap caused by USAID’s demise. While HIV/AIDS response is a central promise of the agreements, they do not include many of the key aspects of prevention and sustained care that are proven to be critical to controlling HIV, particularly the role of community-based outreach workers. The Mozambique agreement is a notable exception, referencing “community engagement and the long-term sustainability of civil society organizations in the HIV response” and commits to scaling up “combination HIV prevention interventions, with special consideration for vulnerable and high-risk population groups.”
Researchshows that for many LGBT people on the African continent, community-based organizations are the main source of care. Advocacy groups in Kenya and Uganda have raised concerns that the absence of efforts to include community-based organizations from the HIV response outlined in the agreements risks pushing LGBT populations into unsafe public health facilities where they might experience stigma and discrimination, or risk being reported to police, thus deterring them from seeking care altogether. Uganda Minority Shelters Consortium Coordinator John Grace described the sidelining of NGOs in the agreements as “deeply troubling,” warning that “without civil society participation there is a real danger of invisibility and neglect.” Essentially, governments that criminalize same sex conduct or persecute LGBT people, are unlikely to fund effective and safe community-based programs to help them.
Some agreements reference pre-exposure prophylaxis (PrEP) as a commodity line item but contain no accompanying commitments to ensure access for the populations who are most at risk of exposure, including men who have sex with men, sex workers, and people who inject drugs.
Mineral Access Concessions
While not made publicly available alongside the documents described above, the draft MoU with Zambia, which was leaked in March, explicitly linked US health assistance to parallel negotiations concerning US access to minerals in the country, underscoring the urgent need for transparency regarding the full set of conditions—explicit and implicit—that each of the health assistance agreements contain.
Zambia’s draft MoU, which it has not signed as of June 2026, contains an explicit cross‑conditionality provision (at Section 6.2), which would make the entire MoU contingent on Zambia’s agreement to, and implementation of, a separate document described as the “Bilateral Compact proposed by the U.S. Secretary of State to the Zambian President on November 17, 2025.” This separate bilateral agreement has also not been made public at the time of writing. However, the New York Times reported that it would require Zambia to undertake “significant reform of the governance of the minerals and other key sectors.”
A leaked draft of a memo prepared for Secretary of State Marco Rubio, first reported by the New York Times in March, outlined how US representatives had suspended negotiations on the health assistance MoU in December 2025 because Zambia wasn’t engaging on the separate bilateral compact concerning minerals, with the memo stating that US negotiators “needed to threaten or actually withdraw assistance important to [Zambia] to elicit progress on our priorities.” The memo further outlined how the US was preparing “the potential use of sticks” to encourage Zambia to agree to granting the US more access to the country’s minerals, including by “demonstrating willingness to publicly take support away from Zambia on a massive scale.”
This draft MoU with Zambia is subject to change and has not been executed by the parties. But the explicit incorporation of a separate, hidden agreement as a necessary condition for US health assistance means that, even if this draft were public and final, substantive obligations embedded within it would remain unknown to the public.
There is no publicly available evidence that similar agreements are being negotiated between the US and other countries. However, the draft Zambia MoU revealed US authorities’ willingness to use and withhold health assistance as a negotiation tactic to advance its material interests, which risks being replicated in other agreements, especially if they remain hidden from the public and opaque in terms.
Since the New York Times first reported on the hidden mineral-access components of the Zambia health MoU, the US government has only taken steps to further obscure the content of these agreements by suddenly removing the MoUs reviewed in this brief from the publicly available government website that had been hosting them only days before. Later, in April, a senior official in the US State Department’s Bureau of African Affairs spoke to a DC-based think tank and described the US’ strategy around these various bilateral agreements: “We call it commercial diplomacy. It means using our diplomatic engagement in the pursuit of commercial deals, infrastructure development and real economic outcomes.”
Without disclosure of all documents and terms that condition or constrain health assistance in these agreements, it is impossible for government officials not privy to these negotiations, affected communities, and civil society to adequately assess the scope and implications of those commitments, including whether they comport with human rights standards.
Nigeria’s agreement includes an additional provision that specimens shared will require approval by a “data and specimen governance committee on a case-by-case basis.”
Uganda’s MoU states that the “Participants are expected to meet as the JHSC [Joint Health Steering Committee] to conduct a root-cause analysis and develop a remediation plan by mutual decision. Funding adjustments by the U.S. government should be a measure of last resort and should be reviewed jointly and implemented in a phased manner to minimize system disruption if possible.”