
What is Trump’s “Mexico City Policy,” also known as the “Global Gag Rule”?
On January 23, 2017, United States President Donald Trump issued a Presidential Memorandum Regarding the Mexico City Policy. This order reinstates and dramatically expands the “Mexico City Policy” adopted under previous Republican administrations since 1984.
On May 15, Secretary of State Rex Tillerson approved a plan named Protecting Life in Global Health Assistance to implement this expansion. US law has banned using US foreign aid for abortion-related activities since 1973.[1] The Mexico City Policy is a separate rule that goes further, and requires foreign nongovernmental organizations receiving US global health assistance to certify that they do not use their own non-US funds to:
- provide abortion services,
- counsel patients about the option of abortion or refer them for abortion, or
- advocate for the liberalization of abortion laws.
This policy is also widely known as the “Global Gag Rule” due to the restrictions it places on how organizations use their own non-US government funds, including through limiting conversations that health providers can have with their patients and preventing them from pressing for legal change in their own countries.
Health assistance provided to recipients found to violate the rule can be terminated. A six-month review of the policy’s implementation did recommend providing more discretion to US government departments and agencies when there is a violation, if the recipient in good faith tried to comply with the rule. The standard provision has not been updated to reflect this recommendation.
What makes Trump’s version of the rule so much worse than previous versions, and why do health advocates say it will have a devastating impact?
Under previous Republican administrations, the restrictions in the Mexico City Policy applied specifically to US family planning funds, approximately US$575 million.
Trump’s policy extends restrictions to an estimated $8.8 billion in US global health assistance, including funding support for family planning and reproductive health, maternal and child health, nutrition, HIV/AIDS—including The President’s Plan for Emergency Relief for AIDS (PEPFAR),[2] prevention and treatment of tuberculosis, malaria (including the President’s Malaria Initiative), infectious diseases, neglected tropical diseases, and even to water, sanitation, and hygiene programs.[3]
The effects of the rule on these programs are still unknown but will most likely include the following profoundly damaging impacts:
- Because the US is the largest global donor on health, the rule is likely to undermine progress on improving health.
- Women and girls in about 60 low- and middle-income countries will have less access to contraception, resulting in more unintended pregnancies, and more—often unsafe—abortions.
- The restrictions will cause easily preventable maternal deaths, both due to unsafe abortion and to an increase in unplanned pregnancies in places where rates of maternal mortality are already high.
- Health programs that lose US funding may have to cut services linked to newborn, infant and child health, including vaccinations; prevention and treatment of HIV/AIDS, malaria, and tuberculosis (TB); and nutrition programs.
- The restriction makes needed health funds the instrument to curtail the speech and activities of activists and health providers in other countries, preventing them from sharing health information with patients about abortion or discussing potential reforms to abortion laws without losing their US funds.
What does the rule mean in practice?
For example, take the case of a foreign nongovernmental organization receiving 50 percent of its funds from non-US sources to provide sexual and reproductive health services, including counseling, referrals, or services related to abortion, and the other 50 percent from the US to provide vaccinations for babies, nutritional supplements, or treatment for HIV/AIDS, malaria, and TB. Under this rule, that group must now choose between losing its US funding—slashing its operating budget in half—or restricting or cutting its reproductive health programs. Those that comply with the restrictions must also set aside some of their resources to meet additional compliance and reporting requirements.
Either way, health services in under-resourced communities will suffer. In many places, organizations affected by the rule are the only source for some of these services.
What has Human Rights Watch research found on the impact of the 2017 rule?
In July 2017, Human Rights Watch interviewed representatives of 24 organizations in Kenya and 21 in Uganda affected by the funding restrictions.[4] Both countries rely heavily on US health funds to combat high maternal mortality rates and the HIV/AIDS epidemic.
Human Rights Watch found the policy has triggered reductions in key sexual and reproductive health services from well-established organizations that cannot easily be replaced. For example, Family Health Options Kenya (FHOK) runs 16 healthcare facilities in the country. FHOK representatives told us the organization will not comply with the restrictions and therefore will lose US funds, which make up roughly 60 percent of its budget, and that it may have to cut as many as half of its services. By July 2017, the organization had already closed one clinic and canceled 100 planned outreach events, including for cervical cancer screening, HIV testing, and family planning counseling, that typically reach 100 people each time.
Another organization, Reproductive Healthcare Network Kenya has lost about two-thirds of its funding and has canceled many activities, including trainings on safe abortion care for doctors and other healthcare providers. Reproductive Health Uganda, which serves 1.2 million people a year, is ending large health programs previously paid for by the US government.
Although governments receiving US funds are exempt from the policy, Human Rights Watch found that many government health clinics will be indirectly weakened. In Kenya, where the law permits abortions for health reasons, many depend on nongovernmental groups for training and equipment to provide safe abortion care, including in cases of rape or incest, or to save a woman’s life.[5]
In Uganda, some health advocacy groups and service providers—representing a diverse range of constituencies and issues—will have to leave a coalition working to end maternal mortality because of unsafe abortion in order to preserve their US funding.
In its six-month review, the State Department does recommend revising standard provisions that clarify that recipients of technical assistance or training that are not awardees or sub-awardees are not subject to the policy. But the standard provisions have not been revised accordingly.
Interviews with sex worker organizations that have come up for funding renewal illustrated that they had to make cruel programmatic choices, including choosing between funds for lifesaving antiretroviral therapy for their members or lifesaving reproductive health services.[6]
Human Rights Watch found considerable confusion about the policy. Health organizations had many questions about the scope and implementation of the policy; and about access to US government-funded equipment and supplies. In the absence of more detailed guidance, some organizations appeared to have interpreted the policy’s restrictions too broadly—for example, feeling they should avoid community outreach on the risks of unsafe abortion.
The State Department has stated that its programs, USAID and Health and Human Services, have invested in extensive outreach and training about implementing and monitoring the policy, with more than 5,000 people trained. These agencies have also developed tools for award recipients to monitor compliance with the policy.
Why is sexual and reproductive health care so important?
Women and girls have a human right—protected under international law—to make their own choices about whether and when to have children, and about how many children they have. Unintended pregnancies can affect a range of other rights, including by ending a girl’s education, contributing to child marriage, resulting in health complications, or putting a woman’s life at risk.
- An estimated 225 million women in developing countries would like to prevent or delay pregnancy but are not using contraception. Among the main reasons are limited access to contraception and poor quality of available services.
- Complications from pregnancy and childbirth are the second leading cause of death for adolescents ages 15 to 19 globally.
- More than 800 women and girls die globally from preventable causes related to pregnancy and childbirth every day, including unsafe abortions.
- The World Health Organization estimates that at least 22,000 women die from abortion-related complications every year.
What do we know about the impact of previous versions of the Global Gag Rule?
Under previous versions of the Global Gag Rule, organizations that chose to continue work that meant the loss of their US funding had to cut staff, services, and sometimes to close clinics. On the other hand, health providers in organizations that complied with the restrictions to keep their US funds have talked about being “gagged” from providing full and accurate information to patients and advocating for changes to restrictive abortion laws.
For example, in 2009 Human Rights Watch found that the rule affected funding to Peru for maternal health because it did not permit funding for organizations that used it to provide information about or to provide what is known in Peru as therapeutic abortions—to preserve the health of the mother or for fetal abnormalities incompatible with life. A new Kaiser Family Foundation study found that nearly 40 countries receiving US global health assistance permit legal abortion in at least one instance not permissible under Trump’s rule.[7]
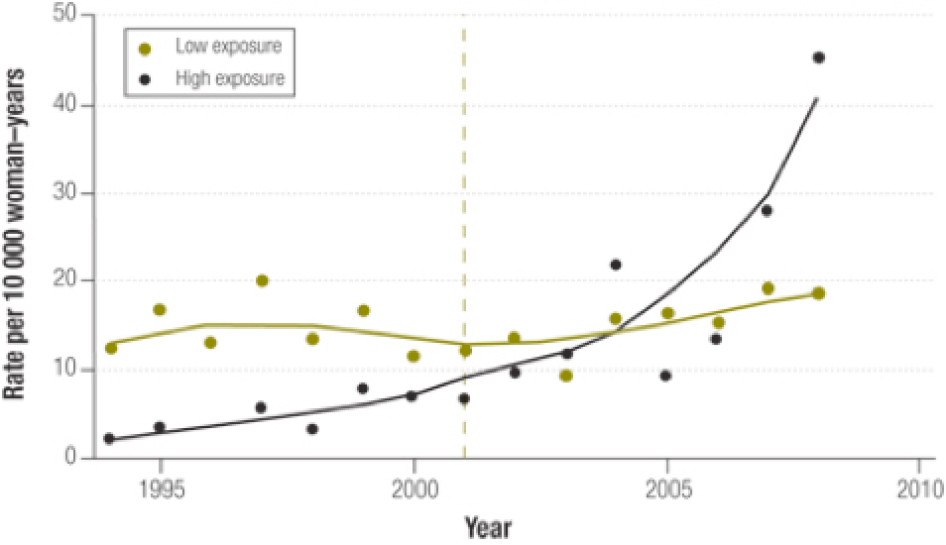
Restricting family planning funds results in unplanned pregnancies, abortions, and maternal deaths. A Stanford University study examined detailed national survey data in 20 countries in sub-Saharan Africa between 1994 and 2008. It found that countries most affected by the Global Gag Rule had significantly increased rates of induced abortions whereas the rates remained relatively stable in countries less affected by the policy.[8]
The six-month review released by the State Department provides no indication that it will be tracking these unintended consequences of the policy.
Are there exceptions?
Trump’s Mexico City Policy will not apply to humanitarian assistance, including State Department migration and refugee assistance, or Defense Department disaster and humanitarian relief activities. However, the Trump administration defunded the UN Population Fund (UNFPA), which provides key family planning and maternal health care services in humanitarian settings. The US provided $69 million, $38.3 million of which was directly targeted for humanitarian emergencies, and was one of the agency’s largest donors.
Other exceptions include basic health research, a program for schools and hospitals abroad, and Food for Peace programs. Under the State Department interpretation, the policy will apply to implementation-science research, operational or programmatic research, surveys, needs assessments, and related capacity-building conducted for the purpose of improving programs.
There is an exception for abortion services, counseling, or referrals in cases of life endangerment, rape, or incest, and for post-abortion care. This includes treatment of injuries caused by legal and illegal abortions. These exceptions were also in place under previous versions of the Global Gag Rule but were not widely known, understood, or acted upon. Passive referrals—defined in the standard provisions as providing a response to a specific question from a pregnant woman who has already decided she wants an abortion about where a safe, legal abortion can be obtained may also be made when medical ethics require it.
When and how did the Global Gag Rule go into effect?
The implementation plan for the policy went into effect on May 15, 2017. Implementation will have a rolling impact on programming. A “standard provision” that outlines the restrictions will be included in all new grants, cooperative agreements, and grants under contracts, or during amendments to existing funding agreements.
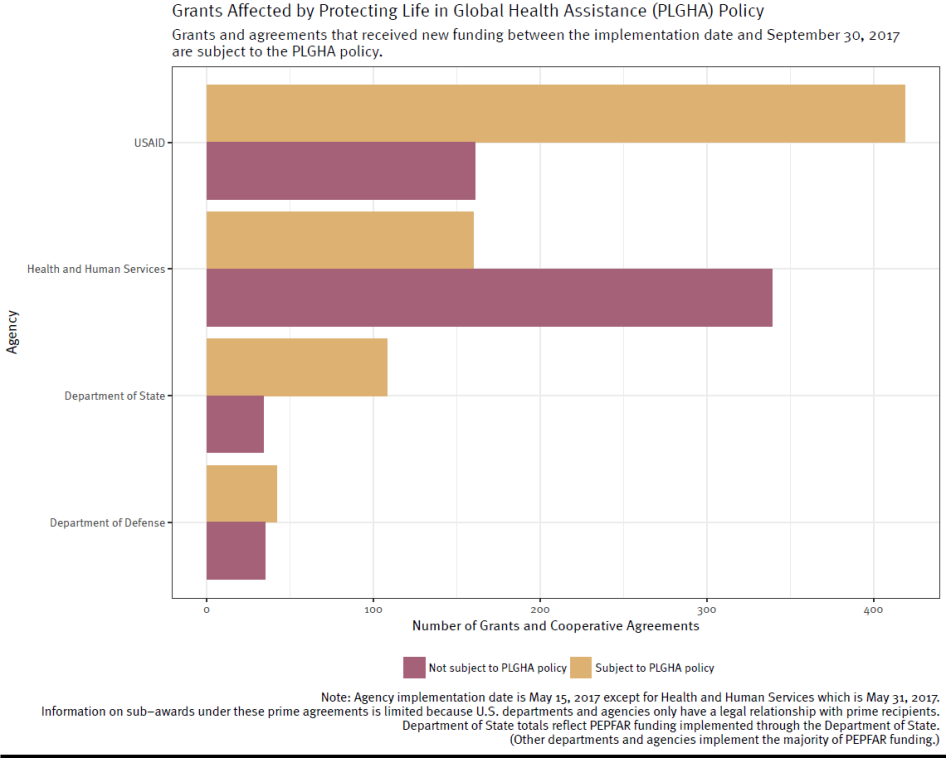
According to the State Department’s six-month report, the majority of grants and agreements as of September 30, are subject to the rule—with that number expected to increase. The report notes that three prime recipient organizations, and 12 sub-awardee organizations have chosen not to certify compliance and have lost funding.
The policy will also apply to organizations awarded funding through contracts. However, an interagency group is still developing rules for carrying out the changes, which must go through a rule-making process and is still under development by an interagency group.
Is the US State Department monitoring the impact of the policy?
On February 7, the US State Department released a “six-month review” of the implementation of the policy. However, as the State Department notes in its report, six months is not long enough to sufficiently assess this policy. Many organizations have not yet or just recently signed new grants or renewals. The State Department in its February 8 report notes that “the picture on progress and challenges is still developing.” Furthermore, the State Department’s review of the policy seems tailored toward monitoring implementation and less directly monitoring the impact of the policy on women’s and girls’ health, which in many cases will take years to monitor and understand.
The February report does acknowledge the need for follow-up analysis, in direct response to third-party stakeholder organizations’ concerns that “six months is insufficient time to gauge the impact” of the policy. It has recommended a further review of the implementation of the policy by December 15, that more thoroughly examines the “benefits and challenges” of the policy.
What can be done?
One priority is for foreign governments, multilateral institutions and foundations to narrow the funding gap for comprehensive sexual and reproductive health services and support groups that provide such services, including safe and legal abortion. In effect, Trump’s Global Gag Rule will produce a funding gap for some organizations that provide the highest quality services in some of the most under-resourced communities and countries. The funding gap left by the US, the world’s largest donor of health assistance, to these highly qualified providers, will be almost impossible to fill, but increasing and diversifying funding from other sources will be life-saving.
Some governments have stepped up to publicly pledge increased support for sexual and reproductive health and rights that do not place restrictions on abortion. For example, the Dutch government has created an international funding initiative to support groups affected by the Global Gag Rule called “She Decides.” An inaugural summit hosted by Belgium, Denmark, the Netherlands, and Sweden on March 2 resulted in pledges of roughly $190 million.
The US government agencies affected by the rule should monitor the impact of the policy on women’s and girls’ health and not just look at data on service delivery disruption. While the State Department recommended an additional review by December 15, the US government should continue to monitor the impact of the policy while it is in place. Congress should mandate an annual, rigorous, and public review as well as hold hearings on the impact. Members of Congress should also invite affected organizations to speak with them, and, when they travel overseas, members and staff should take time to meet with organizations that have been negatively impacted by the policy.
As a longer-term strategy, stability is needed in US global health assistance. It is disruptive and counterproductive to the global health community to have the US policy on foreign assistance change dramatically from one presidential administration to the next. Draft legislation in the US—called the Global HER Act—would permanently repeal the Mexico City Policy (Global Gag Rule). While it is highly unlikely to be adopted under the current Congress and endorsed by the administration, it has been gathering increased support and could be pursued as a long-lasting solution down the road.
[1] The 1973 “Helms Amendment” to the Foreign Assistance Act prohibits the use of US funds from paying “for the performance of abortion as a method of family planning.”
[2] The President’s Plan for Emergency Relief for AIDS (PEPFAR) is the US government’s initiative on HIV/AIDS, and is the largest component of the President’s Global Health Initiative.
[3] The rule applies to all household and community-level water, sanitation, and hygiene programs, but exempts water and sanitation infrastructure spending in some household settings, schools, health facilities, commercial use, and national policy development activities.
[4]Letter from Human Rights Watch to US Secretary of State Rex Tillerson “Re: Early Impact of the Protecting Life in Global Health Assistance Policy in Uganda and Kenya”, October 13, 2017, https://www.hrw.org/news/2017/10/26/re-early-impact-protecting-life-global-health-assistance-policy-kenya-and-uganda.
[5] Skye Wheeler, “The Devastating Domino Effect of the Global Gag Rule in Kenya”, News Deeply: Women and Girls, December 7, 2017, https://www.newsdeeply.com/womenandgirls/community/2017/12/07/the-devastating-domino-effect-of-the-global-gag-rule-in-kenya (accessed December 15, 2017).
[6] Skye Wheeler, “Cruel Choices: How Trump’s Gaga Rule Hurts the Fights Against HIV”, Women’s E-News, December 7, 2017, http://womensenews.org/2017/12/cruel-choices-how-trumps-global-gag-rule-hurts-the-fight-against-hiv/ (accessed December 15, 2017).
[7] Kaiser Family Foundation, “What Is the Scope of the Mexico City Policy: Assessing Abortion Laws in Countries That Receive U.S. Global Health Assistance,” May 3, 2017, http://kff.org/global-health-policy/issue-brief/what-is-the-scope-of-the-mexico-city-policy-assessing-abortion-laws-in-countries-that-receive-u-s-global-health-assistance/#endnote_link_215568-5 (accessed June 2, 2017).
[8] Eran Bendavid, Patrick Avila, and Grant Miller, Stanford University, “United States aid policy and induced abortion in sub-Saharan Africa,” Bulletin of the World Health Organization 2011;89:873-880C, http://www.who.int/bulletin/volumes/89/12/11-091660/en/ (accessed June 2, 2017).
[9] Ibid. Exposure to the Mexico City Policy was classified as high or low according to whether the level of per capita financial assistance provided to the country for family planning and reproductive health by the United States was above or below the median for the period from 1995 to 2000. The dashed vertical line indicates the year the Mexico City Policy was reinstated. The two curves were generated from observational data using the locally weighted scatterplot smoothing (lowess) method.









