(Beirut) – Restrictions on aid deliveries from Damascus and Iraq are preventing medical supplies and personnel needed to prevent, contain, and treat Covid-19 from reaching two million people in northeast Syria, Human Rights Watch said today. On April 17, 2020, the authorities in northeast Syria announced the first confirmed Covid-19-related death.
The United Nations Security Council should immediately reverse its January decision to end its authorization of moving UN aid supplies from Iraq to northeast Syria. Since January 2020, non-UN aid groups that previously depended heavily on the UN for health care supplies have been unable to deliver enough aid from the Kurdistan Region of Iraq to northeast Syria. Syrian authorities in Damascus, the capital, should also reverse their longstanding restrictions on aid reaching Kurdish-held areas in northeast Syria and allow medical supplies and personnel into the region.
“Two million people are stuck in northeast Syria without the tools to tackle outbreaks of Covid-19,” said Gerry Simpson, associate crisis and conflict director at Human Rights Watch. “As the number of infections rise, global and regional leaders should urgently act to allow lifesaving medical supplies and staff to reach those in desperate need of support.”
Between March 31 and April 21, Human Rights Watch interviewed 10 aid workers and officials from UN agencies and international nongovernmental organizations operating or supporting operations in northeast Syria about the obstacles they faced in responding to Covid-19 there. Human Rights Watch sent questions on April 22 to the Syrian government and the Kurdish Regional Government (KRG) in the Kurdistan Region of Iraq about those obstacles. On April 27, the KRG replied, saying that between March 1 and mid-April, it had approved all requests by nongovernmental organizations to deliver medical assistance to northeast Syria.
As of April 25, the authorities in Damascus had tested 48 samples from northeast Syria, of which 1 tested positive. The area is mostly under the control of the Kurdish-led Autonomous Administration, a quasi-autonomous authority. By April 25, Syrian authorities had confirmed 42 cases countrywide. Syria’s limited testing capacity, especially in northeast Syria, means the real number may be much higher. The authorities in Damascus have refused to collect some Covid-19 test samples from northeast Syria for testing, and it took two weeks before the northeast authorities found out in mid-April about the first positive test result on April 2.
Nine years of conflict have decimated Syria’s infrastructure and social services, including for health care, resulting in massive humanitarian needs and leaving the population, including about 6 million internally displaced people, vulnerable to a Covid-19 outbreak.
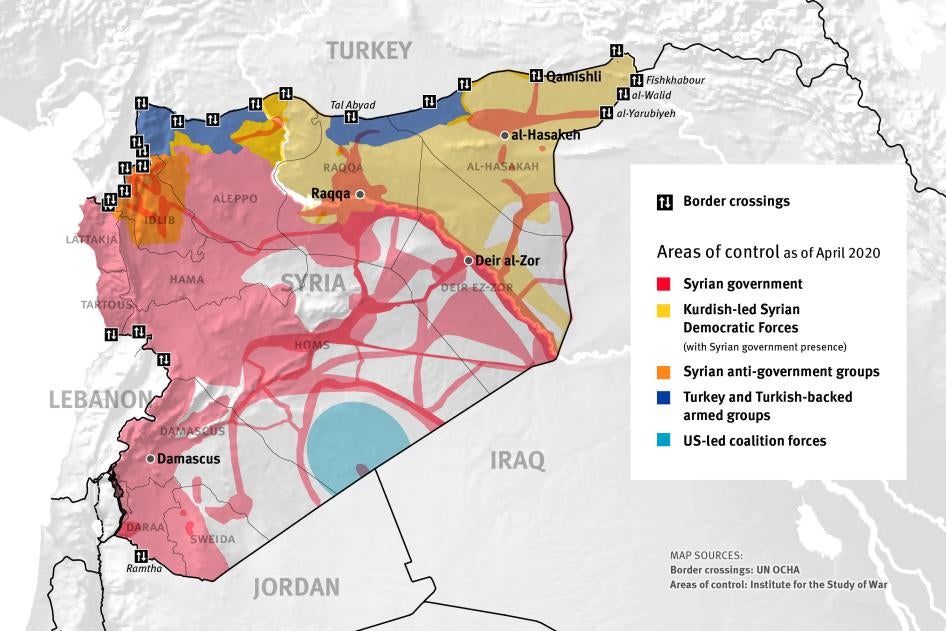
Until January, the UN Security Council allowed UN agencies to transport aid from northern and other parts of Iraq to northeast Syria through a single border crossing, from Rabia, in Iraq, to al-Yarubiyah, in northeast Syria. It was mainly used by the World Health Organization (WHO) to supply the region with medical aid.
Al-Yarubiyah is one of four border crossings the UN Security Council authorized in a 2014 resolution, which has allowed the UN and other aid agencies to deliver aid to northeast Syria through Iraq, to northwest Syria through Turkey, and to southern Syria through Jordan. Although some diplomats and experts believed such authorization unnecessary, the Security Council adopted this approach to address the Syrian government’s persistent refusal to give the UN and other aid agencies explicit permission to supply areas not under government control with aid.
However, responding to Russia’s threat to veto the mandate, on January 10, the Security Council officially removed al-Yarubiyah and Ramtha, a crossing point on the Jordan-Syria border, from the list of authorized border crossings, halting all UN cross-border aid into northeast and southern Syria. Aid workers said this has resulted in a US$40 million shortfall for 2020 for nongovernmental organizations depending on UN support for their operations in northeast Syria, including $30 million for health care, mostly to prevent and respond to Covid-19.
Until mid-March, international aid groups in the Kurdistan Region of Iraq that previously sourced almost all their medical supplies for their operations in northeast Syria through the WHO continued to transfer limited aid and staff to northeast Syria through other border crossings. Since then, however, aid officials say the KRG has introduced restrictions that have limited the amount of aid they can take to northeast Syria. These include banning agencies from buying medical supplies in the Kurdistan Region of Iraq that are destined for export to northeast Syria to prevent and treat Covid-19 there and a lack of clarity relating to organizing cross-border transfers.
Aid workers who spoke to Human Rights Watch and statements by Kurdish officials in northeast Syria said that despite some air shipments in March and April from Damascus to Qamishli, in government-held northeast Syria, bureaucratic obstacles in Damascus are preventing aid agencies from transferring supplies to nongovernment-held parts of the region.
Several aid workers from organizations registered in Damascus and UN agencies said that the combination of restrictions from Damascus, the KRG, and the Security Council has prevented them from preparing for an outbreak of Covid-19 in northeast Syria. In mid-April, the UN said that “the absence of a laboratory capacity in NES [northeast Syria] coupled with transport delays and access challenges, hinders the timely testing of suspected cases.”
The situation in northwest Syria is just as bad or worse, with the almost-complete decimation of the region’s health care infrastructure, severe overcrowding in areas sheltering displaced civilians, and the threat of continued hostilities. The health care sector has severe shortages of equipment needed to tackle a Covid-19 outbreak. However, there the UN has set up coordination hubs and continues to use the UN Security Council’s cross-border authorization from Turkey to ensure that agencies can bring in at least some medical supplies.
Under international law, Syria has an obligation to realize the entire population’s right to health. Although limited resources and capacity may mean that these rights can only be fully realized over time, the authorities are still obliged not to discriminate between different parts of the population, and they must justify any aid delivery limitations. Under international humanitarian law, consent to allow relief operations cannot be withheld on arbitrary grounds. All parties to an armed conflict and other relevant states must also allow and facilitate rapid and unimpeded passage of impartial humanitarian assistance for civilians in need.
Given the speed with which Covid-19 overtakes even the most sophisticated health systems, the UN Security Council should immediately reauthorize cross-border aid operations from northern Iraq into northeast Syria through al-Yarubiyah. This would allow the WHO to assess and scale-up its support to the region, including by resuming supplies and funding to international aid groups based in northeast Syria under the Covid-19 Global Humanitarian Response Plan and the Syria Cross-Border Humanitarian Fund. The Council should also authorize additional crossings based on the recommendations of UN and other humanitarian agencies.
International donors should also press the Syrian authorities and the KRG to facilitate the transfer of health care and other aid into all of northeast Syria and not to block access on arbitrary or discriminatory grounds, including through undue bureaucratic delays.
“As even the most advanced economies struggle to combat Covid-19, governments around the world should be pulling together to immediately let emergency aid flow to millions at risk in conflict-torn regions,” Simpson said. “Neither the UN Security Council nor the Syrian authorities should be waiting for a potentially catastrophic outbreak in northeast Syria before taking action to prevent more unnecessary deaths.”
Covid-19 and Health Care, Water Supply in Northeast Syria
As of late February, almost half of northeast Syria’s 4 million inhabitants needed humanitarian assistance, including 1.34 million – almost 500,000 of them displaced people – in nongovernment-held areas. According to the UN and interviews with aid agencies, half of the displaced do not have sufficient access to services including health care, water, sanitation, and shelter. About 100,000, including 44,000 children, live in abysmal conditions in camps that shelter mostly people displaced from territory previously held by the Islamic State (also known as ISIS) in Iraq and Syria. Aid agencies have developed a Covid-19 awareness campaign plan in camps and collective shelters.
The region’s health care system, run by the Kurdish-led Autonomous Administration for northeast Syria, has been heavily affected by nine years of conflict and Turkey’s October 2019 military offensive. As of mid-April, only 26 out of 279 public health care centers are fully functioning. Aid agencies say that only 2 of 11 hospitals are fully functioning and that no district in northeast Syria meets the minimum emergency threshold of at least 10 beds for every 10,000 people, while just 1 district has enough doctors, nurses, and midwives to meet the minimum emergency threshold of at least 22 health care workers for every 10,000 people. Almost all of the region’s 35 intensive care unit beds are in al-Hasakeh province, with only a few in the two remaining provinces of al-Raqqa and Deir al-Zor.
Aid workers said that the Kurdish authorities in the northeast do not have their own public health monitoring and testing system. To respond to the lack of testing kits for Covid-19, in March, the health authorities in northeast Syria repurposed test kits designed for other diseases such as polio and HIV.
On April 15, the WHO said that among the 1,500 Covid-19 tests carried out by the authorities in Damascus, 48 were of samples collected from the northeast, one of which tested positive. The actual number of cases is likely much higher, due to the lack of available testing in the northeast. On April 10, the KRG facilitated the transfer of two testing machines and 1,500 test kits to the Autonomous Administration in northeast Syria. Since then, the Administration has received three more machines and as of April 23, a further two were in transit.
Aid workers operating in northeast Syria told Human Rights Watch that the region lacks a wide range of advanced and basic medical supplies, including those needed to prevent a Covid-19 outbreak. One aid agency has said that “the few functional medical facilities in the region could very quickly become overwhelmed with an influx of Covid-19 patients” and that the lack of supplies and staff has forced several facilities to close, “leaving patients with chronic disease and compromised immune systems even more vulnerable to Covid-19.”
Health experts have concluded that the region has the capacity to deal with a little under 500 Covid-19 cases and possibly fewer, depending on the speed and severity of the outbreak. On April 25, the UN said that health authorities and nongovernmental organizations are setting up a number of isolation centers in government-held areas and non-government-held areas of northeast Syria. Informed sources in Damascus said that northeast Syria has 10 adult ventilators, 1 pediatric ventilator, and only 2 doctors trained to use them.
Since October, Turkey and Turkish-backed forces have controlled the Allouk water station near the town of Ras al-Ain (Serekaniye) in northeast Syria. It supplies 460,000 people in the region’s al-Hasakeh governorate, including al-Hasakeh City and 3 displacement camps. Aid workers said that the Turkish authorities have interrupted water pumping several times since the start of the year, most recently for a few days in late March.
The Turkish authorities’ failure to ensure adequate water supplies to Kurdish-held areas in northeast Syria has also affected aid agencies’ ability to protect vulnerable communities in the event of a Covid-19 pandemic because strict personal hygiene, including frequent handwashing, is critical to prevent the spread of the disease. Aid agencies say they have prioritized raising awareness about the importance of washing hands, but the repeated interruptions to the water supply have made it hard for them to encourage even this basic measure.
Impact of UN Security Council Action on Aid through Northern Iraq
Between 2014 and early January 2020, the UN Security Council authorized UN agencies – WHO, the UN Children’s Fund (UNICEF), and the UN Population Fund (UNFPA) – and their implementing partners to deliver health care-related and other aid to northeastern Syria through northern Iraq’s al-Yarubiyah border crossing without requiring the Syrian government’s permission. Due to security concerns, the UN’s cross-border operations only started in April 2018.
Since then, UN agencies and international nongovernmental organizations have formally supported northeast Syria, including its health care sector, by taking in much-needed aid and personnel. Aid agencies told Human Rights Watch that throughout 2019, their health care programs in northeast Syria heavily depended on supplies from the WHO taken in through the Yaribuyah border crossing.
The UN secretary-general’s February 2020 report on cross-border aid from northern Iraq to northeast Syria also said that in 2019, only a limited number of health care facilities in northeast Syria received supplies through Damascus and that most relied heavily on supplies from the UN in Iraq, delivered through the Yarubiyah crossing.
However, Russia – with China’s support – vetoed a renewal of the entire cross-border aid mandate in December, contending that it was no longer necessary as those areas were now under the Syrian government’s control and could be reached from Damascus and that aid had been previously taken by “terrorists.” Moscow again threatened to veto the entire mandate in January, demanding that the UN Security Council strike al-Yarubiyah and al-Ramtha, a crossing point on the Jordan-Syria border, off the list of authorized border crossings as they were “totally irrelevant because humanitarian assistance to that region is coming from within Syria.”
On January 10, the UN Security Council passed Resolution 2504 which ended authorization for using two of the four border crossings – al-Yarubiyah and al-Ramtha – authorized in its previous resolutions on cross-border aid into Syria. The resolution reauthorized the other 2 crossing points, between Turkey and northwest Syria, for only 6 months, compared to 12 months in previous cross-border aid resolutions on Syria.
Since then, UN agencies, including the WHO, have stopped supplying aid to northeast Syria from northern Iraq, and international aid groups are unable to receive UN financial support, including through the Covid-19 Global Humanitarian Response Plan and the Syria Cross-Border Humanitarian Fund. Aid workers said that the resulting total funding gap for 2020 will be about $40 million. This includes about $30 million for health funding and supplies, due to the loss of $7.5 million previously pledged and $23.6 million they had expected to receive for their Covid-19 response, had the Yarubiyah crossing remained open, and a further $10 million previously pledged in non-health care support. One aid agency said that this will result in health care service disruption, including closing facilities.
Aid workers in northeast Syria said that the KRG has allowed them for a number of years to use border crossings between the Kurdistan Region of Iraq (KRI) and northeast Syria to deliver some aid, including health care supplies and personnel, which continued between mid-January and early March. Aid workers said that on March 1, the Autonomous Administration in northeast Syria closed its border with the KRI but authorized aid agencies in KRI to continue to enter northeast Syria so that the border closure on the Syrian side did not affect their cross-border operations from Iraq.
However, they say that restrictions gradually imposed during the first half of March by the KRG to prevent the spread of Covid-19 in the KRI made it more difficult to continue to scale-up their medical response in northeast Syria. The restrictions involved only allowing agencies to take supplies and staff to northeast Syria once a week and banning agencies from buying medical supplies needed to prevent and treat Covid-19 that are destined for export to northeast Syria, including personal protective equipment, in Erbil, the region’s capital, and other cities.
The aid workers said that a global scarcity of Covid-19-related medical supplies, including protective equipment, has also affected their operations in northeast Syria as they cannot get supplies from outside the region in sufficient amounts and at a non-prohibitive cost. Agencies said that despite improved authorization procedures introduced in mid-April, they do not know whether the authorities will allow them to import Covid-19-related supplies into the Kurdistan Region of Iraq – as opposed to buying them locally – and transport them to northeast Syria.
Aid agencies also said that on March 17, the KRG introduced movement restrictions between towns and cities, including Erbil and Dohuk, near the Syrian border, although it exempted the international aid agencies. However, on March 18, the KRG closed the main crossing point that the groups were using to take aid to northeast Syria because of storm damage. They also ended the previous arrangement of allowing aid agency staff and supplies to cross once a week to northeast Syria.
Since March 18, the KRG has not put in place clear authorization procedures, government offices have been mostly closed, and it has taken a lot of effort to negotiate permission to take occasional supplies to northeast Syria, which happened twice, on March 31 and on April 15, aid agencies said. As a result, aid agencies have had to keep critical health care aid, including for Covid-19 preparedness and response, in their warehouses in Erbil. They say the border restrictions have limited their response in northeast Syria, resulting in a severe shortage of personal protective equipment and supplies to prevent and control infections, including basic materials such as hand sanitizer, and that 71 health facilities in northeast Syria are affected.
Aid agencies also say that on April 15, the KRG announced that it would automatically allow aid agencies to transfer supplies relating to health care, water, sanitation, and food and cash distribution programs to northeast Syria. The KRG also said it would approve the transfer of supplies for other aid sectors, including agriculture, on a case-by-case basis. However, aid agencies say that since April 15, they have continued to negotiate at length with authorities each time they wish to transfer medical supplies and staff northeast Syria.
On April 27, the KRG responded to a summary of Human Rights Watch’s findings. In its reply, the KRG said that on March 1, the Autonomous Administration in northeast Syria had closed the main border crossing aid agencies in KRI had been using to transfer supplies and staff to northeast Syria as a precautionary measure to prevent the transmission of the coronavirus to northeast Syria. The KRG also said that on an unspecified date after March 1, it had authorized aid agencies to cross to northeast Syria once a week with Covid-19-related humanitarian aid and that between March 1 and April 15, ten tons of medical supplies had crossed to northeast Syria.
The KRG said that since then, aid agencies have had to continue to request permission for each shipment of health care supplies. Finally, the KRG said that aid agencies cannot purchase Covid-19-related supplies in the KRI for export to northeast Syria because the KRG has a shortage of materials to treat people in KRI, but that if aid agencies import such supplies, they can transfer them to northeast Syria.
Non-UN aid workers Human Rights Watch spoke with said that even if they could resume the level of cross-border work they carried out until early March, they would not be able to adequately respond to a Covid-19 outbreak alone. They said that the UN agencies, including the WHO, are essential to coordinating a large-scale response and to reliably guaranteeing a sufficient amount of supplies, as the response requires coordination hubs and independent supply chains.
This is echoed by the UN secretary-general’s February 2020 report on cross-border aid, which concluded that unless an alternative was found, “by May … there is likely to be a broad … gap in basic medicine in medical facilities previously supplied by the UN cross-border operation.”
The same report proposed the Akçakale-Tel Abyad border crossing between Turkey and northeast Syria as a possible alternative to al-Yarubiyah. However, since October 2019, Turkish-backed Syrian national army factions control Tal Abyad and are unlikely to allow aid to be delivered from the city to areas held by the Kurdish-led administration in northeast Syria. Turkey views the administration as indistinguishable from the armed Kurdistan Workers’ Party (PKK), with which Turkey has been engaged in a decades-long conflict in southeast Turkey and across its border in the KRI.
Syrian Authorities’ Restrictions on Aid from Damascus
UN Security Council Resolution 2165 of 2014, authorizing cross-border operations without Damascus’ permission, reflected the international community’s recognition of the Syrian government’s “arbitrary and unjustified withholding of consent to relief operations and the persistence of conditions that impede the delivery of humanitarian supplies to destinations within Syria.” In June 2019, Human Rights Watch reported that the Syrian government’s legal and policy framework allows for diverting aid and the discriminatory distribution of essential supplies.
Aid workers interviewed said that since January, their organizations have continued to face significant longstanding obstacles in transporting materials and personnel from Damascus to nongovernment-controlled areas of northeast Syria.
Two aid agencies said that as of early April, the Syrian authorities had sent none of their 1,200 Covid-19 sample collection kits to nongovernment-controlled areas in the northeast.
In March, Rapid Response Team staff from Syria’s Health Ministry collected samples that had been taken from patients in the northeast using repurposed test kits and took them to the Central Public Health Laboratory in Damascus for testing. Representatives of the northeast authorities, as well as one well-informed aid worker, said that Damascus had initially refused to test the samples, but a high-level international official intervened and pressured the authorities to allow the testing.
According to an official in the Health Directorate of the Autonomous Administration in northeast Syria and an aid worker, Syrian authorities in Damascus have also refused to give some Rapid Response Team staff permission to collect samples from northeast Syria, in one case blocking a planned sample collection from al-Hasakeh National Hospital on the grounds that one of the aid agencies working there is banned by the Syrian authorities from operating in government-held areas.
According to the UN, on March 29, the Central Public Health Laboratory in Damascus tested a sample that had been collected two days earlier in Qamishli in northeast Syria. An aid worker said that on April 2, the laboratory confirmed that the sample had tested positive for Covid-19 and the authorities announced the test result as part of the countrywide new case total that same day. The patient died the same day in Qamishli National Hospital. However, the authorities took 3 days to inform the WHO that 1 of the cases had originated in the northeast and it took them a further 11 days to inform the Qamishli National Hospital. An aid worker said that the same day, a WHO nongovernmental partner organization informed the Autonomous Administration in the northeast of the test result. On April 17, the Syrian Democratic Forces (SDF) in northeast Syria announced the test result and criticized the WHO and the Syrian government for failing to inform them earlier.
A media report said that Damascus agreed in early April to allow tests in the government-controlled part of Qamishli in northeast Syria, but as of mid-April, this had not been put in place. According to the UN, the Syrian government has approved new testing laboratories in Lattakia, Homs, and Aleppo, but not in al-Hasakeh or Deir el-Zor.
Aid agencies also said that they have to obtain permission from the Syrian authorities in Damascus for each staff member and shipment of supplies traveling from Damascus to northeast Syria. They said that often the authorities do not respond to their requests and that if they do, it can take up to several months. They said that if they finally obtain permission, the movement may be cancelled at the last minute due to security concerns. If they are finally allowed to move staff or supplies, bureaucratic hurdles often delay them further as they try to leave government-controlled areas.
The UN secretary-general’s February 2020 report also describes a range of bureaucratic obstacles between Damascus and northeast Syria in 2019 and early 2020 that makes the “crossline delivery of medical items … particularly restrictive.” These include Syrian government approvals for shipments taking between three and four months, trucks being “held at checkpoints for five days,” and convoys being cancelled on security grounds. A UN aid worker said that compared to 2019, there had been no improvement during the first three months of 2020 in the number of health care facilities in nongovernment-held parts of northeast Syria that had received aid supplies from Damascus.
Aid agencies said that in March, the WHO and UNICEF in Damascus sent medical supplies to Qamishli, in government-held northeast Syria, including emergency health kits, midwifery kits, and resuscitation kits, and that a little over half, measured in weight, reached nongovernment-held areas.
On April 14, the WHO said it transported 20 tons of medical equipment to Qamishli, including seven ventilators. According to the UN, the WHO previously sent a shipment of medical aid, including personal protective equipment and sterilization items, to the government-affiliated Department of Health in al-Hasakeh and to Qamishli, and that the shipment to Qamishli will be used only by the government-run hospital there.
An aid worker said that the March and April deliveries “do not come close” to the amount of medical aid the UN used to transfer to northeast Syria from northern Iraq, which other aid workers confirmed.
According to a forthcoming report from the UN Secretary General on the situation in Syria obtained by Human Rights Watch, in February and March, two UN agencies - UNICEF and UNFPA - delivered 64 tons of health supplies in two shipments to northeast Syria by road, of which almost 60 percent were delivered to health facilities or healthcare agencies previously supplied through al-Yarubiyah. The report underlines, however, that only 30 percent of facilities previously supported through al-Yauribyah received some of these supplies.
An aid worker told Human Rights Watch that as of mid-April, the Syrian authorities had not granted the WHO authorization to take their supplies by road from Damascus to UN warehouses in Qamishli and had insisted that security forces would have to escort any such convoys. The UN secretary-general’s February report said that in 2019, the Syrian authorities did not give any permission for UN supplies to reach northeast Syria by road. The report also underlined that as air freight is significantly more expensive than road convoys, the UN would require overland authorization if it “is to increase the delivery of health materials to the north-east in a sustainable manner.”
One aid worker said that the UN resident coordinator in Damascus is responsible for asking the Syrian authorities there to allow the UN and non-UN aid groups to transport supplies and personnel from Damascus to northeast Syria, but it remains unclear to what extent these requests are being granted.
Four aid workers said that as a result of ongoing bureaucratic obstacles in Damascus, they have been “unable to scale-up quickly from Damascus” to respond to the threat of Covid-19 in northeast Syria.
In mid-March, the WHO’s Syria representative in Damascus said:
If we want to send aid to the north-east, we have to get what is called a ‘facilitation letter’ from Damascus … so far, we did not have any problems … it was smooth … more than 50 percent of supplies were going to non-government-controlled areas[,] either directly to the hospital, or even to the Kurdish Red Crescent and other partners, NGOs [nongovernmental organizations], and of course, 30 percent or 40 percent to areas under government control.
On March 30, the UN Security Council discussed Syria’s Covid-19 response, including the issue of the Syrian authorities in Damascus blocking aid deliveries between Damascus and nongovernment-controlled areas in the northeast. The UN emergency relief coordinator said that that medical facilities and individuals in northeast Syria who had depended on medical supplies arriving from northern Iraq through the Yarubiyah border crossing had not yet received them through alternative channels. He noted that, as a result, medical supplies were running low and that at least one primary health care center was likely to close. The UN Secretary General’s forthcoming report on the situation in Syria confirms this, concluding that “multiple medical facilities previously dependent on the cross-border operation reported acute shortages.”
General Health Care Situation in Syria
After nine years of war that destroyed much of the country’s infrastructure, just over 11 million Syrians needed humanitarian assistance as of early 2020. Millions still lack regular access to safe and clean water, which is critical to supporting good hygiene practices. Many people live in dense urban centers, informal settlements, or overcrowded camps, making it nearly impossible to use the social distancing measures necessary to mitigate the spread of the virus.
As of April 21, the Syrian authorities said the country had confirmed 42 cases of Covid-19 resulting in 3 deaths. On April 15, the WHO said the authorities in Damascus had carried out about 1,500 tests, and previously said that this number of tests is far below the number needed to establish the extent to which Covid-19 has spread in the country. According to the UN, China sent about 2,000 more kits to Damascus in mid-April while Russia donated 50 ventilators, 10,000 test kits, and 2,000 sets of personal protective equipment. The authorities have set up at least 12 quarantine centers across government-controlled areas and as of mid-April, only had one testing laboratory, in Damascus.
A recent survey concluded that the maximum number of Covid-19 cases that could be adequately treated in Syria is about 6,500, based on the number of Intensive Care Unit beds with ventilators – about 325 – and a calculation that an approximate 5 percent of the total Covid-19 cases would require critical care. According to a well-informed medical source in Damascus, Syria has only about 300 ventilators.
In late March, the WHO said that because of border closures and the suspension of flights it was having trouble ensuring that the equipment needed to test for the coronavirus was available.
Several countries have placed sanctions on Syria, including the United States and the European Union. Two aid workers said that some of the material required for Covid-19 testing is under sanctions but that they have applied for exemptions and are awaiting a response from the US Department of Trade. Such exemptions should be granted without delay.
Recommendations
To adequately prepare for a possible Covid-19 outbreak in northeastern Syria, the following urgent steps should be taken.
Given the speed with which Covid-19 overtakes even the most sophisticated health systems, the UN Security Council should immediately reauthorize cross-border operations from northern Iraq into northeast Syria through the Yarubiyah border crossing by renewing UN Security Council Resolution 2449 of December 2018, which grants explicit permission for cross-border aid delivery through four border crossings for one year. This would enable the WHO to rapidly scale-up its support to the region and allow international aid groups providing front line services in northeast Syria to get funds under the Covid-19 Global Humanitarian Response Plan.
Russia should not oppose a UN Security Council reauthorization of the Yarubiyah crossing, especially as Damascus has not allowed UN and non-UN agencies to increase their cross-line delivery of health care-related supplies from Damascus to northeast Syria, which might otherwise have compensated for the January closure of al-Yaribuyeh. Russia should also vote for a renewal of the entirety of the December 2018 cross-border resolution. Russia should also use its influence to pressure the Syrian authorities to allow UN and non-UN aid agencies unimpeded humanitarian access to all areas in Syria, including areas not under the Syrian government’s control.
The Syrian government should immediately facilitate unimpeded access for UN and international aid agency staff to all areas of Syria, including areas not under Syrian government control. It should also ease restrictions that create undue bureaucratic delays around medical supplies and other aid reaching northeast Syria and allow aid groups to conduct independent needs assessments and assist people on the basis of need, without any political constraints.
The WHO, the UN secretary-general, the UN under-secretary-general for humanitarian affairs and emergency relief coordinator and the resident humanitarian coordinator in Syria should continue to press the Syrian authorities to allow WHO and other UN agencies in Damascus to provide supplies and personnel aid to all parts of Syria in an equitable manner and based purely on an objective needs assessment. They should also support international aid groups’ ability to procure urgently needed medical supplies that may not be commercially available in the region or elsewhere by providing access to the UN’s preferred vendors and supply chains.
The KRG in northern Iraq is obliged to take measures to control the spread of Covid-19 in the Kurdistan Region of Iraq, but as far as any necessary precautions allow, it should let humanitarian supplies and personnel enter northeast Syria and allow aid agencies to transport humanitarian supplies from its cities to the Syrian border. It should also remove the restrictions on medical supply sales to aid groups that are trying to respond to the lack of supplies from the UN after the UN Security Council withdrew authorization of UN cross-border aid to the area.
Turkey should cease cutting off the water flow from Allouk water station and press the KRG in northern Iraq to allow non-UN aid agencies to cross back and forth into northeast Syria.
International donors, including the US and the EU, should encourage the Syrian authorities and the KRG to allow medical supplies and personnel to enter northeast Syria. Donors should also ask the UN resident coordinator in Damascus to provide regular updates of how many requests the UN, WHO, and international aid groups have submitted to the Syrian authorities to establish local testing capacity, accelerate full sharing of information of all test results, and transfer supplies and personnel from Damascus to nongovernment-held parts of the northeast, how many have been refused and on what grounds, how swiftly the rest have been approved, and how many of the supplies and staff have reached those areas.
Donors should ask the UN Security Council to reauthorize UN agencies’ use of the Yarubiyah border crossing to help supplies and staff reach northeast Syria from northern Iraq. The secretary-general and emergency relief coordinator should continue to press the council to do so, while exploring ways to continue to ensure that lifesaving aid continues to move across borders if the mandate is not fully restored.