
"The doctor said to my daughter ‘If they had forced themselves on you, there should have been marks on your body – but you don’t have any. You must have done this of your own free will.’” Palak’s mother said that her daughter, already traumatised, felt humiliated and scared after the medical exam.
Palak (name changed to protect her identity), a Dalit woman, was 18 when she reported being kidnapped and raped in Madhya Pradesh, in June 2013.
As part of the legal reforms after the gang rape and murder in New Delhi in 2012, denying medical treatment to rape survivors is punishable under section 166B of the Indian Penal Code with imprisonment for up to a year.
Health providers have a dual role when it comes to responding to sexual violence. Apart from collecting forensic evidence for any criminal investigation and prosecution, they must provide therapeutic care to survivors – including addressing their sexual, reproductive and mental health problems.
However, as in Palak’s case, Human Rights Watch’s investigation into 21 recent cases of rape and sexual harassment in India shows that instead of providing a safe environment of trust for treatment and examination, doctor attitudes toward women who report rape can leave them traumatised a second time.
The 2014 guidelines
In 2014, India’s Ministry of Health and Family Welfare issued guidelinesfor medico-legal care for survivors of sexual violence to standardise healthcare professionals’ examination and treatment of sexual assault survivors. The guidelines integrate processes geared to respect women’s and children’s rights to privacy, dignity, creating a non-threatening environment, and informed consent.
The Ministry of Health and Family Welfare, in collaboration with the World Health Organization, has conducted five regional workshops over the last two years to encourage adoption and implementation of the guidelines by the states. However, so far, according to health rights groups, only nine states have adopted the guidelines. But even in these states, the implementation has been uneven, without any oversight mechanisms in place.
The guidelines seek to correct pervasive myths and degrading practices around rape that have been reinforced by common medico-legal practices. Specifically, the guidelines eliminate what is commonly known as the “two-finger test,” a practice where the examining doctor notes the presence or absence of the hymen and the size and so-called laxity of the vagina of the rape survivor, to assess whether girls and women are “virgins” or “habituated to sexual intercourse”.
This evidence has been used during trials to assert that the rape survivor had “loose” or “lax” morals. The new guidelines limit internal vaginal examinations to those “medically indicated,” such as when it is done to diagnose infection, injury, or presence of a foreign body.
Even before the guidelines, the Supreme Court held that the results of the test cannot be used against rape survivors and further that whether she is “habituated to sexual intercourse” or not is irrelevant, constitutes an arbitrary and unlawful interference with the survivor’s reputation. The 2015 edition of Modi’s Medical Jurisprudence, a key reference tool for medical and legal professionals, has also attempted to steer doctors away from the unscientific “two-finger test.”
End abusive “two-finger testing”
However, Human Rights Watch has found that doctors continue to conduct the invasive, humiliating, and inhumane finger test to make degrading characterisations. The doctors also fail to explain the process or purpose of the finger test to rape survivors, causing them to be further traumatised. The test can also cause pain. The doctors do this irrespective of whether the survivor is under 18 or an adult, single or married.
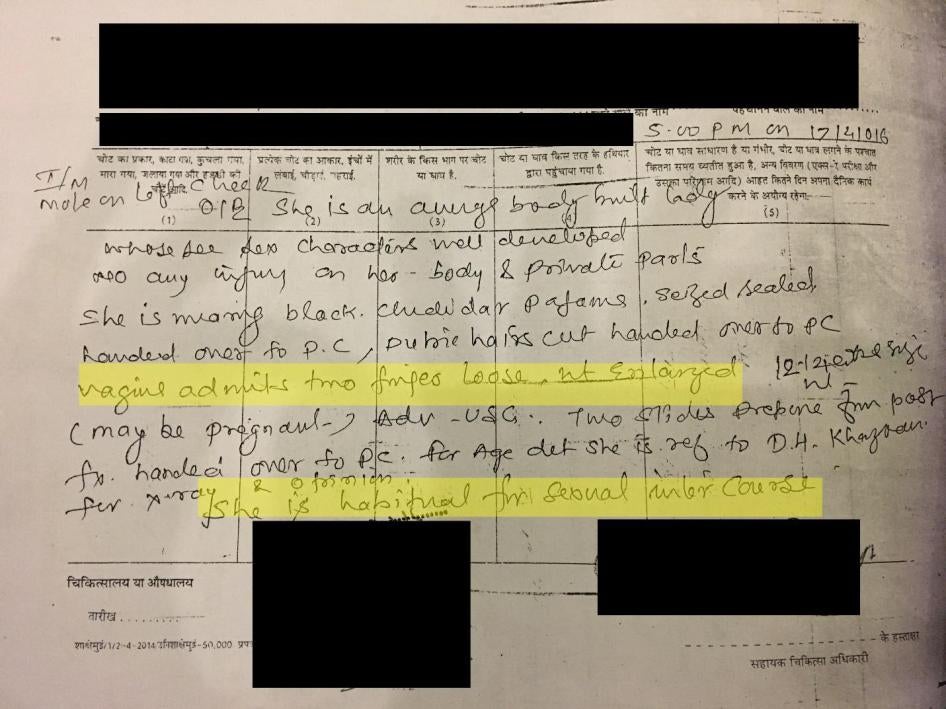
Gayatri (not her real name), from Madhya Pradesh, was 17 when her brother witnessed their father raping her in April 2016, which had been going on for months. After they reported rape, the doctor noted she was likely pregnant, but still conducted a “two-finger test”. The doctor wrote that her “vagina admits two fingers loose, not enlarged” and concluded that “she is habitual to sexual intercourse”. The test was completely contrary to the guidelines, which Madhya Pradesh state has adopted, and served no purpose at all.
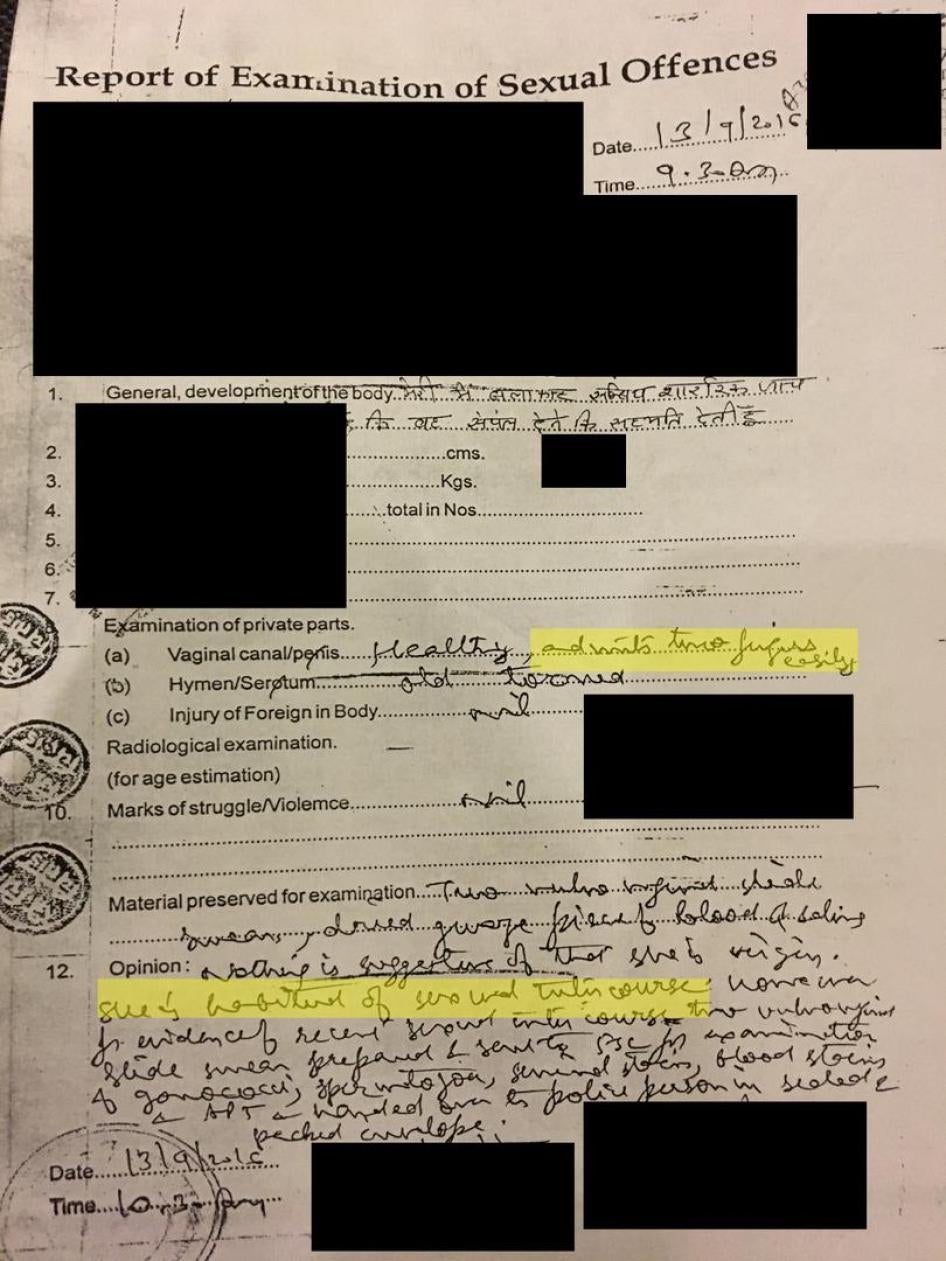
Harshita (name changed to protect her identity), a 30-year-old married woman from Chittorgarh in Rajasthan, reported being repeatedly raped by a relative for a year and a half in July 2016. The doctor examining her conducted a “two-finger test” and observed that her vagina “admits two fingers easily,” and she was “habitual of sexual intercourse,” an unnecessary conclusion for legal purposes.
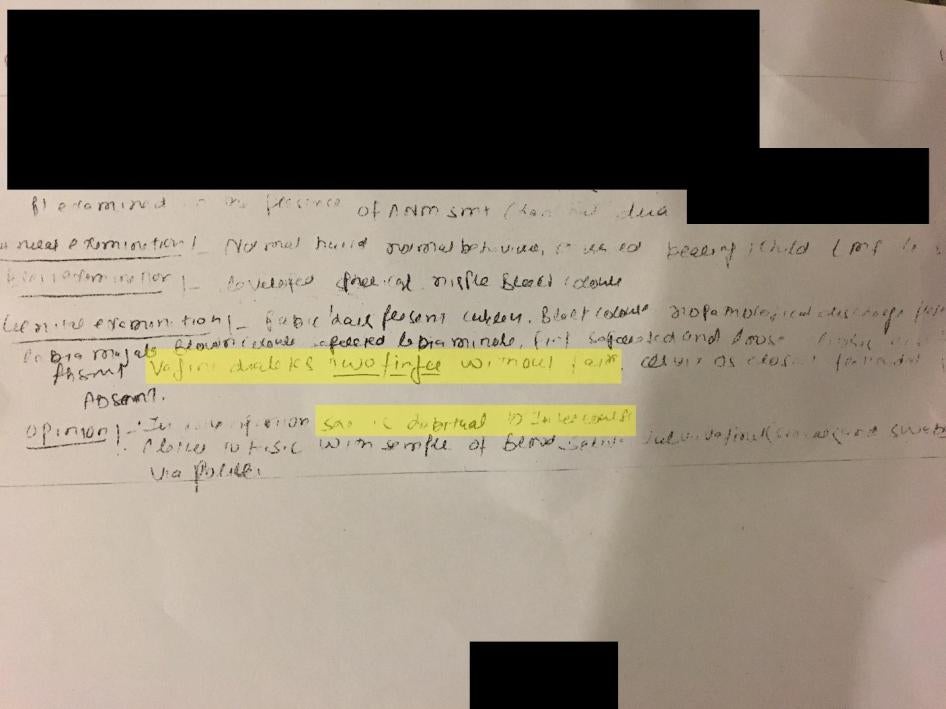
The use of the finger test can also harm the investigation process because police, too, may rely on medico-legal reports. Sameena (not her real name), 25, from Bharatpur in Rajasthan was pregnant at the time she reported being gang raped in March 2016. Instead of noting that the police did not bring her for the medical exam until several days later, resulting in loss of critical evidence, the doctor conducted a “two-finger test” and observed that it was “without pain,” and that “she is habituated to intercourse”. In October 2016, the police filed a charge-sheet against the five accused for assault, intent to outrage her modesty, and for sexual harassment, but ruled out rape. As part of reasons for the decision, the police cited the medico-legal report to say that Sameena did not have any injuries on her body and “was habitual of intercourse”.
Failure to provide adequate healthcare
Human Rights Watch also found that doctors frequently give priority to the collection of forensic evidence, and spend little, if any, time on essential therapeutic care. The 2014 guidelines lay out psychosocial care for survivors saying that health professionals should themselves provide first-line support or ensure someone else trained at the facility can provide it. This includes addressing the survivor’s well-being, encouraging her to express her feelings and seek crisis counseling, making a safety assessment and safety plan, and involving family and friends in the healing process. But the state healthcare systems have largely failed when it comes to providing therapeutic care and counseling to survivors.
Gayatri, who had been raped repeatedly by her father, did not know she was three months pregnant until the medico-legal examination.
According to Gayatri’s aunt, the gynaecologist said they needed the court’s permission to perform an abortion, even though the law states that pregnancy can be terminated for those under 18 years with the written consent of her guardian. Gayatri’s uncle filed a petition in lower court but the court denied the request. Her uncle then appealed to the High Court, which in May 2016, gave Gayatri permission to terminate her pregnancy. By the time Gayatri terminated her pregnancy, she was five-months pregnant. Gayatri was not offered any follow-up care or psychosocial counselling after the abortion, and was ill for some time.
Lack of adequate training, resources, and oversight mechanisms to ensure doctors treat sexual assault and rape survivors with dignity and offer them the necessary services, have left survivors without the critical support they need. The central government should work with all states to adopt, enforce and implement the 2014 medico-legal guidelines.
This is the second in a three-part series looking at barriers to justice, health care, effective legal aid and other support services for sexual assault survivors in India. despite strong laws and policies since the 2012 gang rape and murder in Delhi. The first part can be read here.








