
Summary
Khobor lives with his wife, two sons, and daughter in a rural village in central Bangladesh. Their house is small, with a dirt floor, thatched walls, and a corrugated tin roof. Too poor to own his own land, Khobor earns his living farming a richer neighbor’s land and sharing the meager profits. When he spoke to Human Rights Watch, he had returned from nearby fields with fodder for the family’s one cow. Lean and muscular, he was sweating from exertion under the midday sun.
In his mid-30s, Khobor recently noticed patchy marks across his chest and on his feet. His mother died three years ago and his father a year later, both with similar but more pronounced marks on their bodies.
Khobor suspects these marks are caused by arsenic in water from the family’s nearby tubewell, a small diameter pipe drilled into the ground that allows him to draw up water by a hand pump. When the government tested water from the tubewell many years ago they told him the water had around “250 [micrograms per liter] arsenic.” The family has no alternative but to drink from the contaminated well. Still, he knows what that means: “[The water] can kill us.”












Arsenic in water is colorless, tasteless, and odorless. Exposure to high amounts, such as through accidents or deliberate poisoning, can result in seizures, coma, cardiovascular collapse, and death. Exposure to lower doses can also have severe health consequences, although these will take many years to develop. While dark and/or light spots on the skin and a hardening of the skin on the palms and soles are often the first visible symptoms of chronic exposure, the main causes of death are cancers and cardiovascular and lung diseases.
Khobor told Human Rights Watch that since testing his tubewell many years ago, no one from the government has returned. Most of the private wells nearby are also contaminated and there are no government tubewells in his part of the village. He’s never seen a government doctor or healthcare worker for the serious health problems that arsenic exposure is known to cause.
Left to their own devices, Khobor and his family try to avoid arsenic as best they can. The roof of tin sheets on their home allows Khobor to capture rainwater during the rainy season. But when the rains end, his household’s only storage vessels—one white metal bucket and one clay pot—will supply drinking water for one week, two at best. Then the family returns to using their tubewell and drinking water they know is slowly killing them.
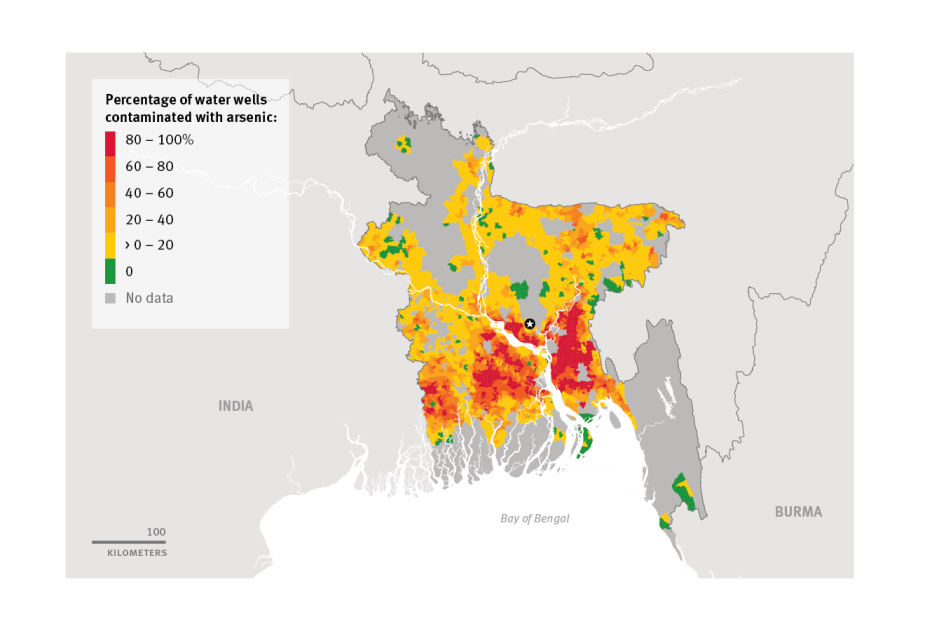
Arsenic occurs naturally in Bangladesh’s groundwater. But arsenic’s deadly contamination of the drinking water of many millions of Bangladesh’s rural poor is a disaster that humans have caused and perpetuated.
Arsenic does not affect the drinking water of Bangladesh’s capital Dhaka or other large cities, where drinking water comes from deep aquifers of higher-quality water, or from treated surface water, which is then distributed through a network of pipes.
Rather, it affects hand-pumped, mostly shallow, tubewells across huge swaths of rural Bangladesh. The common figure given for the number of shallow tubewells across the country is about 10 million, although this is a crude estimate.
The government and international donors initially promoted the proliferation of tubewells many years ago as a source of drinking water in order to reduce death and illness from microbial contamination of surface water. From the start of these campaigns to the early 1990s, it was not known that much of Bangladesh’s shallow groundwater, particularly in the center and south of the country, contains arsenic. The campaigns were successful and much of the rural population shifted to government and donor-funded wells, or began to install their own.
Today, an estimated 43,000 people die each year from arsenic-related illness in Bangladesh, according to one study. The authors go on to estimate that, depending on progress of ending exposure, between 1 and 5 million of the 90 million children estimated to be born between 2000 and 2030 will eventually die due to exposure to arsenic in drinking water.
Bangladesh maintains a standard of 50 micrograms of arsenic per liter of water. However the evidence for considerable death and illness from exposure to arsenic in drinking water between 10 and 50 micrograms is increasing.
This report is based on field work in five villages in Bangladesh; a total of 134 interviews, including with people suspected of having arsenic-related health conditions, caretakers of government water points, as well as government officials and staff of nongovernmental organizations (NGOs); and the analysis of approximately 125,000 government water points installed between 2006 and 2012 (constituting approximately 85 percent of government water points installed during this period).
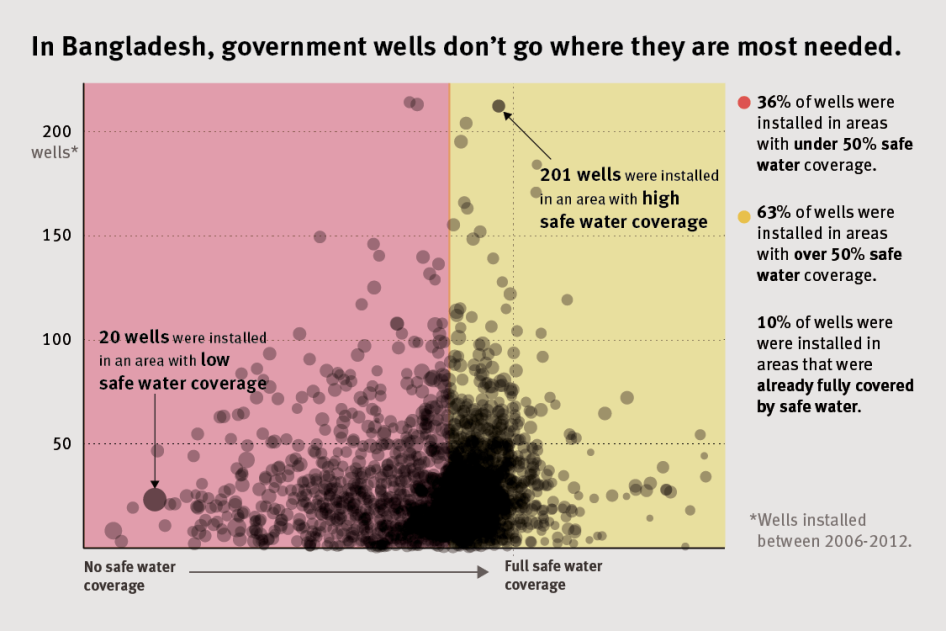
It finds that the official response to arsenic contamination of drinking water in Bangladesh’s rural villages is failing, with the government instead expending considerable resources in areas where the risk of arsenic contamination is relatively low and where water coverage is relatively good. Despite government reports stating that the government should do a better job of targeting arsenic mitigation options in areas where they are most needed, it inexplicably fails to do so. Human Rights Watch wrote to the government to ask the reason for this approach, but no reply had been received at time of publication.
It also finds that, long before such water points are installed, politicians undermine the allocation of new government water points by diverting these life-saving public goods to their political supporters and allies. In at least one recent government project, official policy recognized the influence of parliamentarians in siting 50 percent of all new water points.
There is a serious lack of monitoring and quality control in arsenic mitigation projects. In a small but significant number of cases, government-installed water points are themselves contaminated with arsenic above the national standard. Human Rights Watch visited one village where some contaminated government-installed wells were used by villagers as a source of drinking water. According to Human Rights Watch’s analysis of approximately 125,000 government water points installed between 2006 and 2012 (constituting most government water points installed in this period), some 5 percent were contaminated above the Bangladesh standard.
The failures of the government to take reasonable steps to target interventions in the areas where the risk of arsenic contamination is high, to tackle technical difficulties (where they exist), to control the quality of projects to mitigate arsenic exposure, combined with a widespread diversion of safe water devices for political supporters and allies, violates the human rights to water, to health, and ultimately the right to life.
The government and international donors promoted tubewells as a source of drinking water in rural Bangladesh many decades ago without precautionary tests of tubewell water for chemical hazards such as arsenic. Yet ongoing exposure cannot be understood the same way. Rather, it is the result of political complacency over the progress made, political interference in the distribution of life saving alternatives, and a lack of quality control in executing and monitoring projects.
Tackling Contamination
The vast scale of arsenic contamination of rural water supplies began to be understood by the mid-1990s. From 1999 to 2006, the government, international donors, and nongovernmental organizations (NGOs) oversaw a concerted effort to mitigate arsenic contamination in Bangladesh’s groundwater. Some 5 million tubewells across the country were tested with field kits and the results communicated to their owners.
Although the World Health Organization (WHO) has set a provisional guideline value of 10 micrograms of arsenic per liter of drinking water, Bangladesh’s standard allows for a much higher concentration—50 micrograms per liter—and the pumps were painted red or green according to whether they were above (red) or below (green) its standard. Subsequent studies showed that many people switched wells for their drinking water to a green painted well when there was one relatively close by.
The government, international donors, and NGOs installed a few hundred thousand safe water devices—mostly deep tubewells that reach groundwater of better quality. Bangladesh also adopted a National Policy for Arsenic Mitigation and an accompanying implementation plan in 2004. In 2005 the country adopted a “pro-poor strategy” to prioritize poor villagers when new government water points were allocated.
Waning Efforts
Since 2006, however, the urgency of such efforts has dissipated.
With little or no ongoing government water testing of wells and monitoring of results at the village level, some people perceive that the problem has been largely solved. Most progress reviews involve counting the number of safe water devices installed by the government, international donors, and NGOs, then multiplying those totals by a hypothetical number of optimal users for different water points. Calculated in this way, the response to arsenic contamination of drinking water in Bangladesh means millions of people are “covered” by safe water devices.
A more direct way to measure the extent of progress is by testing water at the village level. The national tubewell screening from 2000 to 2006 found that approximately 20 percent of tubewells across the country, providing water for an estimated 20 million people or 14 percent of the national population, yielded water with arsenic above 50 micrograms per liter.
In 2013, a nationwide study of drinking water quality showed a similar result. Although it measured samples of drinking water at the point of use—people’s homes—rather than tubewells, it found that 12.4 percent of samples exceeded the Bangladesh standard, a rate that corresponds to some 20 million people exposed to arsenic above this level.
Shallower tubewells that individual families have installed relatively cheaply are generally more likely to be contaminated and far outnumber the number of safe government water points. Most of the former are untested and villagers are left to guess whether wells are contaminated. In many cases, they no longer care. Public awareness campaigns stressing the dangers of arsenic ended many years ago. The government’s approach to well water testing—which relies on villagers bringing their water samples to a government office in a district town—barely functions.
Health Impact Ignored
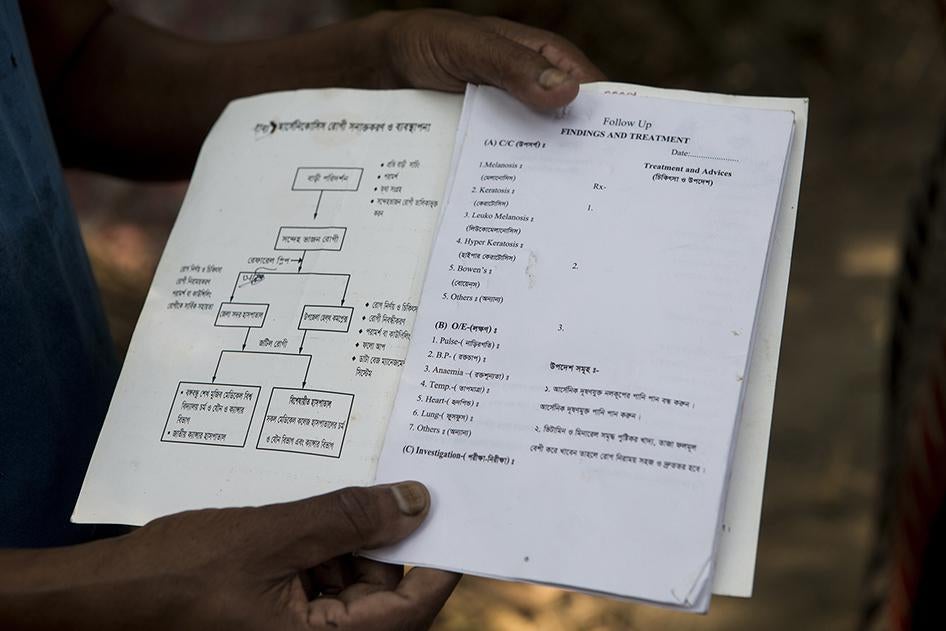
Within Bangladesh’s health system, the impact of past and current exposure to arsenic on people’s health is being largely ignored. In the course of researching this report, Human Rights Watch was repeatedly told that government doctors or health care staff do not currently conduct arsenic screening in villages. If patients go to village health clinics with symptoms of arsenic exposure, they are told nothing can be done for them. If they go to health complexes in nearby towns, they are often told there are no longer even the multivitamins and ointment that they used to receive as treatment.

The government keeps a national list of patients, identifying them primarily via their skin lesions. Yet the vast majority of exposed individuals (even with high levels of chronic exposure) will not develop skin lesions and are at risk of other diseases. The main causes of death from arsenic are cancers (of the skin, liver, kidney, bladder, and lungs), cardiovascular disease, and lung disease.
Calculating the death and disease caused by arsenic among Bangladesh’s rural population involves many uncertainties, including variations in individual exposure over time, and different latency periods between different diseases. Despite these uncertainties, it is estimated that arsenic will cause premature deaths of millions of Bangladeshis.
Even when not fatal, millions of Bangladeshis will live with the effects of cardiovascular diseases, cancers, lung diseases, and other illnesses linked to arsenic exposure such as diabetes, hypertension, and tuberculosis. Children will suffer impaired cognitive functions.
There have been efforts to supply safe drinking water to rural villagers, led by the Department of Public Health Engineering (DPHE) under the Ministry of Local Government, Rural Development and Cooperatives. In some villages, the government’s deep tubewells are functional, accessible, and supply abundant and life-saving water for thousands.
Failing Response to Arsenic Contamination
This report finds that, at the national level, the government is expending considerable resources in areas where the risk of arsenic contamination is relatively low and where water coverage is relatively good.
For the most part, things look a little better at the village level.
Of the 56 government water points that Human Rights Watch located across five villages, 23 were both functional and accessible. However, 18 were not functioning (and hence no longer used) and 15 were functioning but restricted from the general public. In a small but significant number of cases, it appears that government-installed water points are themselves contaminated with arsenic above the national standard.
There are undoubtedly technical difficulties in installing safe water devices in some areas, including a layer of hard gravel above the arsenic-safe aquifer. But at the village level there is little or no evidence of concerted efforts to tackle such geological or hydrological challenges. Indeed, even in areas where technical difficulties exist, a small number of functioning government or NGO water points provide safe alternatives, suggesting that, with reasonable effort, far more could be done to mitigate exposure in such areas.
Necessary Steps
Bangladesh has led international advocacy to recognize water as a human right at the United Nations. But at the national level, realizing this right to water requires reviving the commitment that the government and international donors displayed up until 2006.
It requires improved targeting of high priority areas. It requires ending the pernicious influence of political representatives on the allocation of new water points. It requires remediation plans for communities serviced by contaminated water points. It requires a massive effort to test all wells, including private, shallow tubewells.
Bangladesh’s obligation under the right to health requires that people living in rural villages and suspected of having arsenic-related health conditions have access to basic health care. Bangladesh has a nationwide system of village-level community health clinics, however they currently do little or nothing for arsenic-related illnesses. The government should build upon these clinics and strengthen the capacity of upazila (sub-district) health centers and district hospitals to diagnose, treat, and care for the vast majority of individuals exposed to arsenic who will suffer chronic diseases without easily visible symptoms like skin lesions.
Bangladesh’s bilateral and multilateral donors should seize this moment to act. There is an urgent need for a comprehensive national level arsenic mitigation strategy for Bangladesh.
But this report also finds increased care in funding is required.
UNICEF and the World Bank have been two significant international donors to recent and current government efforts to install safe water points. From 2007 to 2012, UNICEF supported the government to install what were intended to be safe water points, although (in UNICEF’s words) there was not a “transparent and honest process for the collection and submission of water samples for [initial] testing.” Follow-up testing in 2012 and 2013 found that 1,733 wells (out of 20,597 installed wells) were contaminated by arsenic above the national standard. UNICEF subsequently rehabilitated or replaced the 1,733 contaminated wells.
UNICEF also supported broader follow-up testing of a larger set of approximately 125,000 water points installed by the DPHE from 2006 to 2012. As noted above, that testing covered approximately 85 percent of the total government water points installed over that period. The results showed a further approximately 5,000 wells contaminated by arsenic above the national standard. According to correspondence received from both UNICEF and the World Bank, these wells were painted red but Human Rights Watch has no indication that the government has replaced or rehabilitated them.
Human Rights Watch does not have information to suggest that water points installed with support from the World Bank’s Bangladesh Water Supply Program (2004-2010) are contaminated. However water points supported by the bank were included in the larger set of approximately 125,000 water points tested by the DPHE—of which some 5 percent were found contaminated.
Human Rights Watch believes the bank should promptly and thoroughly investigate whether water points installed with its support are contaminated and, should it find any that are, replace or rehabilitate those wells. In correspondence with Human Rights Watch, the World Bank country director wrote that the bank agrees with the need to review whether any bank-supported wells are contaminated and is currently considering ways to undertake a review.
For all international donors supporting government efforts to install safe water points, increased care when executing and monitoring projects is necessary. In practical terms, this means measuring success not simply in terms of what is built, but assessing project outcomes in terms of safety, functionality, and how many people actually benefit. UNICEF and the World Bank have reported to Human Rights Watch that they have put in place enhanced water quality monitoring protocols for ongoing or future water projects.
Realizing the rights to water and to health is a matter of life or death for Bangladesh’s rural poor.
Recommendations
To the Government of Bangladesh
- End any official or de facto policy or practice whereby political representatives (members of parliament, upazila (sub-district) chairmen, or others) influence the locations of government water points;
- Adopt a national plan to end arsenic exposure through drinking water in Bangladesh, with quantifiable targets, sufficient budget allocations, and a fixed time frame for implementation. Designate the Department of Public Health Engineering (DPHE) and Directorate General of Health Services (DGHS) as lead agencies responsible for reducing exposure in rural drinking water. As part of this:
- Direct the Department of Public Health Engineering (DPHE) to implement a dedicated and comprehensive arsenic mitigation project specific to all those administrative unions already identified as “very high” and “high” priorities for action;
- Launch a national awareness-raising campaign on the health problems caused by arsenic. Disseminate such information through radio, television, mobile phones, and more innovative forms of communication such as village theatre and music. Integrate the campaign with improved government efforts to provide water testing services for arsenic, as well as improved medical testing, treatment, and care for people suffering arsenic-related health conditions;
- Include a time-bound commitment to reduce the current standard for arsenic in drinking water (50 micrograms per liter) to WHO’s current provisional guideline value of 10 micrograms per liter.
- Reactivate a high-level inter-ministerial committee to oversee national arsenic mitigation activities, supported by a secretariat tasked to collect, collate, and evaluate data on mitigation progress and continuing exposure;
- Prepare an annual report for the general public explaining the current status of contamination and exposure, ongoing and planned activities, and future needs for arsenic mitigation. Report the number of people still exposed, detailed to the union-level;
- Establish a regulatory body to oversee rural drinking water safety. Ensure that the regulatory body:
- Is independent of the Department of Public Health Engineering and any other government agency responsible for providing water;
- Has sufficient capacity to independently test rural water points, both public and private; and
- Reports annually to parliament and the public about the state of efforts to improve the safety of rural drinking water, including progress on the national plan to end exposure to arsenic through drinking water.
To the Department of Public Health Engineering (DPHE)
- Publicly adopt a policy of “zero tolerance” of any attempts to influence the process of allocating government water points that is not based strictly on objective criteria relating to the actual need of people or communities;
- Take immediate steps to end arsenic exposure from contaminated government water points, including but not limited to installing alternative water sources (such as new deep tubewells, piped water supply systems, rainwater harvesters, or dug wells), drilling existing tubewells to a greater depth, and building arsenic and iron removal plants;
- On an urgent basis, revise and review existing databases, including the Nationwide Public Water Point Mapping database, for government water points contaminated with arsenic. Supplement this data with screening of government water points where there are technical indicators to suggest other government water points may be contaminated;
- Immediately prioritize a dedicated and comprehensive arsenic mitigation project specific to all administrative unions already identified as “very high” and “high” priorities for action. Include measurable and time-bound goals to reduce exposure in these areas, with independent third party quality control to assess results of the project;
- For dedicated arsenic mitigation projects and general rural water supply projects, operationalize the Government’s “Pro Poor Strategy for Water and Sanitation Sector” (2005) by identifying and mapping clusters of households of poor villagers where that basic minimum level of service is not met, and ensure that such clusters will get priority in the allocation of government water points;
- Unless recommended by a technical committee on the basis of site specific assessments, reduce the allocation of shallow tubewells in favor of increasing allocations of arsenic-safe alternatives in arsenic-prone areas;
- Improve availability of information regarding government water points. Specifically:
- Require bulletin boards in public places to inform local communities on the location of all government water points. Include information on the year of allocation, sources of funds, the name and address of the contractor(s) carrying out the work, the name and address of government water point caretaker(s), and the depth (range) of the well;
- Make the Nationwide Public Water Point Mapping database publicly available, including the GPS coordinates of all government water points.
- End the unrealistic expectation that unpaid community caretakers are responsible for operating and maintaining government water points by creating a system for community members to report to district DPHE offices where government water points have become non-functional or otherwise need maintenance. Dispatch DPHE mechanics to repair water points where technically possible. Record and report such activities publicly;
- Exchange information about the locations of contaminated water points with DGHS so that improved surveillance, treatment, and care programs for chronic diseases known to be caused by arsenic can be targeted to these areas;
- Ensure all district and upazila (sub-district) DPHE offices are provided with sufficient arsenic test kits and are required to regularly use these to monitor and report on arsenic levels in public and private water supplies in the area.
Directorate General of Health Services (DGHS)
- Provide, at a minimum, nutritional supplements and basic symptomatic treatment for skin lesions at village-level community healthcare centers. Ensure a continuity of supply. Improve referral processes to district hospitals and upazila-level healthcare centers;
- Initially for district hospitals and upazila-level healthcare centers covering administrative unions identified as “very high” and “high” priorities for action, and then in other areas of the country, develop and implement improved surveillance, treatment, and care programs for chronic diseases known to be caused by arsenic, including but not limited to cancers, cardiovascular disease, respiratory disease, diabetes, and hypertension;
- Initially in administrative unions already identified as “very high” and “high” priorities for action, and then in other areas of the country, undertake village-level health camps with a view to improving the accuracy of the national registry of people suffering arsenic-related health conditions;
- Initially in administrative unions identified as “very high” and “high” priorities for action, and then in other areas of the country, instruct doctors, nurses, and other healthcare workers attending to patients to always enquire what a patient’s drinking water source is, and if the patient knows the arsenic concentrations in it. If the arsenic concentration is unknown, the patients should be advised where the water can be tested, and requested to bring the arsenic test result with them for their next appointment;
- Initially in administrative unions identified as “very high” and “high” priorities for action, and then in other areas of the country, ensure all village-level community healthcare centers, upazila-level healthcare centers, and district hospitals are equipped with arsenic test kits;
- Exchange information about patient locations with DPHE so that new water points can be targeted to these villages;
- Initially in administrative unions identified as “very high” and “high” priorities for action, and then in other areas of the country, launch a national awareness-raising campaign on the health problems caused by arsenic, including the death and illness due to arsenic exposure in utero and early childhood, and later in adulthood;
- Initially in administrative unions identified as “very high” and “high” priorities for action, and then in other areas of the country, support research to monitor excess death and illness due to arsenic exposure and, on an ongoing basis, target and improve surveillance, treatment, and care interventions accordingly.
To the Donor Community
To the World Bank
- In addition to reviewing the results from 125,000 government water points tested by DPHE in 2012-2013, promptly and thoroughly investigate whether water points installed under the World Bank’s Bangladesh Water Supply Program (2004-2010) are contaminated above the national standard and, if any are, replace or rehabilitate those wells.
To the Donor Community
- Support the government to replace or rehabilitate those government water points already identified as contaminated by arsenic above the national standard in the Nationwide Water Point Mapping database;
- Support a comprehensive national level arsenic mitigation strategy for Bangladesh, prioritizing:
- Improved targeting of safe water supply options to those areas already identified as “very high” and “high” priorities for action;
- Improved quality control mechanisms, including independent third party monitoring of safe water devices and public reporting of results;
- Improved government infrastructure for testing tubewells for arsenic;
- Improved government infrastructure for the surveillance, treatment, and care of chronic diseases known to be caused by arsenic;
- Publicly adopt a policy in any donor-supported projects of “zero tolerance” of any attempts to influence the process of allocating new government water points that is not based strictly on actual need of people or communities;
- Ensure independent third party assessment of project results, including random sampling and testing of water quality and rehabilitation or replacement when testing reveals water point contamination, is a mandatory component of any current and future rural water supply projects that receive multilateral or bilateral donor support.
Methodology
This report is based on information collected during five weeks of field research conducted in Bangladesh between June and September 2015. Human Rights Watch visited the capital city Dhaka as well as sites in seven rural districts. Some of these locations have been withheld to protect the confidentiality of government officials who spoke to Human Rights Watch on the condition of anonymity.
A senior researcher with Human Rights Watch interviewed 134 people for this report, including 50 people suspected of suffering arsenic-related health effects, 56 caretakers (or their family members) of government water points, 7 government officials, and 21 people who currently work, or previously had worked, on arsenic-related issues in Bangladesh.
Human Rights Watch undertook field work in five rural villages.
- Balia, in Ulania Union (of Mehendiganj Upazila in Barisal District), about 140 kilometers due south from the capital Dhaka. The village is located on the eastern-most edge of a large island beside one of the main rivers in Bangladesh, the Megnha. According to the 2011 census, Balia has a population of around 4,400 people living in some 900 households. Over 99 percent of villagers draw their drinking water from tubewells.
- Bilmamudpur, in Aliabad Union (of Faridpur Sadar Upazila in Faridpur District). It is located in central Bangladesh, about 60 kilometers west of Dhaka. According to the 2011 census, Bilmamudpur has a population of around 11,000 people living in some 2,400 households. Approximately 97 percent of the population draws its water from tubewells.
- Ruppur, in Pakshi Union (of Ishwardi Upazila, Pabna District), about 140 kilometers from Dhaka. It is located in north-western Bangladesh on the banks of the Padma River. According to the 2011 census, the village has a population of around 5,000 people living in some 1,300 households. 98 percent of villagers draw their drinking water from tubewells.
- Iruain, in Kandirpur Union (of Laksam Upazila in Comilla District), located about 90 kilometers south east from Dhaka. According to the 2011 census, it has a population of around 3,800 people in almost 800 households. 91 percent of the village is reported as getting its drinking water from tubewells.
- Tilchandi, in Haizadi Union (of Araihazar Upazila, in Narayanganj District), in central Bangladesh, located about 25 kilometers east of Dhaka. According to the 2011 census, the village has some 800 people living in 120 households. 83 percent of the village gets its drinking water from tubewells.
The five villages represent different geographic locations across areas affected by arsenic in groundwater: Balia is located in a coastal district (Barisal) in the south, Bilmamudpur is in a central district (Faridpur) west of Dhaka, Ruppur is in a north western district (Pabna), Tilchandi is in a central district (Narayanganj) east of Dhaka, and Iruain is in a south eastern district, Comilla.
The five villages represent a range of sizes. According to the 2011 census, Tilchandi is the smallest (with some 800 people living in 120 households) and Bilmamudpur the largest (with some 11,000 people living in some 2,400 households).
The five villages also represent a range of different profiles for prioritization for arsenic mitigation, as determined by the government.[1] Iruain (in Kandirpar Union) and Bilmamudpur (in Aliabad Union) are both in unions considered a “high priority” for arsenic mitigation, Balia (in Ulania Union) and Tilchandi (in Haizadi Union) are both in unions considered a “medium priority” for arsenic mitigation, and Ruppur (in Pakshi Union) is in a union considered a “low priority” for arsenic mitigation. None of the villages are in unions considered a “very high priority” for arsenic mitigation (i.e. those unions with supposedly over 80 percent water points contaminated by arsenic and less than 20 percent of the population covered by safe water devices).
Human Rights Watch spoke to 10 people suspected of suffering arsenic-related health conditions in each of the five villages.[2] These individuals were identified on the basis of their arsenic-related skin lesions as recognized by field workers with experience in identifying people suspected of having arsenic-related health conditions. As skin lesions affect only a small percentage of people suffering arsenic-related health conditions, Human Rights Watch also enquired about other health problems, as well as the health conditions of family members.
Of the 50 people suspected of suffering arsenic-related health effects, 27 were adult women and 23 were adult men. None were children.[3]
The interviews were conducted in Bangla through an interpreter. All people suspected of suffering arsenic-related health effects provided verbal informed consent to participate and were assured that they could end the interview at any time or decline to answer any questions. Interviewees suspected of suffering arsenic-related health effects have been given pseudonyms, and in some cases other identifying information has been withheld to protect confidentiality.
This report uses the term “water point” to refer to the main water supply technologies used. The principle types of water points installed in rural Bangladesh are shallow and deep tubewells, but the term can also refer to other technologies such as ringwells, shallow shrouded tubewells, rainwater harvesters, pond sand filters, and small piped water systems.[4]
Caretakers are individuals who have successfully applied to DPHE for a government water point on public land, usually near their place of residence, or on their own land. Designated caretakers of government-installed water points were identified by comparing lists from DPHE district offices and the main office in Dhaka and cross-checking those lists with information from local residents in the villages. Human Rights Watch spoke to 56 caretakers of government tubewells or, where those caretakers were not available at the time Human Rights Watch visited, relatives of caretakers from the same household.
Human Rights Watch conducted a short interview (of approximately 5-10 minutes) to confirm the well was installed under a government program, as well as to sight and discuss the well’s functionality and accessibility.
Where government tubewells were tagged by a unique national water point code—a twenty-digit number that includes information on the year of installation, the location, and the project that supported the water point—Human Rights Watch noted and photographed the code. In two instances, codes were searched in the Nationwide Public Water Point Mapping database to confirm verbal reports of arsenic contaminated government tubewells.
During this research, a technician with extensive experience in performing field tests for arsenic undertook a small number of water quality tests on behalf of Human Rights Watch. The Econo-Quick kit was used according to the manufacturer’s instructions.[5] A 50 mL water sample was collected directly into the kit's bottle after pumping for approximately one minute during periods of general water collection by members of the community. The kit uses a series of reagents added to a bottle containing the 50 mL water sample over a 10 minute reaction period. This reaction produces arsine gas if arsenic is present. The arsine gas developed by the addition of these reagents is then trapped on a reaction strip that contains mercuric bromide. The color of the reaction strip is then compared with the reference scale given by the manufacturer. The technician visually compared the color of the mercuric bromide strip to that of a reference scale corresponding to 0, 10, 25, 50, 100, 200, 300, 500 and 1,000 micrograms of arsenic per liter of water.
All tests performed indicated (as the caretakers were aware) that the wells tested contained arsenic over the Bangladesh standard. The results were communicated to caretakers and nearby householders, and villagers were encouraged to seek a neighboring well that contained less arsenic. Human Rights Watch communicated concerns about contaminated government wells in the village of Bilmamudpur to the government of Bangladesh.
Human Rights Watch also undertook statistical analysis of approximately 125,000 government water points located and tested by DPHE mechanics under the Nationwide Water Point Mapping Programme (NWMP) in 2012 and 2013, a data set that included the overwhelming majority of government water points installed between 2006 and 2012. As noted in this report, Human Rights Watch identified one government tubewell with a government identification code that was not included in the NWMP database, despite being installed during a year supposedly covered by that database.
Human Rights Watch spoke to seven government officials, including five from the Department of Public Health Engineering (DPHE), one from the Ministry of Health, and one local political representative. Some DPHE officials spoke to Human Rights Watch on the condition of anonymity. Some DPHE officials interviewed for this report were working in different districts to those where village-level field work occurred. In some cases, identifying information has been withheld to protect confidentiality.
Human Rights Watch also interviewed 21 people who currently work, or previously had worked, on arsenic-related issues in Bangladesh, including staff of nongovernmental organizations (NGOs), health administrators, staff of international organizations, and academic researchers. Secondary sources—including academic research, project reports, and media coverage—were reviewed and included to corroborate information from village residents. Bangladeshi laws and policies were also reviewed.
In January 2016, Human Rights Watch wrote to the minister of health and the minister of local government to request information on the government’s efforts to address arsenic in drinking water and to solicit responses to the issues documented in this report. This correspondence is attached in Annex 2. No reply had been received at time of publication.
In February 2016, Human Rights Watch wrote to UNICEF and the World Bank to request information on the steps taken to rehabilitate contaminated government water points. This correspondence and the respective replies, are attached in Annexes 3 and 4.
I.Background
Geology and History
Historically, people in Bangladesh retrieved most of their drinking water from surface water sources, particularly ponds. These were often reserved for this purpose and fenced off to keep them relatively clean. However, diarrheal diseases such as dysentery and cholera were widespread.
In the 1970s and 1980s there was a sustained campaign by the government and international donors, spearheaded by UNICEF, to promote tubewells.[6] A tubewell functions by virtue of a small diameter pipe drilled into the earth to the depth of the aquifer, enabling the user to draw up water by the suction mechanism of a pump (usually a hand pump). Tubewells were considered a relatively easy way of obtaining “safe water” uncontaminated by fecal matter and associated pathogens.
Driven by concerns over the safety of drinking water—as well as the practical convenience of having water sources near homes—the campaign to install tubewells was successful. By 1991, there were an estimated 2.5 million tubewells in rural areas of the country, providing drinking water for some 95 percent of the population.[7] About half of the people in rural areas were sourcing drinking water from public wells, the other half from privately installed wells.[8] There was a considerable decline in deaths from diarrheal disease in these decades.[9]
The number of shallow tubewells, including private wells, continued to increase. The price of a shallow tubewell with a common pump is within reach of many households even in poor rural areas.[10] Consequently, the overwhelming majority of tubewells in Bangladesh have been installed to a shallow depth—less than 150 meters, and often in the range of 20 to 50 meters. The primary exception to this situation is in the coastal areas of Bangladesh, where salinity in the shallow aquifer has meant tubewells have historically been installed to a depth of around 150 to 200 meters in order to reach fresh water.[11]
Thousands of years ago, rocks rich in arsenic were eroded from the Himalayas and deposited in low-lying areas which now make up West Bengal (in India) and Bangladesh. The current scientific consensus is that arsenic is released into the groundwater from these sediments by a natural chemical process called “reductive dissolution.”
In this process, arsenic—which is bound to iron oxyhydroxides—is released into the surrounding water when iron or manganese oxyhydroxides dissolve due to natural conditions that lead to a decrease in oxygen levels. These conditions are facilitated by microbial metabolism of organic matter contained in river floodplain and delta deposits.[12]
The chance of a well drawing groundwater contaminated with arsenic greatly depends on the depth of the tubewell: in general terms, the deeper the tubewell, the lower the concentration of arsenic.[13] During the initial explosion of the popularity of tubewells in Bangladesh, arsenic was not recognized as a problem in groundwater supplies.
An Emerging Problem
Doctors and researchers in India began to identify patients with arsenic poisoning in that country in the early 1980s.[14] Some also noticed cases of arsenic poisoning among people who had crossed into India from Bangladesh. One early case, in 1992, was described by researchers from the School of Environmental Studies (SOES) in Kolkata working in villages in West Bengal, the state adjacent to Bangladesh:
In one family, a woman who came to West Bengal from Bangladesh after her marriage had arsenical skin lesions, though others in the family did not show any symptom[s]. On being interviewed, the woman revealed that many of her relatives in Bangladesh had similar skin lesions. She further told that she had seen similar skin lesions among a few of her neighbors and also in some people living in two neighboring villages.[15]
In 1995, SOES hosted an important international conference in Kolkata on the subject, presenting conference participants with people with arsenic-related skin lesions from both West Bengal and Bangladesh.[16]
The conference triggered an active response. In the late 1990s there were a series of efforts to test wells across the country.[17] In 1998 and 1999, the British Geological Survey (BGS) conducted a rapid assessment survey of some 3,500 public tubewells used for domestic water supply across most of the country, reporting that 25 percent of all wells were above 50 micrograms per liter.[18]
What followed was one of the largest and most intensive water quality screenings ever to take place. The World Bank’s Bangladesh Water Supply Arsenic Mitigation Project (BAMWSP) included a coordinated effort which aimed to test every single well providing water for domestic use in 270 upazilas (sub-districts) across the country— covering an area home to around 65 million people.[19] This screening was mostly conducted from 2000 through 2003, though some testing continued until 2006.
Almost 5 million tubewells were tested by field testers who gave information about arsenic to tubewell owners and painted the wells based on the test results. By 2005, the spouts of 1.4 million wells that draw groundwater with greater than 50 micrograms per liter according to the field test had been painted red; another 3.5 million wells with arsenic up to 50 micrograms per liter had been painted green.[20]
In the early 2000s, the government and international donors made a significant commitment to tackle the problem. An Inter-Ministerial Secretaries Committee on arsenic met regularly during these years, supported by a National Committee of Experts on technical matters. The Secretaries Committee oversaw the preparation of the National Policy for Arsenic Mitigation and the Implementation Plan for Arsenic Mitigation, which the government adopted in 2004.[21]
Under BAMWSP, a National Arsenic Mitigation Information Centre (NAMIC) was established for collecting, storing, and disseminating information related to Bangladesh’s arsenic problem.[22] In 2003, an Arsenic Policy Support Unit (APSU) was established for coordinating the activities of the many organizations undertaking mitigation efforts and to support research and training around arsenic.
The BAMWSP project also involved identifying some 38,000 suspected arsenicosis patients from the 270 upazilas. The project supported the training of some 2,000 doctors and 12,000 health workers— although there was no specific treatment of these patients.[23]
Health Impacts
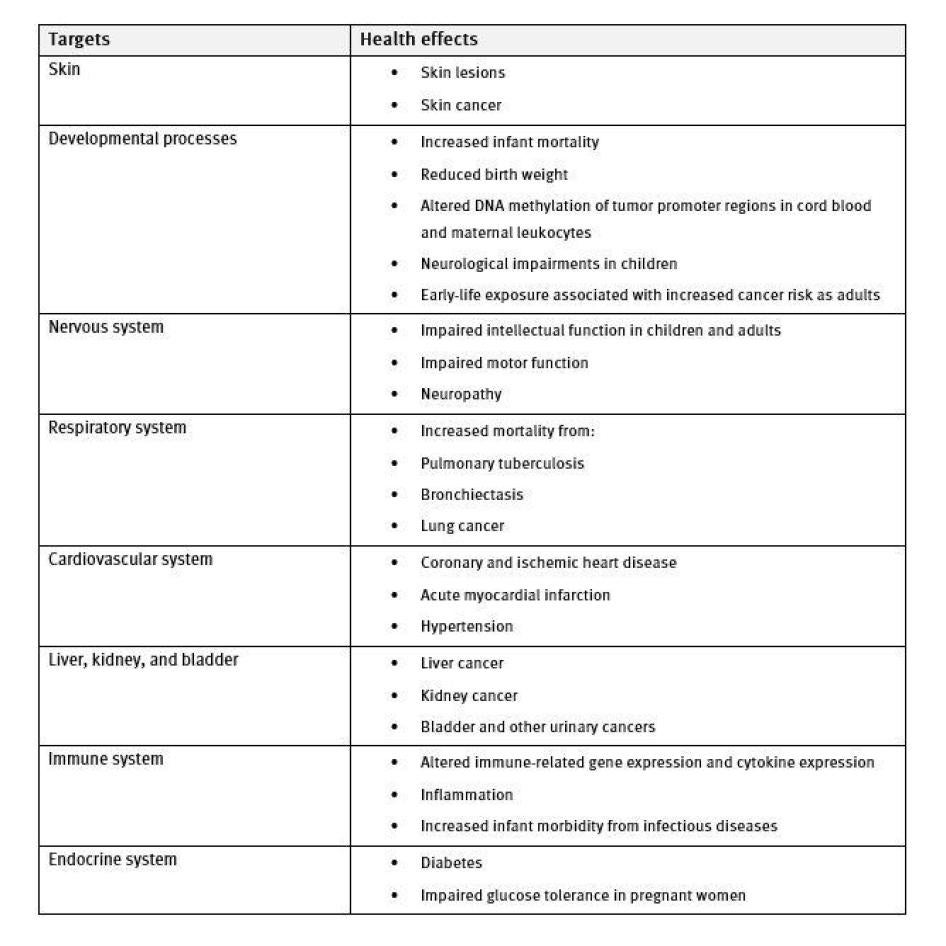
The health impacts of chronic arsenic exposure are extensive and wide-ranging: arsenic-associated health problems can affect nearly every major organ and system in the body.[24]
Although they may take years to develop, some symptoms are easily visible even to the untrained eye. Some people chronically exposed to high levels of arsenic will develop melanosis, essentially dark and/or light spots against the background skin. Often they have a distinctive “raindrop” pattern on the trunk of the body, arms, and legs.
Keratosis, a hardening of the skin often on the palms and soles, is also common. This condition can progress to scaly, nodular "corns" or "warts" on palms and soles. Skin lesions, which are easily infected and can be very painful, are common. Patients can also report general weakness, burning sensations, and chronic coughs.
There is a latency period to both melanosis and keratosis: these symptoms often develop some five to ten years after initial exposure, depending on the amount of arsenic ingested.[25] While skin abnormalities have long been considered hallmarks of chronic arsenic exposure, the vast majority of exposed individuals (even with high levels of chronic exposure) will not develop skin lesions but are still at risk of other diseases.[26]
The main causes of death from arsenic are cancers (of the lungs, liver, kidney, skin, and bladder), cardiovascular disease, and lung disease. Some of these diseases have even longer latency periods than skin lesions, meaning that many patients may not manifest symptoms for decades.
Arsenic increases the risk of cancer in the liver, kidney, bladder, and lungs. Skin cancers such as basal and squamous cell may also develop, in most cases from skin lesions.
Chronic arsenic exposure is associated with respiratory diseases, such as tuberculosis and bronchiectasis (where the airways of the lungs become abnormally widened, leading to a build-up of excess mucus that can make the lungs more vulnerable to infection). Long-term exposure to arsenic also increases the mortality rate from cardiovascular disease, in particular ischaemic heart disease (a blockage in the coronary arteries reducing the supply of blood to the heart) and other heart disease.[27]
Arsenic exposure is associated with increased infant mortality and, in some studies, increased spontaneous abortion and stillbirth, as well as reduced birth weight.[28] Exposure to arsenic can impair cognitive development in children.[29]
Exposure during pregnancy and childhood is associated with an increased occurrence and/or severity of lung disease, cardiovascular disease, and cancer in childhood and later in life, with evidence of decades-long latency periods for these health conditions.[30]
Arsenic’s effects on a broad range of organs and bodily systems[31]
Studies from both Bangladesh and the Indian state of West Bengal have shown that the impacts of arsenic exposure tend to be worse among people with a lower soci0-economic status.[32] This may be related to factors such as poor nutrition (the manifestation of severe skin lesions is associated with a lower body-mass index), increased water consumption (for example, among manual laborers), and the ability of wealthier families to afford to shift to alternative water sources.[33] The social and economic impacts of arsenic-related health conditions can be devastating for both the individual and their family. Death, illness, or severe weakness may affect an individual’s ability to earn a living at the same time as incurring considerable expenses, increasing the household’s poverty and ill health.[34]
There is no known cure for chronic arsenic poisoning. Avoiding arsenic contaminated water is essential. A focus on improving nutrition (through increased protein and vitamins) can help the body excrete arsenic. Treatment of painful symptoms, such as skin lesions, can help relieve pain and suffering. Early diagnosis and management of chronic diseases could improve and prolong the lives of people suspected of suffering from chronic arsenic poisoning. Accurate diagnosis of disease and its cause can also help relieve the trauma of illness.
Although ending exposure to arsenic is imperative, it does not end the risk of disease. Fatal arsenic-induced cancers and heart and lung disease can develop decades after exposure ends.
Policy Lethargy
Mitigation Efforts
There has been no national screening of wells since the BAMWSP effort ended in 2007 as planned.[35] Analyzing the data from the BAMWSP tubewell screening (the bulk of which occurred between 2000 and 2003) and adjusting the results to account for inaccuracies in the field test kit method used, researchers estimated that in that period approximately 20 percent of tubewells nationwide were yielding water with arsenic above the Bangladesh standard (50 micrograms of arsenic per liter of water.)[36] They calculated that 20 million people—about 14 percent of the national population—were drinking water in excess of the Bangladesh standard.[37]
Over 10 years later, some 20 million people continue to drink water above 50 micrograms per liter.
In 2013, a study reported 12.4 percent of some 13,000 water samples from households randomly selected across the country exceeded the Bangladesh standard of 50 micrograms per liter, while 24.8 percent of the population were above the WHO provisional guideline value.[38] With an estimated population of 157 million in 2013, the results indicate that 19.4 million were drinking water above the Bangladesh limit and 38.9 million above the WHO provisional guideline value.[39]
Various types of water points can be used for arsenic mitigation.[40] In general, the risk of arsenic contamination of drinking water from tubewells is greater the shallower the well. Deeper tubewells are a good arsenic mitigation tool and can supply drinking water that is generally of acceptable chemical and microbial quality for many years and serve more than one hundred people. [41] They also require less maintenance compared to other safe water devices such as pond sand filters and dug wells.
However, deep tubewells cost approximately US$850-950 to install, putting them beyond the reach of most individual households in rural areas.[42] Many households in rural areas must rely on the deep tubewells or other water points installed by the government if they are to avoid the high levels of arsenic found in shallow wells.
The Department of Public Health Engineering (DPHE) (under the Ministry of Local Government, Rural Development and Cooperatives) is responsible for planning, designing, and implementing water supply and sanitation services in rural areas. Some NGOs and international donors are active in the water and sanitation sector, but the government is responsible for the majority of public water sources (including deep tubewells) installed in Bangladesh.
Most DPHE programs are focused on expanding access to drinking water in all rural areas, not on arsenic mitigation in areas with a high level of arsenic contamination.[43] As a result, there is insufficient targeting of arsenic mitigation in those areas of Bangladesh that need it most. As early as 2005, a DPHE review recognized this. A review of government-installed water points found:
[T]he highest proportion of water supplies have been installed in areas with less than 40% of tubewells contaminated [with arsenic], followed by those with 40-80% contaminated and the areas with over 80% tubewells contaminated. The water supplies in the areas with less than 40% tubewells contaminated have primarily been installed in general water supply programmes, which would account for the larger number.
The data on mitigation option[s] should be kept in the context of the relative populations.… Nonetheless, the data indicates that the worst arsenic affected areas have not had sufficient priority to date.[44]
A later DPHE review of progress published in 2010 found strikingly similar results. It concluded there was “a tremendous gap between the number of installed safe water options and the areas with high arsenic contamination.”[45]
The review found that of the approximately 700,ooo active water points installed by the government up to 2009, 420,ooo had been installed in administrative unions where arsenic contamination was less than 20 percent of water points. The majority of those water points installed by the government (approximately 360,000) were shallow tubewells.[46]
Some of these are used by poor villagers, although this use is constrained by the fact that the poorest of Bangladesh’s villagers lack land on which to install the well. But the effect of the policy of installing shallow tubewells in areas where the risk of arsenic contamination is low is that there are less government resources available to mitigate arsenic exposure in areas where the risk of arsenic contamination is high.
Even when installing water points intended to mitigate arsenic exposure (primarily but not exclusively, deep tubewells), DPHE has also installed them through general water supply programs. As a result, even deep tubewells have been poorly targeted to those areas where the risk of arsenic contamination is high.
For example, of the approximately 164,ooo deep tubewells installed by DPHE up until 2009, 52,000 were installed in unions where less than 20 percent of water points were contaminated with arsenic, while just 38,000 were located in those unions where more than 80 percent of water points are contaminated by arsenic.[47]
Meanwhile, much of the administrative infrastructure built by the government and international donors to address arsenic in drinking water from 1998 to 2006 no longer exists: NAMIC was closed at the end of the World Bank’s project in 2006, the APSU closed around the same time. The Inter-Ministerial Secretaries Committee no longer meets.
While government water points are generally tested following installation, the overwhelming majority of private tubewells installed after the BAMWSP testing finished—over 10 years of installations—have never been tested.[48] The common figure given for the number of shallow tubewells across the country is about 10 million, although the estimate is a crude guess.[49]
In Bangladesh, many people drinking water with elevated levels of arsenic are unaware of arsenic in their wells. Some rural villagers may be drinking water from wells that have been tested, but may have forgotten or no longer care about those test results. Few, if any, public awareness campaigns exist to reinforce messages about the health dangers of arsenic.
Others are drinking water from wells that have never been tested. They may suspect a well is safe—or contaminated. But even if rural villagers are concerned by the possibility of arsenic in their drinking water, they have no easy access to arsenic testing services to test their water. [50] There is no clear plan or process for tubewell rehabilitation for people who find their public or private well is contaminated.
The Health Response
The Ministry of Health and Family Welfare is responsible for policy formulation, budget development, financial allocation, and monitoring health service programs. The ministry’s Directorate General of Health Services (DGHS) is tasked with implementing health service programs.
Bangladesh’s health system identifies people suffering from arsenic-related health conditions via readily visible symptoms of skin lesions. The DGHS reports that in 2012 there were 65,910 “arsenic patients” in Bangladesh.[51]
The government identifies “arsenic patients” by a particular set of dermatological symptoms. However, as noted above, long-term exposure to arsenic produces enormous health impacts far beyond skin lesions. The Bangladesh government does not attempt to measure these deaths or serious illnesses caused by arsenic.
A number of academic studies have attempted to measure the excess mortality caused by exposure to arsenic across large populations. One study analyzed mortality data over a decade for a cohort of 115,000 people. It found that exposure to arsenic above 10 micrograms per liter in drinking water accounted for considerable excess mortality among adults in rural Bangladesh.[52]
Another study analyzed mortality data over a 10 year period among 11,000 people. They found that 21 percent of all deaths in that population could be attributed to arsenic exposure above 10 micrograms per liter in drinking water. [53]
Other researchers applied the risk of deaths from arsenic exposure identified in these two studies, as well as exposure findings from 2009, to estimate an annual death toll of 43,000 people from arsenic-related illnesses in Bangladesh each year. [54]
|
Bangladesh’s safety level for arsenic in drinking water WHO reduced the guideline value for arsenic in drinking water from 50 to 10 micrograms per liter in 1993.[55] WHO considers the guideline provisional because of measurement difficulties and practical difficulties in removing arsenic from drinking water.[56] A number of countries have since lowered their permissible limits to 10 micrograms per liter, and some have established lower standards. Bangladesh maintains a standard of 50 micrograms per liter. However the evidence for considerable death and illness from exposure to arsenic in drinking water between 10 and 50 micrograms in Bangladesh is increasing.[57] In their estimate on the excess mortality from arsenic exposure, Flanagan and others noted that “the excess deaths among people exposed to arsenic concentra¬tions of 10–50 micrograms per liter (below the national standard) represent from 45% to 62% of all arsenic-related deaths.”[58] |
II.Findings
Ongoing Exposure
Government Water Points at the National Level
DPHE is responsible for overseeing the installation of new water points in rural Bangladesh. While there are a variety of water point technologies, the majority that the government installs are deep tubewells and shallow tubewells.[59]
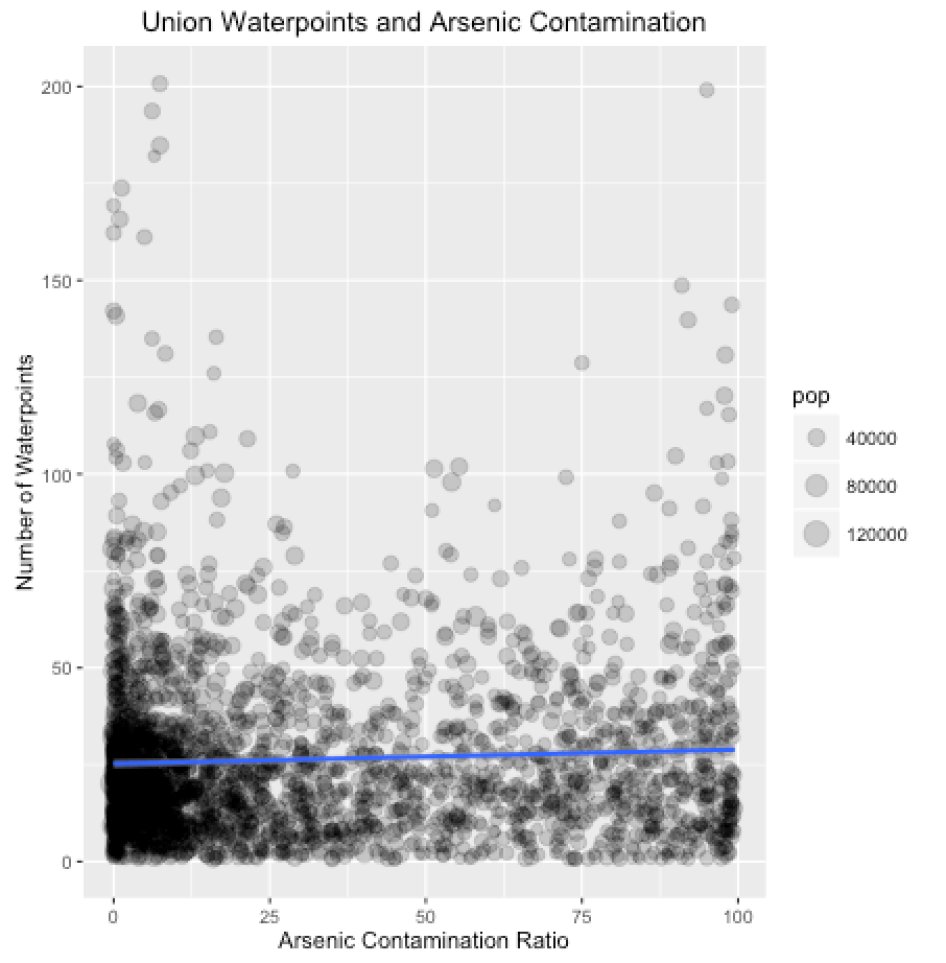
Human Rights Watch’s analysis of approximately 125,000 government water points installed between 2006 and 2012 (and tested under the Nationwide Water Point Mapping Programme (NWMP)) finds that government water points have not targeted areas where the risk of arsenic contamination is high.
If the government wastargetingwater pointinstallations to areas with high levels of arsenic contamination, the above graph would show administrative unions plotted in a general trend from the top right corner to the bottom left. Instead, the graph depicts little organization or structure. Correlation tests show that there is no relationship between the number ofwater pointsrecently installed and the level of arsenic contamination (Pearson coefficient = 0.051. The coefficient is measured on a scale of 0 (no relationship) to 1 (perfect relationship).
One potential justification for this lack of prioritization of arsenic affected areas is that government water points are targeting those rural areas most in need of safe water (regardless of the issue of arsenic). However, Human Rights Watch’s analysis of government water points installed between 2006 and 2012 shows that government water points are not targeting areas where existing coverage by safe water points is low.
If the government was installing morewater pointsin unions with low safe water coverage, the above graph would show unionsplotted in a trend from the upper left corner towards the lower right corner. Again, the plots show randomness. There is no statistical relationship between safe water coverage andwater point installation (Pearson coefficient = 0.081).
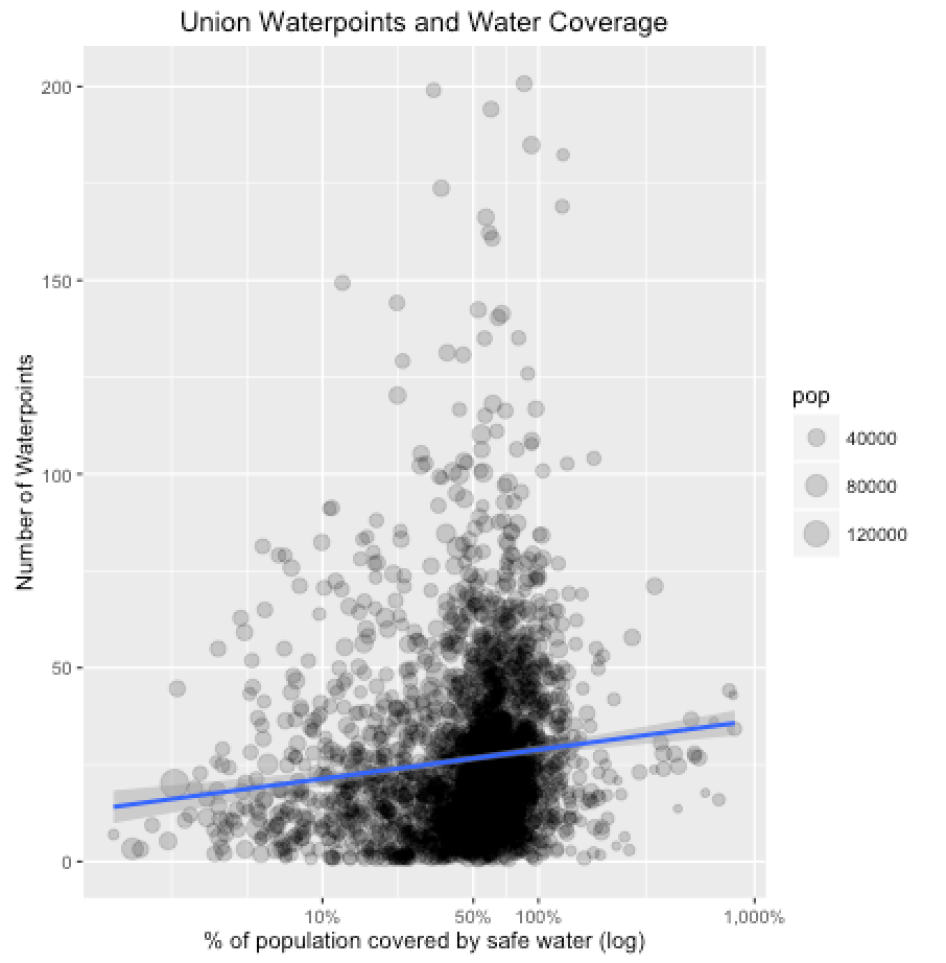
Another justification for this lack of prioritization may be that the government is simply placing water points in administrative unions with large populations. If this were true, both of the above graphs would show larger circles at higher points along the y-axis and smaller circles plotted towards the bottom of the graph. This is not the case. In fact, a correlation test shows no relationship between union population size and the number of water points recently installed (Pearson correlation coefficient = 0.177).
In sum, this data shows the government is expending considerable resources in areas where the risk of arsenic contamination is relatively low and where water coverage is relatively good. Consequently, government resources left to mitigate arsenic exposure are severely diminished without a clear rationale.
As noted in the Background section of this report, at least two previous government reports criticized the government’s lack of targeting of areas of the country most in need of arsenic safe water points.[60] Despite these government reports stating that the government should do a better job of targeting arsenic mitigation options in the areas where they are most needed, it inexplicably fails to do so. In January 2016, Human Rights Watch wrote to the government to ask the reason for this approach, but no reply had been received at time of publication.
Government Water Points at the Village Level
Human Rights Watch identified 56 government-installed water points in the five villages where it undertook research. Of the total 56 government-installed water points, 23 were both functional and accessible. However 18 were permanently non-functional (and hence no longer used), and 15 were functioning but located inside the perimeter of the caretaker’s property.[61]
One village (Balia) had all government-installed water points functioning and publicly accessible. The high rate of functioning deep tubewells in Balia reflects the fact that Balia is 80 kilometers from the sea and the coastal zone of Bangladesh has traditionally relied on deep tubewells because of salinity in the groundwater.
Two villages (Iruain and Tilchandi) were without any government-installed functioning and publicly accessible water points.
In many cases, the caretaker had paid the government’s up-front contribution himself or herself—and, as detailed below, sometimes considerably more. The tubewell may have been installed on his or her land. As a consequence, many caretakers consider themselves the de facto “owner” of the public water point.
The extent of restrictions on access to these water points varies depending on individual caretakers. Some caretakers declined to describe how many people use the water point in practice. Restrictions on wider use of government water points appear common. In 7 of the 15 water points located inside the caretaker’s property, the caretaker or the caretaker’s family member stated that the water point was only used by the caretaker’s immediate family (typically around five individuals).[62]
More complete tables are included in Annex 5.
|
Village |
Government water points |
Functioning and accessible |
Not functioning |
Inside caretakers perimeter |
Government claimed contaminated |
|
Balia |
9 |
9 |
0 |
0 |
|
|
Bilmamudpur |
16 |
10 |
1 |
5 |
5 |
|
Ruppur |
18 |
6 |
6 |
6 |
|
|
Iruain |
12 |
0 |
8 |
4 |
|
|
Tilchandi |
1 |
0 |
1 |
0 |
Contaminated Drinking Water
Shuta lives in Iruain. There are 13 people in her household. Both her palms are covered by thick, yellow skin and the backs of her hands, the tops of her feet, and the skin of her forearms is patchy. She suffers pain from wart-like nodules on the soles of her feet that make it very painful for her to walk barefoot. She also complains of an itchy, burning feeling on her skin, which feels more intense on hot summer days.
When describing the impact of arsenic on her village, Shuta points quickly in various directions, explaining “so many people from our village have died because of arsenic—one person in this direction, two in that direction, another two women from over there.” She knows that the water she collects for her family contains a dangerously high level of arsenic. Shuta told Human Rights Watch:
There’s a well about three minutes-walk away that is supposed to be low in arsenic so I try to drink from that. It was tested a few years ago by an NGO: they said it is a bit safer but not safe. It is painted red. A lot of people use it, we have no other option. There are no government wells that work, none at all.[63]
Dupur, in her early 30s, lives in the same village, Iruain. A widow with three children, the youngest of whom was just eight months old when Human Rights Watch talked with her, she has known that her family’s drinking water is contaminated with a dangerously high level of arsenic ever since an NGO tested the tubewell from which it is drawn.
Dupur began noticing patchy spots on her skin when she was pregnant with her most recent child. Worried, she went to see a doctor at the upazila (sub-district) health complex, who told her that it was important that she begin to avoid drinking water with arsenic in it. However she explained to Human Rights Watch that she is unable to follow this advice because “there is no government tubewell around here that works.” Dupur is acutely worried for her health and her children’s health:
I have begun to give my [eight months old] daughter water to drink directly. If there was a government tubewell I could use, even if it was far away, I would go there for my sake and also my daughter’s sake.[64]
Khobor (see the Summary section) lives in Bilmamudpur and supports his wife, two sons, and daughter by working as a farmer. When he spoke with Human Rights Watch he expressed anxiety about patchy marks that had recently appeared on his body and his feet—a fear heightened by the fact that both his parents died in the last three years with similar marks all over their skin. The tubewell that he and his family use for drinking water had been tested both by an NGO and by the government; they told him the test results were around 250 micrograms per liter:
The NGO and the government people told us not to drink the water but we have no other options. When it rains we collect the rainwater, but we only have one large bucket and one clay pot to store water in so the rain water lasts one or two weeks at most. There are no government-installed water sources in this area. Look at my children! Even if we feed them as best we can and look after them well, they will fall sick from arsenic in the water.[65]
Balish, in his mid-60s, works as a farmer and also lives in Bilmamudpur village. There are six people in his household. He has dark spots across his chest and the backs of his hands, and thick skin on the palms of his hands. He told Human Rights Watch that three people in his household had died of arsenic-related problems about 10 years ago, with spots on their bodies and feet that he described as swollen and cracked. He recalls that an NGO had tested his household’s tubewell in about 2006 and told him it contained 450 micrograms of arsenic per liter of water.
The same NGO that tested his tubewell installed a rainwater harvesting system for his house; it is only one of two such household systems in the local neighborhood. In this system, rainwater that falls on the corrugated tin roof of his house is collected by gutters and pipes and stored in a large concrete tank beside the house. Balish expressed frustration at the lack of safe water devices in his village:
We drink rainwater during the monsoon and for three months afterwards. Then we have to drink tubewell water with arsenic in it. The rainwater tank only holds 2,000 liters. If our rainwater harvester was bigger, or if there were more of them, it could help many more people around here.
Bailash was nevertheless grateful to the NGO who had installed this partial solution, but complained there was no government assistance to his neighborhood:
I’ve never seen a government person helping us with safe water in this neighborhood of the village. The government could try to dig more tubewells or build more rainwater harvesters. They could try piped supply water, or build ponds that give arsenic free water. But here the government is not even trying.[66]
Agrahayan, in his mid-50s, lives in Ruppur village in a household with six other people. He has white and black spots across chest. He complains of a chronic cough:
There are many people with arsenic [related] problems in this part of the village but there are no government tubewells here. There’s a tubewell behind my house that’s one of the worst in the village for arsenic. I use it sometimes, when I don’t have time to go to my brother’s tubewell. If I need a glass of water at night, would I walk to my brother’s house for a glass of water? After all, I’m not sure my younger brother’s tubewell is safe: I don’t know if it was tested and it isn’t painted.[67]
Shada, in her early 60s, lives in Tilchandi village. There are seven people in her household and she shares the housework with her two daughters. Her hands and feet are marked by strong, dark spots. She says that many days she feels a strong itching across her torso and in her hands, a sensation that becomes more intense in hot weather:
I have a tubewell inside my house and drink water from it: it is marked red. There are some tubewells marked green in this village but it would take over 10 minutes to walk to them. There are no government wells in this village. If the government gave us a well with safe water we could save ourselves and our children from these sorts of illnesses.[68]
Shada’s neighbour, Purono, is in her late 40s. She told Human Rights Watch that Tilchandi had a functioning government-installed tubewell near the local primary school that many hundreds of villagers used to use each day “because there are so few good wells in this village.” However, “it broke down many years ago and they never came to fix it”.[69]
Contaminated Drinking Water from Government Tubewells
In Bilmamudpur, three caretakers of government tubewells and one person suspected of suffering arsenic-related health conditions told Human Rights Watch that government officials had informed them, since installation, that those tubewells were contaminated with arsenic.[70]
All four government tubewells were still in use for drinking water purposes. Only one was painted red, three were unpainted. Two (including the one that was painted red) had a government water point code attached to the tubewell, the other two did not. Only one of those two codes was contained in the Nationwide Public Water Point Mapping database (despite the missing tubewell being installed during a year supposedly covered by that database.)
This is not an exhaustive list of government tubewells in Bilmamudpur contaminated with arsenic. There may be more, such as contaminated tubewells that have not been tested by the government following installation, or contaminated tubewells where caretakers of government tubewells have not been informed of test results.
Biroho is a man in his late 30s living in Bilmamudpur. There are eight people in his household and he makes a living selling construction materials. He has dark spots on his chest, back, arms, and calves, and thickened skin on his palms. He also suffers from a chronic cough. Biroho’s house is beside a tubewell that was installed by DPHE in 1995. It is unpainted. He told Human Rights Watch:
People say it’s 150 or 200 meters deep but I’m not convinced. The well was tested when it was installed and then again in 2002 or 2003. The result was 150 micrograms per liter in 1995 and the second time they tested it they also said it was 150. They asked us not to drink the water, but where else should we go? We received no filters. We have subsequently bought a filter ourselves but it only filters iron not arsenic. Currently this tubewell is used by 5 or 6 families around here, maybe 40 to 50 people in total.[71]

The caretaker of another government tubewell described to Human Rights Watch a similar scenario. He was caretaker of a government tubewell in Bilmamudpur that was painted red; the pump bore the mark of the DPHE’s Special Rural Water Supply Program. He explained:
It was installed about three years ago. People from DPHE came and said not to drink from it. But we drink from it directly. There are three houses nearby who use this, maybe 30 people drink from it. No one around here has any arsenic filters.[72]
For three of the four government tubewells identified in this way, field tests of the water performed for Human Rights Watch by a trained technician confirmed what the villagers had been told: that the water was contaminated above the Bangladesh standard. Field tests gave results of 500 micrograms per liter, 300 micrograms per liter, and 200 micrograms per liter. (The tubewell owner of the fourth government tubewell declined permission to test the water, explaining that there was no point as he already understood the water was contaminated).
Two of the government tubewells identified in this way had a unique national water point code attached to the tubewell. One of these codes matched with a code from the Nationwide Public Water Point Mapping database which recorded (as the caretaker had claimed) that the tubewell was indeed contaminated with arsenic. For an unknown reason, the other code was not included in the database despite being installed during a year supposedly covered by that database.
The two water point codes of government tubewells where the caretaker (or a family member of the caretaker) told Human Rights Watch that the government had informed them that the tubewell was contaminated are:
|
Government water point code |
Government result |
|
2011-1-01-04-29-47-13-00-001 |
100 micrograms per liter |
|
2011-1-01-04-29-47-13-00-021 |
Not included in database |
This is not an exhuastive list of the government tubewells in Bilmamudpur contaminated with arsenic; there may be more.
Human Rights Watch wrote to DPHE in January 2016 explaining that villagers in Bilmamudpur claimed that government officials had informed them, following installation, that (at least) four government tubewells were contaminated with arsenic and that, in all cases, the tubewells were still in use. By the time this report went to print Human Rights Watch had not received a response.
Arsenic contamination of government-installed water points does not reach the scale of arsenic contamination in the considerably larger number of privately-installed tubewells across the country. However it is a significant issue.
According to Human Rights Watch’s analysis of approximately 125,000 government water points installed between 2006 and 2012 and tested under the Nationwide Waterpoint Mapping Programme (NWMP) in 2013, some 5,000 government water points installed were contaminated with arsenic above the Bangladesh standard of 50 micrograms per liter. The proportion at which these water points are contaminated is around 5 percent. [73]
Human Rights Watch wrote to DPHE in January 2016 enquiring what steps, if any, the government had taken to replace or rehabilitate these contaminated water points. By the time this report went to print Human Rights Watch had received no response.
Human Rights Watch wrote to UNICEF in February 2016 for further information on this matter. This correspondence, and UNICEF’s reply, is attached as an annex to this report [see Annex 3].
In correspondence to Human Rights Watch, UNICEF’s chief of water, sanitation and hygiene in Bangladesh confirmed that of 20,597 wells installed with UNICEF support under the SHEWA-B project (2006-2012), 1,733 were subsequently found to be contaminated with arsenic above the Bangladesh standard of 50 micrograms per liter.[74]
The contamination of UNICEF-supported wells installed from 2008-2012 was identified by follow-up testing in 2012-2013. The initial monitoring protocol for the project included water quality (for iron and arsenic) among its indicators. However it appears that, at least in some cases, there were irregularities with the water samples submitted by government contractors for initial testing. UNICEF’s correspondence to Human Rights Watch noted:
An assessment by UNICEF and the Department of Public Health Engineering (DPHE) to determine why some DPHE-UNICEF supported water points were contaminated recognized that a specific clause in the government’s drilling contract stipulates ‘no success, no payment’ which made the contractor liable for arsenic contaminated water points. This clause may have discouraged a transparent and honest process of collection and submission of water samples for testing.
UNICEF’s correspondence to Human Rights Watch also noted that “UNICEF undertook necessary actions to rehabilitate/replace 1,733 wells and completed the project in September 2015.”
UNICEF subsequently supported the government of Bangladesh to conduct a nationwide mapping of water points installed by the DPHE between 2006 and 2012—the initial survey of the Nationwide Waterpoint Mapping Programme (NWMP). The survey of approximately 125,000 water points represented around 85 percent of water points installed by the government during this period.[75]
That review revealed that a further approximately 5,000 water points were contaminated. According to UNICEF, these were “marked [red] in compliance with the UNICEF-advocated strategy.”[76] However, as noted above, there is also no indication that the government has taken any steps to replace or rehabilitate these contaminated water points.
Human Rights Watch also wrote to the World Bank in February and March 2016 to request further information on this matter. This correspondence and the World Bank’s replies areattached as an annex [see Annex 4].
Under the World Bank’s Bangladesh Water Supply Program Project (BWSPP) (2004-2010) some 13,000 rural water points were installed by the government with the bank’s support. Human Rights Watch has no indication that water points installed by the government with World Bank support were contaminated with arsenic. However, in correspondence to Human Rights Watch, the World Bank country director stated:
The Department of Public Health Engineering (DPHE) tested all public wells installed during 2006-2012. Around 5,000 of 125,000 public wells were found to be contaminated. This may include some BWSPP wells although DPHE did not identify them as such. All these 5,000 wells were painted red to show they are unsafe and there is a high level of community awareness that red wells are unsafe for drinking water. The ongoing Bangladesh Rural Water Supply and Sanitation Project (BRWSSP—2014-2017) has introduced improved water quality monitoring protocols.[77]
In an email to the bank’s country director, Human Rights Watch expressed the significant limitations to this DPHE testing process.[78] The data did not include information on whether bank-supported water points are among those that are contaminated. In addition, the DPHE testing of approximately 125,000 water points covers only 85 percent of all government wells (and none that were built before 2006).
According to Human Rights Watch’s research in Bilmamudpur, not all contaminated government water points are painted red. As discussed above, marking contaminated wells red does not in practice prevent people from using water points for drinking water— particularly where there are few or no tested and marked safe water points in the immediate vicinity. As such, it is a deeply inadequate step to ending exposure.
Human Rights Watch recommended that the bank itself should promptly and thoroughly review whether bank-supported water points are indeed contaminated and should take steps to replace or rehabilitate any that are. These steps are important, in part, because of the bank’s ongoing support to the government on this issue. Under the World Bank’s Rural Water Supply and Sanitation Project (2012-ongoing), the bank envisages support to the government in installing a further 14,000 rural water points.
In a letter received by Human Rights Watch shortly before this report went to publication, the World Bank’s country director stated:
We fully agree with your recommendation for undertaking a review into whether any of the bank-supported water points under the Bangladesh Water Supply Project (BWSPP) are contaminated. In this regard, we look forward to working with the Department of Public Health Engineering (DPHE) to systematically identify the wells (if any) from their screening results.
The World Bank is also considering a separate review to identify if there are contaminated BWSPP wells if DPHE cannot identify the contaminated BWSPP wells. The review will be helpful to provide more information about the sustainability of interventions, including: (i) current water quality; (ii) number of users; (iii) distance to the nearest alternative safe devices; (iv) awareness of arsenic risk; (v) GPS mapping; (vi) breakdown history; (vii) attitudes and mitigation seeking behavior; and (viii) satisfaction. Based on the results of the review, we would decide whether further action is needed subject to discussion and agreement with DPHE.[79]
Human Rights Watch encourages the bank to promptly undertake the separate review, with water quality testing being a core component, and rehabilitate or replace any water points found contaminated.
Human Rights Watch also welcomes the steps described in the correspondence from both UNICEF and the World Bank to improve protocols for the monitoring of future projects.
No Well Testing or Awareness Activities
It has been at least 10 years since arsenic people came from the government to conduct tests and paint the tubewells red or green. I wish they’d come back and do their job properly.
—Agrahayan, a man in his mid-50s who lives in Ruppur[80]
Dhaan is a man about 30 years of age who lives in Bilmamudpur. He works as a security guard in a local school. He has dark spots on his back and feet. He lives with his parents, his wife and his two children, the youngest of whom had just been born in the weeks immediately before Dhaan spoke to Human Rights Watch.
My family gets its water from a private well we put in about 10 years ago. It’s not been tested. No one from the government has ever been around here and it’s not been tested by anyone else. I’m worried it might be high in arsenic, above all for my new-born child: if his generation is affected like ours, it will be a disaster.[81]
In other villages, people remembered the government’s blanket screening of tubewells in their village, but draw their drinking water from wells that have been installed since then. Astha, about 40 years old, lives in Ruppur. She and the members of her household draw water for drinking and household uses from a shallow tubewell beside their house that they had installed about four years ago.
I don’t know if it’s safe to drink or cook with this water, my well has never been tested. The government people who do tests haven’t come to this village since we have had the tubewell installed. They haven’t come for at least 10 years. I’m scared of the water but what can I do?[82]
Chaabi is a woman in in her mid-40s who lives in Iruain. There are 10 people in her household. She has had difficulty breathing and problems with her vision for the last eight years. She recalls an earlier period of government screening and notification of tubewells in Iruain.
Earlier there were a lot of government activities: officials came here and they went house to house to test the water and mark the tubewells and to talk to us about our drinking water. I don’t know why, but people from the government haven’t come for many years, maybe 10 years or more.
After the screening program in her village, Chaabi learned that three tubewells around her house were supplying drinking water with a dangerously high level of arsenic. Her husband installed a new tubewell, at a slightly greater depth than the others (20 meters, not 15 meters). Chaabi uses the new well for all drinking and domestic use. The new well has never been tested. Chaabi shrugs and admits “I hope the new well is OK, but I really don’t know.”[83]
In theory, if villagers take a water sample to DPHE offices in their local upazila (sub-district) city or town, those offices can test the water for arsenic using field kits. It appears to be an ad hoc arrangement, with test kits supplied to DPHE offices on a sporadic basis and no one particular DPHE staff person tasked with performing the test.
In practice, many villagers do not know this option exists. For example, when Human Rights Watch asked Astha (whose evidence appears above) if she had taken water samples to the DPHE technicians to get them tested, she replied:
I don’t know how to do this or where to take it. I didn’t know that they test water, so how could I go there?[84]
Some DPHE officials also told Human Rights Watch that even if villagers travelled to the DPHE offices with a water sample, they did not currently have the capacity to perform tests.
If any people come to us with water samples, we have to send them away. All our [field test] kits are expired by now- they expired three months ago. There are always these administrative problems.[85]
Political Interference in Government Allocations
This [political interference] happens all over Bangladesh.
—DPHE official, Bangladesh, 2015[86]
If the member of parliament gets 50 percent [of the allocation] and the upazila chairman gets 50 percent, there’s nothing left to be installed in the areas of acute need.
—DPHE official, Bangladesh, 2015[87]
According to government policy, poor people should be prioritized during the allocation of government tubewells. For example, the Sector Development Plan for Water Supply and Sanitation (2011-2025) states:
During the short ‐term period, the aim is to provide, at least, the basic minimum water and sanitation services for all, particularly the poor and vulnerable groups.[88]
Bangladesh’s Pro Poor Strategy for Water and Sanitation Strategy Sector defines a “basic minimum level of service” as 20 liters of water (for drinking, cooking and personal hygiene) per person per day, where the water meets national water quality standards and the water source is within 50 meters of the household.
The policy establishes a formula for identifying clusters of households of poor villagers where that basic minimum level of service is not met, and provides that such clusters “will get priority in having community water points from the Department of Public Health Engineering or other development partners.”[89]
However, it is not clear how this policy is implemented in practice (if it is at all), nor how it relates to the policy of allocating new government water points.
According to Bangladesh’s Implementation Plan for Arsenic Mitigation (2004), locations for new safe water sources should be determined by Arsenic Mitigation Committees at the upazila (sub-district), union, and ward (village) levels. The ward (village) committee should decide the exact location of each water point within the ward, overseen by the union and upazila (sub-district) committees.[90] More recent DPHE projects have given the responsibility for locating new safe water sources to water and sanitation (WATSAN) committees at the upazila (sub-district), union, and ward (village) level.[91] In practice, these committees are often non-functional.
In many cases, the allocation of safe water points to those most at need may be undermined by nepotism by political representatives. A public DPHE report from 2010 alludes to this influence: it acknowledges “a tremendous gap between the number of installed safe water options and the areas with high arsenic contamination” and lists various institutional and technical difficulties that cause this gap. Among the institutional issues the report recognizes:
…sometimes influential or elite person [sic] influence the site selection process resulting in selection of less priority areas.[92]
Such interference is a highly sensitive topic for DPHE officials and some agreed to discuss it with Human Rights Watch only on the condition of anonymity. According to DPHE officials, the main people who interfere in the allocation process are parliamentarians and upazila (sub-district) chairmen who decide many—and in some parts of the country, all—locations of new DPHE water points.
Political interference happens by various means and to different extents across the country, but DPHE officials described a practice that is widespread and pervasive.[93] In the words of one experienced DPHE official, who spoke to Human Rights Watch on condition of anonymity, “this happens all over Bangladesh.”[94]
In at least one recent major government water supply project, the influence of members of parliament was formally recognized in official policy. The allocation process for new water points under Bangladesh’s Special Rural Water Supply Project (SRWSP) (2010-2015) was governed by a memo drawn up in November 2011 following a meeting of Local Government Department officials.
The memo stipulates that safe water options should be installed on a priority basis in poor communities. However the memo also directs that “50 percent of the sites for allocation should be finalized after discussion with the relevant Member of Parliament of that area.” The SRWSP memo is reproduced in Annex 1.
The SRWSP director, a DPHE official, sent written instructions concerning annual allocations of new water points under the project to DPHE field offices. The instructions explicitly invoke the memo and stress the role of members of parliament in deciding the locations of safe water devices:
According to [the memo] sources of water should not be installed for individuals but for communities. In addition, special importance should be given to ensuring that the very poor communities get access to the water. Where there is inadequate access to clean water the installations should be done on the basis of necessity and the WATSAN committee should make the ultimate decision regarding the location of the water supply allocated under the Annual Development Plan. However, 50 percent of the sites for allocation should be finalized after discussion with the relevant Member of Parliament of that area.
A DPHE official, who spoke to Human Rights Watch on the condition of anonymity, confirmed the role of the local member of parliament in the allocation process in his district. He shared with Human Rights Watch a letter that the parliamentarian sent to his DPHE field office in 2010.
Written on the letterhead of Bangladesh’s National Parliament and signed by the member of parliament, it was addressed to the executive engineer of the district DPHE office. The letter listed the names of 25 people living in an upazila (sub-district) “under my electoral area where deep tubewells need to be installed”.[95]
DPHE officials explained that members of parliament can sometimes decide more than 50 percent of annual allocations. A different DPHE assistant engineer explained:
According to our policy, the member of parliament is supposed to take only 50 percent [of new allocations] and the WATSAN Committee has [the remaining] 50 percent. But in this upazila (sub-district) the member of parliament decides 100 percent. We receive a list of where to install the tubewells. The initial list might have more than the allocated number of tubewells: in that case, the member of parliament will [later] send us a shorter list.
Many DPHE officials also explained that, along with members of parliament, upazila (sub-district) chairmen can also hold considerable sway over the allocation of safe water points.[96]
One DPHE official showed Human Rights Watch written records of annual allocations of new tubewells for one particular upazila (sub-district), for three consecutive years. The first year showed a total number of allocated tubewells of around 45 (the exact number is not included here). Handwritten in the margins of the DPHE allocation record was the sentence: “Around 15 (the exact number is not included here) are reserved for the Honorable member of parliament and the Honorable Upazila chairman.”
The allocation records of the subsequent two years showed a similar proportion of the total tubewell allocations “reserved” (in roughly equal proportions) between the member of parliament and the upazila chairman. The official considered his situation relatively fortunate, given that the member of a parliament in a neighboring area decided 100 percent of new allocations.[97]
Another DPHE official from a different district spoke of his frustration at the way safe water sources are allocated. He gave an example from one year that he considered representative of the general allocation process:
In 2013, we had an allocation of [approximately 100] tubewells from two projects and that year they were split 50-50 between the member of parliament and the upazila chairman.
All DPHE officials who spoke to Human Rights Watch were adamant that allocations of tubewells by members of parliament and upazila chairmen were to reward political support, not on the basis of actual need for arsenic safe water. One DPHE official, working in an upazila (sub-district) where 100 percent of allocations were decided by the local member of parliament, said: “The tubewells are for party members and other people he favors.”[98]
Another DPHE official, working in a different upazila (sub-district) (where the allocation is usually split 50/50 between the member of parliament and the upazila chairman) explained:
Site selection of new tubewells is essentially all about politics. They give them to their political allies, their supporters, those close to them or those who work for them. It is very frustrating, they don’t consider the real needs of the people. We know they’re not going to those who really need them because we have mechanics in the field. Our mechanics tell us “Some guy made some phone calls to the member of parliament and got a tubewell.” The tubewells don’t reach the hardcore poor.[99]
Yet another DPHE official explained:
Normally, a member of parliament will give tubewells to supporters of his or her political party. One time I went to see the upazila chairman at his house and said we should allocate on the basis of need. I said “Look, there are so many patients!” But he did not respond.[100]
Diverted Tubewells
Many people suffering suspected arsenic-related health problems who talked to Human Rights Watch had no inkling of how to request a government water point in their village. Bhadro, in his mid-30s, lives in Tilchandi. He supports his wife, son, and daughter as a farmer. He had black spots across his chest and dark, thickened skin over most of his palms. He told Human Rights Watch:
There are no government-installed tubewells in this village. They installed one in the nearby school but it hasn’t been working for years. They don’t give them to us but I don’t know why. I don’t know who to ask or how to ask.[101]
Other people expressed frustration at not knowing where government tubewells are actually located in their village. Khaddro, is a farmer in his late 30s who lives in Ruppur village. He told Human Rights Watch:
There are so many people with arsenic [related] health problems around here but people with just a little bit of political connection get the tubewells, not the patients. Many government tubewells are installed in private homes: the owners bribe government people or use their political connections. We don’t even know where some of them are, they’re so secretive. It makes me very angry to think about this.[102]
Many caretakers spoke openly about how they had received a government water point. Many described a process of requesting a tubewell that was consistent with DPHE policy: prospective caretakers gather signatures from neighbors and apply in writing to a local political representative (often a union chairman or union member) and then, if the application is successful, deposit an official contribution amount into a government bank account.[103] A team of mechanics and laborers contracted by DPHE then come to install the water point a few months later.
Human Rights Watch spoke to a small number of caretakers who confirmed that they had received government tubewells through their political connections. Others declined to answer questions on how they had received a government water point.
Human Rights Watch spoke to a caretaker who was also employed as a government functionary. He claimed to have paid 29,000 taka (approximately US$375) for a deep tubewell that, when it was seen by Human Rights Watch, was no longer functional because of mechanical failure. The caretaker told Human Rights Watch:
The MP has a few trusted followers in this area and he gives the tubewells to them. I didn’t get mine from the MP. The tubewell I received was allocated by the upazila chairman to someone else but that person couldn’t pay the extra costs, so the upazila chairman gave it to me. I work with the government and so I get some advantages.[104]
Human Rights Watch spoke to another caretaker of a government deep tubewell. The tubewell, which he believed was over 200 meters deep, was located in a small tin shed inside the fenced compound of the man’s house. The man considered himself the owner rather than the caretaker of the tubewell and explained:

Six people from my household drink from this well. We don’t let others drink from it. My father-in-law is a friend of the upazila chairman. They are in the same political party, so they have a political friendship. We paid 30,000 taka (approximately US$ 390) to the upazila chairman.[105]
In the same village, Human Rights Watch located a government tubewell installed inside a new private house under construction.
The effects of diversion of government water points across the country is difficult to estimate. However, one recent study of tubewells in one upazila (sub-district) (Araihazar Upazila, consisting of 290 villages in an area 20 kilometers east of Dhaka) gives a sense of the extent of the problem at an upazila level. The study found:

The clustering of deep wells and their frequent installation in areas where access is limited to the household of the land owner may indicate elite capture of a public good ostensibly intended to benefit the entire population.[106]
The study undertook a hypothetical redistribution of deep tubewells according to an evenly spaced grid. Redistributing the deep wells in this way would have improved the number of shallow unsafe wells “covered” by safe deep wells (i.e. within 100 meters) from approximately 6,000 to approximately 16,000. The authors conclude that “a more equitable distribution of the same number of deep wells would have brought almost three times as many exposed households within walking distance of a low-arsenic source.”[107]
Negligible Health Response
Although avoiding arsenic contaminated water is essential, and there is no known cure for chronic arsenic poisoning, the use of vitamins and anti-oxidants can accelerate the natural excretion of arsenic from the body. Symptomatic treatments are also important to help reduce the suffering of patients. Accurate diagnosis of disease and its cause can also help relieve the trauma of illness.
Bangladesh has a nationwide system of village-level health clinics that could provide such basic treatment. The government could also strengthen the capacity of upazila (sub-district) health centers and district hospitals to diagnose, treat, and care for the vast majority of individuals exposed to arsenic who will suffer chronic diseases without easily visible symptoms like skin lesions.
Yet Bangladesh currently does little or nothing for those who suffer arsenic-related health problems. In none of the villages visited by Human Rights Watch were village-level health clinics distributing vitamins, anti-oxidants, or symptomatic treatments such as ointments.
Some villagers told Human Rights Watch that they had previously received these items from government health clinics, usually upazila (sub-district) level health complexes in nearby towns. But supplies had since stopped, so these individuals no longer bothered to make the trip.
The problem of inadequate health care services for people suffering arsenic-related health conditions has been reported by previous studies.[108] A survey of staff from over 50 upazila (sub-district) health complexes across the country reported that insufficient supplies of medications was widespread, there was generally poor case management of patients, and health complexes had limited capacity to carry out water testing.[109]
At the national level, the DGHS lists the number of “arsenic patients” each year in the chapter on non-communicable diseases in its annual Health Bulletin.[110] These patients are identified by their skin lesions. The DGHS does not count the vast majority of exposed individuals (even with high levels of chronic exposure) who will not develop skin lesions but will develop diseases such as cancers, cardiovascular disease, and lung disease.
In terms of national health policy, Bangladesh’s has no plan to manage the health impacts from arsenic exposure. The country’s strategic plan for surveillance and prevention of non-communicable diseases for 2007-2010 made no mention of arsenic. The following plan (2011-2015) mentions arsenic once in an annex listing national policies, noting only that a “national plan [is] to be developed.”[111]
Lack of Village-Level Efforts
Nayok lives in Balia and is suspected of having arsenic-related health conditions. She is in her late 20s and lives with her husband and three children. She has calloused palms and white and dark spots on her neck and upper chest. She told Human Rights Watch she had never seen a government doctor or health worker for arsenic-related issues. Her house is located a few hundred meters from a village health clinic in Balia:
It’s just two minutes’ walk away but I’ve never been there. My neighbors have the same problems, but I haven’t seen anyone from our neighborhood go to that community clinic for arsenic issues. They don’t provide help with arsenic problems, not even with multivitamins.[112]
Astha is a woman about 40 years old. She lives in Ruppur and looks after her two children while her husband lives and works in Dhaka. She has spots on the back of her hands and the soles of her feet. For the last couple of years, she has had a chronic cough and complains of a burning sensation on her skin. She told Human Rights Watch:
I’ve never been to a hospital, I’ve never seen a doctor. I take no medication. No one from the government has ever told me anything about arsenic or that I suffer some effects of arsenic poisoning.[113]
Like Astha, Choritro lives in Ruppur and is suspected of having arsenic-related health conditions. He is about 50 years old and runs a small shop. He has dark spots over his chest and a heavy, persistent cough:
I can’t remember any government health workers coming to this village. We have a community health clinic in this village which distributes things like painkillers and some medicines for pregnant women but they have never given any help for people with arsenic poisoning.[114]
Khobor is the man in his mid-30s introduced in the Summary section of this report, who has recently developed similar marks on his body and feet. He also told Human Rights Watch, “I’ve never been to a government hospital or health clinic.”[115]
In some locations, some basic care for arsenic-related illnesses was previously provided in health clinics in nearby towns but had since ceased.
Shuta is a woman in her mid-50s living in Iruain. Shuta explained that the government health clinic in Iruain provides no assistance for people suffering arsenic-related health problems. For a while she attended the government’s upazila (sub-district) health complex in Laksam, about four kilometers away from Iruain.
In Laksam health complex they told me I have arsenic poisoning. They registered me as a patient and they gave me medicine and ointment for my hands. The ointment helped with the pain in my hands. This was about four years ago and they gave me these medicines every month, for about two years. Then they stopped. I went once and they said there were no more vitamins. Now I’m not getting any treatment.[116]
Like Shuta, Meru lives in Iruain village. He is in his early 30s. When Human Rights Watch talked to him, he had spots on his body, thickened skin on the palms of his hands, and large, cracked callouses on his feet. Meru had previously worked as a health officer in an arsenic-related project run by an NGO. He told Human Rights Watch:
The government gave medicines just once, for three months, out of Laksam health complex. But when I went back they said there was none. They have nothing for people with health problems because of arsenic in the local clinic. I don’t know why, because some arsenic medicines are very simple.
Meru’s previous employment had given him a sense of the lack of government registration of people suspected of having arsenic-related health conditions in Iruain village. He added:
I think there are many people with arsenic-related health conditions, maybe as many as a few thousand, in Iruain village. No one knows because they don’t count them. Maybe a few hundred are registered as patients with the government. I know hundreds of patients who are not registered with the government.[117]
Nouka is around 60 years old. She lives in Balia with her husband, son, and three daughters. She has black spots on her shoulders, arms, and palms and the back of her hands. She had infected skin lesions on one hand and one foot. She described general pain all over her body, poor vision, and nausea. Nouka told Human Rights Watch “I’m not registered with the government as an arsenic patient: I don’t think anyone from this village is registered.”
She previously received sporadic health services from the community health clinic in Ulania (about three kilometers away):
I show them the back of my hands and asked ‘Do you have any cream or ointment for my hands?’ They say, ‘No.’ I also ask about multivitamin tablets: the clinic has given me multivitamins two or three times over the last few years. Each time is 10 tablets that last 10 days. They usually say they have none in stock. When it comes to arsenic problems they usually say, ‘We have nothing for your illnesses.’[118]
Agrahayan is a man in his mid-50s living in Ruppur village. He has white and black spots across his chest. He also complains of a chronic cough. He told Human Rights Watch he used to receive health care from the government’s upazila (sub-district) health complex in Ishwardi, about eight kilometers from his house:
People used to come from Ishwardi health complex, check on us, and tell us to go to the clinic on a specific day to collect our little bottles of multivitamins. But they don’t come any more— they haven’t come for the last five years or so.
Agrahayan added:
There’s a government health clinic in the next neighborhood of Ruppur [to mine]. I’ve never been there for any medicines because they don’t have these sorts of tablets. They do family planning, immunizations, birth assistance, things like this. But they have no medicines for arsenic.[119]
Khaddro is a farmer in his late 30s. Like Agrahayan, he lives in Ruppur village. He has had patchy skin all over his body for the last 20 years. He showed Human Rights Watch swollen hands and spots on his hands and feet. He recalls one recent occasion when the Ishwardi health complex distributed multivitamins for people suspected of having arsenic-related health conditions:
About two years ago they gave multivitamins out of the upazila (sub-district) health complex but when they did this they were all one month from expiry. They gave me so many bottles that my backpack couldn’t hold them. When I asked, ‘What am I supposed to do with all these tablets?’ they said, ‘Just give them to others.’ They expired a month later so I threw most of them away. If you went to the health complex now they would give you a prescription saying you need treatment, but no medicines.
Khaddro added, “It’s easy to undercount [people suspected of having arsenic-related health conditions in Ruppur village]. The government doesn’t do any field work. They don’t come to see.”[120]
Hospitals as a Last Resort
There is a pressing need for district hospitals to develop and implement improved surveillance, treatment, and care programs for chronic diseases known to be caused by arsenic, including cancers, cardiovascular disease, and lung disease.
Many people suffering arsenic-related health conditions see no point in attending government hospitals. Shetu is a woman about 50 years old who lives in Bilmamudpur. Her husband died from cancer some 15 years ago, which she put down to arsenic exposure because “he had black spots all over his skin.”
She showed Human Rights Watch the thickened skin on her hands and spotty skin on her forearms. She complained of itchy skin, particularly when it is hot, and pain in her joints. The local health clinic in the village provides no arsenic-related services and she has never been to the upazila (sub-district) health complex nor the district hospital.
Shetu explained to Human Rights Watch why she had never sought care for her arsenic-related conditions from a government hospital:
We poor people don’t go to government hospitals. What is the point? It costs for transport to go there, then they take money to do tests. Then, at the end of the day, they give you paracetamol and tell you to go to the pharmacy for other medicines.[121]
In a few cases, people suspected of having arsenic-related health conditions had sought care from government hospitals. Balu is a man in his 40s who works as a farmer in Bilmamudpur. When he spoke to Human Rights Watch he had dark spots on his chest and swollen feet. He and his family get their drinking water from three shallow wells close to his house, all of which had been painted red approximately three years ago after being tested by an NGO.
When Balu went to a nearby government hospital—Faridpur Medical College hospital—he was told he was suffering a skin allergy and given a prescription for vitamins that he had to purchase from a local pharmacy:
I don’t really know if I have these problems because of arsenic. They told me it was a skin allergy that’s not related to arsenic. They did no further tests. They spent about 10 minutes with me.[122]
In some cases, villagers undergo extraordinary efforts and expenses to receive better medical care. Neel, in his early 30s, also lives in Bilmamudpur. He has thickened skin and spots on his hands and white spots on his forearms arms and calves. He had never been to a government hospital. However, in 2006 his family had sought care for his mother (who had similar but more severe symptoms) in India:
In 2006 we took her to a government doctor [in Faridpur] working in a private practice. He said there was no way to save her, that there was no treatment left for her in this country. So we decided to take her to India. We went to Benapole on the border neat Jessore, then took a taxi to Kolkata. She saw a skin specialist, a general practitioner, and an eye specialist. It cost us about 70,000 taka (approximately US$4,900) in total.[123]
When people suspected of having arsenic-related health conditions do attend government hospitals in Bangladesh, it is often too late. Groho, in his mid-50s, works as a farmer in Balia. He has spots on his hands, chest, and forearms. He complains of a frequent feeling of itchiness across his torso. He lives in a household of eight people, and worries about the health of his wife and his youngest daughter, both of whom have similar symptoms to his. He told Human Rights Watch: “I’ve never seen a government doctor in this village in my entire life. They just don’t come here.”
The day that Groho talked to Human Rights Watch, his cousin had died. He was visibly upset and spoke in a low voice.
My cousin had the same type of spots on his arms and chest as I have, only worse. He always complained that his arms and legs felt like they were burning. He was a diabetic for the last couple of years. He went to see government doctors in Dhaka five months ago: they told him to go somewhere else because they didn’t have facilities to treat him. So he went to a private clinic, but it did him no good.[124]
III.Bangladesh’s Legal Obligations
Right to Water
In 2013, Bangladesh adopted a Water Act that declared water for drinking, sanitation, and hygiene as “the highest priority right”.[125] At the international level, Bangladesh has recognized the human right to safe drinking water and sanitation on several occasions. Bangladesh voted in favor of General Assembly resolution 64/292 of July 2010 which “Recognizes the right to safe and clean drinking water and sanitation as a human right that is essential for the full enjoyment of life and all human rights.”[126]
Bangladesh was a member of the Human Rights Council when it adopted without a vote various resolutions affirming that the human right to safe drinking water and sanitation is derived from the right to an adequate standard of living.[127] The right to an adequate standard of living is enshrined in human rights instruments ratified by Bangladesh such as the International Covenant on Economic, Social and Cultural Rights (ICESCR), the Convention on the Rights of the Child (CRC), and the Convention on the Rights of Persons with Disabilities (CRPD).
The Committee on Economic, Social and Cultural Rights (CESCR), in the General Comment 15 on the Right to Water, has noted that a core content of the right to water is that water required for personal or domestic use must be safe. This means it must be free from microbes and parasites, chemical substances, and radiological hazards that constitute a threat to a person’s health.[128]
The committee also stated that a “violation of the obligation to fulfill” the right to water can occur when there is “insufficient expenditure or misallocation of public resources which results in the non-enjoyment of the right to health by individuals or groups.”[129]
|
The DPHE, within the Ministry of Local Government, Rural Development, and Cooperatives, is the lead government agency responsible for water and sanitation services in all parts of the country (except for urban areas, which are covered by water supply and sewerage authorities). Responsibilities for water supply are also distributed to various levels of local government. The lowest level of local government in rural areas of Bangladesh is the union parishad (council). The Union Parishad Act (2009) establishes that union parishads (councils) are responsible for the management and maintenance of water points, preventing the contamination of water points used for drinking water, and prohibiting the use of water points suspected to be dangerous to public health.[130] In areas governed by a municipality (pourashava), the municipal government is responsible for providing or ensuring “sufficient wholesome water for public and private purposes”.[131] The law also provides that the municipality control, regulate, and inspect all private water-supplies.[132] At the upazila (sub-district) level, the upazila administration also has a role coordinating “proper measures for supplying drinking water.”[133] |
Right to Health
The right to the highest attainable standard of health is found in article 25 of the Universal Declaration of Human Rights and in international treaties binding upon Bangladesh, including the International Covenant on Economic Social and Cultural Rights (ICESCR) and the Convention on the Rights of the Child (CRC).[134]
The CESCR, in the General Comment 14 on the Right to Health, has interpreted the ICESCR to include:
[T]he requirement to ensure an adequate supply of safe and potable water and basic sanitation [and] the prevention and reduction of the population’s exposure to harmful substances such as radiation and harmful chemicals or other detrimental environmental conditions that directly or indirectly impact upon human health.[135]
The right to health encompasses the right to healthy natural environments.[136] This right involves the obligation to “prevent threats to health from unsafe and toxic water conditions.”[137]
The CESCR has stated that a “violation of the obligation to fulfill” regarding the right to health can occur when there is “insufficient expenditure or misallocation of public resources which results in the non-enjoyment of the right to health by individuals or groups.”[138]
The Bangladeshi Constitution orders the government to improve public health and guarantees all citizens the right to life.[139]
Right to Information
The CESCR, in the General Comment 15 on the Right to Water, has noted that a core obligation of states under the right to water is that individuals have the right to seek, receive and impart information concerning water issues.[140] The CESCR has also noted that “[i]ndividuals and groups should be given full and equal access to information concerning water, water services and the environment, held by public authorities or third parties.”[141]
The CESCR, in the General Comment 12 on the Right to Health, has stated that a “core obligation” of states under the right to the highest attainable standard of health is:
To provide education and access to information concerning the main health problems in the community, including methods of preventing and controlling them.[142]
Bangladeshi law protects the right of the public to access existing environmental information.[143] Internationally, it is acknowledged that freedom of information is critical to environmental protection and realizing the right to health. As Fatma Zohra Ksentini, special rapporteur to the sub-commission on prevention of discrimination and protection of minorities, noted as early as 1994:
The Special Rapporteur also considers that the right to information includes the right to be informed, even without a specific request, of any matter having a negative or potentially negative impact on the environment. It is clear to the Special Rapporteur that the right to information imposes a duty on Governments. It is also clear to the Special Rapporteur that the right to information imposes a duty on Governments to collect and disseminate information and to provide due notice of significant environmental hazards.[144]
Bangladesh’s Water Act (2013) establishes that intentionally providing false or distorted information is liable to up to one year in prison and/or a fine of up to 3,000 taka (approximately US$40).[145]
Acknowledgements
This report was researched and written by Richard Pearshouse, senior researcher for the Health and Human Rights Division of Human Rights Watch. Brian Root, quantitative analyst at Human Rights Watch, analyzed the data and created the graphs in the “Government Water Points at the National Level” section. The report was edited by Joe Amon, director of the Health and Human Rights Division; Clive Baldwin, senior legal advisor; and Danielle Haas, senior editor in the Program Office. Amanda Klasing, senior researcher for the Women’s Rights Division; Michael GarciaBochenek,senior counsel to the Children’s Rights Division; and Tejshree Thapa, senior researcher for the Asia Division, all provided input and comments on portions of the report.
Marco Bassano and Michele Johnsen provided significant research support. Meg Mszyco provided editing and production assistance. Olivia Hunter, publications specialist; Veronica Matushaj, creative manager; Jiahui Chen, production associate; and Fitzroy Hepkins, administrative manager, provided production assistance. Grace Choi, Josh Lyons, and Brian Root produced the map. Atish Saha and Richard Pearshouse took the photos.
Human Rights Watch is deeply grateful to those people in Bangladesh who facilitated this research and to those people who reviewed draft sections of this report for its technical accuracy.
Above all, Human Rights Watch would like to acknowledge the many individuals living in rural areas of Bangladesh who shared their knowledge and experiences with us. Without their testimony this report would not be possible.


