
Summary
In January 2019, hundreds of thousands of Venezuelans took to the streets, following an appeal by National Assembly president Juan Guaidó, who asked the Venezuelan people to mobilize in support of restoring constitutional order in the country. During a massive protest on January 23, Guaidó claimed that he was taking power as interim president of Venezuela and said he would call for free and fair elections. More than 50 governments have since recognized him as Venezuela’s interim president, but Nicolás Maduro continues to exercise firm control over all Venezuelan institutions, except for the opposition-controlled National Assembly.
While this political power struggle unfolds, one of the major underlying concerns for the Venezuelan people is the dramatic humanitarian crisis they are facing. In one of his first public speeches since becoming the National Assembly president on January 5, Guaidó said Venezuela was facing a humanitarian emergency and asked the international community for aid to address it.
It is impossible to know yet the full extent of the health and food crises in Venezuela. This is largely because the Venezuelan authorities have failed to publish health and nutrition data and retaliated against those who did.

To assess the current state of the humanitarian crisis in Venezuela, and the impact of the crisis on the human rights of Venezuela’s population and on neighboring countries, Human Rights Watch partnered with the Center for Humanitarian Health and the Center for Public Health and Human Rights at the Johns Hopkins Bloomberg School of Public Health. This report is based on interviews with more than 150 health care professionals, Venezuelans seeking or in need of medical care who recently arrived in Colombia and Brazil, representatives from international and nongovernmental humanitarian organizations, United Nations (UN) officials, and Brazilian and Colombian government officials. In addition, researchers analyzed data on the situation inside Venezuela from official sources, hospitals, international and national organizations, and civil society organizations.
We found a health system in utter collapse with increased levels of maternal and infant mortality; the spread of vaccine-preventable diseases, such as measles and diphtheria; and increases in numbers of infectious diseases such as malaria and tuberculosis (TB). Although the government stopped publishing official data on nutrition in 2007, research by Venezuelan organizations and universities documents high levels of food insecurity and child malnutrition, and available data shows high hospital admissions of malnourished children.
A massive exodus of Venezuelans—more than 3.4 million in recent years, according to the UN—is straining health systems in receiving countries.
Acknowledging the problem and asking for help is a crucial first step, but the UN’s leadership is essential to the success of any large-scale humanitarian assistance plan in Venezuela. The combination of medicine shortages and food shortages, together with the spread of diseases across Venezuela’s borders, amounts to a complex humanitarian emergency that requires a full-fledged response by UN humanitarian actors.[1]
International humanitarian aid to Venezuela increased in 2018, after a shift in the government’s discourse from entirely denying the humanitarian crisis to recognizing an economic one. The government, however, blamed the shortages on US imposed sanctions, even though the humanitarian crisis preceded sanctions on the oil sector that could potentially have an impact on the importation of food and medicines. Humanitarian actors from international and non-governmental organizations have consistently reported that aid to Venezuela is not enough to cover the population’s urgent needs.
To protect the rights to health and food of the Venezuelan people, UN Secretary-General António Guterres should lead efforts to develop a comprehensive humanitarian response plan for the situation both inside and outside of the country. The plan should respect the principles of humanity, neutrality, independence, and impartiality in the provision of assistance. It should also include an independent assessment of the extent of the crisis, prioritization of the crisis by the UN Office of Coordination of Humanitarian Affairs (OCHA), and ensure access to import necessary food, medicines, and medical supplies. Furthermore, a concerted and comprehensive plan to assist displaced Venezuelans outside of the country, which recognizes that such displacement tends to be protracted, needs to be created and implemented.
Health Crisis
Venezuela’s health system has been in decline since 2012, with conditions worsening drastically since 2017. A nation-wide blackout in March that lasted more than a day, and intermittent blackouts since then, have further undermined the ability of public hospitals to adequately respond to the medical needs of Venezuelans.
Venezuela is now routinely experiencing outbreaks of vaccine-preventable diseases that had once been eliminated in the country. These outbreaks suggest a serious decline in vaccination coverage. The Pan American Health Organization (PAHO) reports:
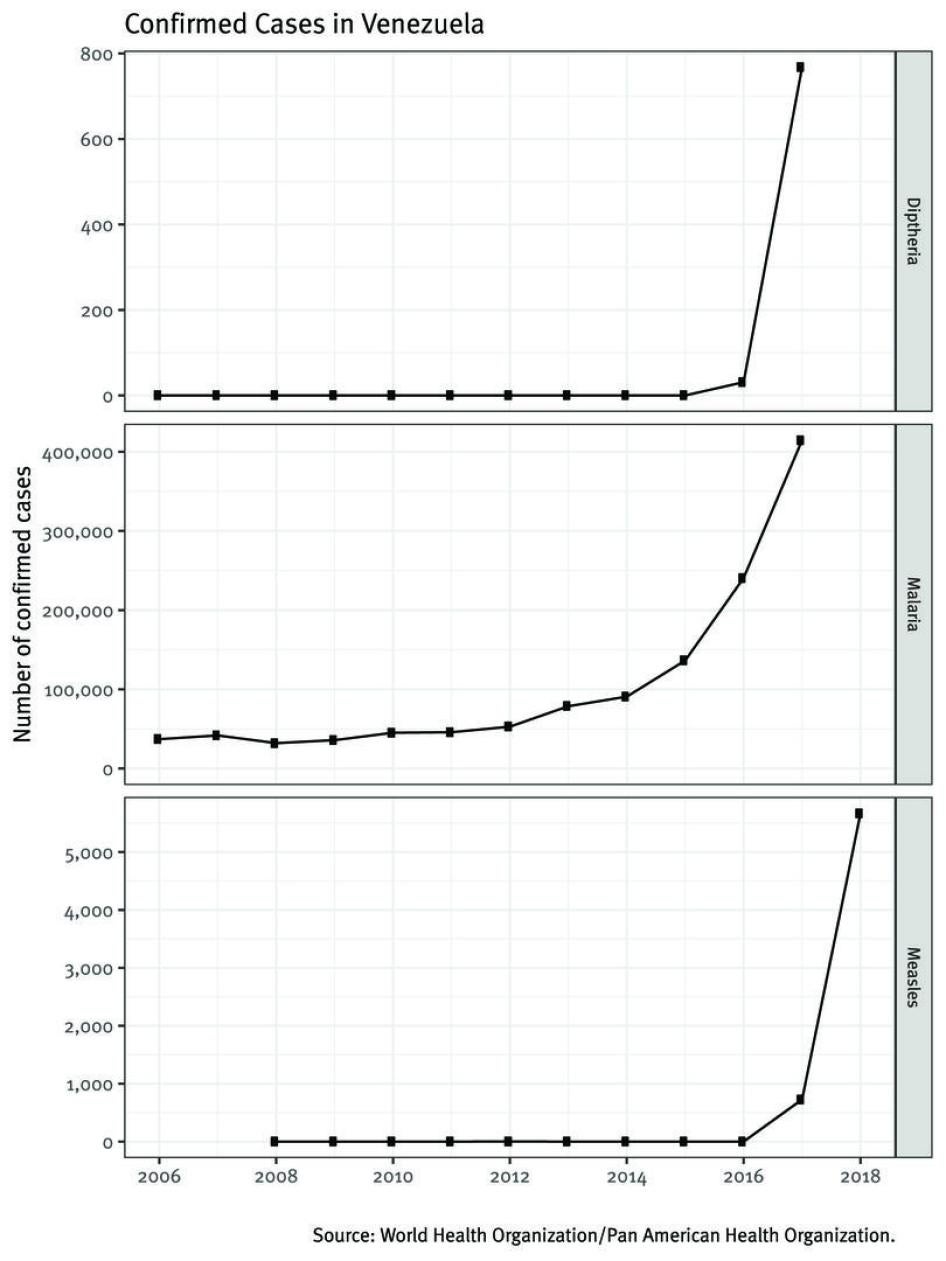
- Between 2008 and 2015, only a single case of measles was recorded (in 2012). Since June 2017, more than 9,300 cases of measles have been reported, of which more than 6,200 have been confirmed.
- Venezuela did not experience a single case of diphtheria between 2006 and 2015, but more than 2,500 suspected cases have been reported since July 2016, including more than 1,500 confirmed cases.
The World Health Organization (WHO) reports that confirmed malaria cases in Venezuela have consistently increased in recent years—from fewer than 36,000 in 2009 to more than 414,000 in 2017. An official document co-authored by the Venezuelan Health Ministry shows that malaria is now endemic in Venezuela. Health experts attribute this to reductions in mosquito-control activities, shortages in medication to treat the disease, and illegal mining activities that promote mosquito breeding by creating pools of water.
The number of reported TB cases in Venezuela increased from 6,000 in 2014 to 7,800 in 2016, and preliminary reports indicate more than 13,000 cases in 2017. The TB incidence rate has increased constantly since 2014, reaching 42 per 100,000 in 2017—the highest seen in Venezuela in 40 years.
It is difficult to estimate recent HIV trends in Venezuela: HIV testing has been greatly reduced because of a lack of test kits, and no surveillance data on new HIV diagnoses has been published since 2016. Similarly, statistics on HIV-related mortality are not available after 2015. However, according to the last data available, both new HIV infections and HIV-related deaths have been sharply increasing.
Venezuela is the only country in the world where large numbers of individuals living with HIV have been forced to discontinue their treatment as a result of the lack of availability of antiretroviral (ARV) medicines. A 2018 PAHO report estimated that nearly nine of ten Venezuelans living with HIV registered by the government (69,308 of 79,467 people, or 87 percent) were not receiving ARV treatment, though the actual number of people who need ARVs is unknown.
The latest official statistics available from the Venezuelan Ministry of Health indicate that in 2016, maternal mortality rose 65 percent and infant mortality rose 30 percent in just one year. While infant mortality has risen throughout the region, Venezuela is the only country in South America that has risen back to infant mortality rate levels of the 1990s. The health minister who made these statistics public in early 2017 was fired a few days later, and the Ministry of Health has not released any epidemiological data since then.
Nutrition Crisis
Hunger, malnutrition, and severe shortages of food are widespread. Many of the dozens of Venezuelans whom the Human Rights Watch and Johns Hopkins team interviewed at the border said they had lost weight and were eating one or two meals a day back home. For some, a meal consisted solely of yuca or tinned sardines.
The Venezuelan government has not published nationwide nutrition data since 2007, but available evidence suggests malnutrition is high:
- In 2018, the UN’s Food and Agriculture Organization (FAO) indicated that between 2015 and 2017, 11.7 percent of Venezuela’s population—3.7 million people—was undernourished, up from less than 5 percent between 2008 and 2013.
- In February 2019, a spokesperson for WHO confirmed that “Venezuela had indeed experienced an increase in the number of undernourished persons,” based on a joint report by FAO, PAHO, UN Children’s Emergency Fund (UNICEF), and the World Food Programme (WFP).
- A nationally representative survey by three prestigious universities in Venezuela concluded that 80 percent of Venezuelan households are food insecure, meaning they do not have a reliable source of food, and that nearly two-thirds of people surveyed had lost weight (on average 11 kilograms or nearly 25 pounds) in 2017.
- Cáritas Venezuela, a Catholic humanitarian organization that monitors nutrition and provides nutritional aid to children in low-income communities in Caracas and several states, reported that moderate acute malnutrition (MAM) and severe acute malnutrition (SAM) among children under age 5 increased from 10 percent in February 2017 to 17 percent in March 2018—a level indicative of a crisis, based on WHO standards. Subsequent reports found that the overall rate in those states had decreased to 13.5 percent in July and 9.6 percent in September, but rates increased in the same period from 11.6 to 13.4 percent in Miranda state, and from 6 to 11.8 percent in Sucre state.
- A September 2018 Cáritas Venezuela survey found that 21 percent of pregnant women in low-income communities had moderate or severe acute malnutrition.
- Several hospitals across the country are reporting increases in the number of children admitted with moderate or severe acute malnutrition, as well as deaths of children with acute malnutrition, according to information provided by Venezuelan health professionals to Human Rights Watch and Johns Hopkins University.
Impact Across Venezuela’s Borders
The massive exodus of Venezuelans—many of whom fled their country in search of medicines, medical supplies, health providers, and basic health services—is straining services across Venezuela’s borders. Available data from Colombian and Brazilian authorities on Venezuelan patients gives a glimpse of the deteriorating conditions that Venezuelan authorities are failing to adequately report.[2]
In Colombia—the country that has received the largest influx of Venezuelans—the North Santander border area has seen a sharp rise in the number of reported cases of Venezuelans seeking medical care, from 182 in 2015 to 5,094 in 2018.[3] Venezuelans have sought care for acute, chronic, and infectious diseases, as well as access to reproductive health and prenatal and maternal care.
According to a 2018 report by the Colombian government, more than 8,000 pregnant Venezuelan women who had entered Colombia were expected to give birth in the country; the majority of this population did not have access to any type of prenatal care in Venezuela. Declines in maternal and infant health, health professionals said, reflected the lack of availability of care in Venezuela. Forty-five Venezuelan women experienced serious illness tied to pregnancy or childbirth, and seven died in 2018 on the Colombian side of the border. Low birth weight and perinatal and neonatal mortality among Venezuelan infants have risen drastically in Colombia with 211 newborn deaths in 2018.
Colombian health officials have had to address increasing cases of SAM among Venezuelan children under age 5 as well, with the number of cases rising from zero in 2015 to two in 2016, 13 in 2017, and 360 in 2018. Health officials have also seen the first deaths of Venezuelan patients from acute malnutrition ever reported in 2017, with three deaths. In 2018, 11 Venezuelans died from acute malnutrition.
Brazil experienced its first cases of measles in early 2018, after no confirmed cases since 2015. More than 10,000 cases have since been confirmed, as of January 2019. The strain of the measles virus (D8) in Brazil is identical to the strain causing the outbreak in Venezuela. The majority (61 percent) of cases in Roraima state, the main Brazilian port of entry from Venezuela, have occurred among Venezuelans.
Malaria has also surged in Roraima, where the number of cases among Venezuelans increased from 1260 in 2015 to 2470 in 2016 and 4402 in 2018. They have continued to rise since. Physicians told us that Venezuelans were more likely to arrive at the hospital very sick, and their management was often complicated by malnutrition.
Brazilian health officials are also seeing increasing cases of TB and HIV. Between January and December of 2018, 60 Venezuelans with TB had been identified by the health authorities in Roraima. This was more than the total number of TB cases among Venezuelans in the preceding five years (2013 to 2017), when a total of 32 cases were reported among Venezuelans in Roraima.
At the Specialty Clinic Colonel Mota, which is the primary source of outpatient HIV care in Roraima, 171 Venezuelan patients were receiving ARV therapy for HIV in August 2018. Among them, almost 70 percent (117) arrived at the clinic seeking care in 2018 alone. Physicians at the clinic reported to the Human Rights Watch and Johns Hopkins University team that Venezuelans living with HIV presented for care often malnourished and already very sick with life-threatening opportunistic infections due to the lack of available ARVs in Venezuela.
The Maduro Government’s Responsibility
Despite overwhelming evidence that Venezuela is facing a humanitarian crisis, the Maduro government continues to publicly minimize it and to suppress information about it, and has done far too little to alleviate it.
Venezuelan authorities under Maduro have concealed the crisis by ending the once-regular publication of official health information. They have harassed and retaliated against those who collect data or speak out about food and medicine shortages. These actions, together with the government’s failure to acknowledge the full scope of the problem, have rendered a comprehensive diagnosis of the crisis impossible. Such a diagnosis is critical to creating an effective humanitarian response.
The Venezuelan government’s failure to report public health information, its suppression of those speaking out about health conditions within the country, all while the country’s health facilities continue to deteriorate, represent a violation of Venezuela’s obligations to respect, protect, and fulfill the right to health guaranteed under both the Venezuelan Constitution and the International Covenant on Economic, Social and Cultural Rights (ICESCR). The ICESCR, which Venezuela has ratified, guarantees everyone the right to “the enjoyment of the highest attainable standard of physical and mental health,” as well as the right to an adequate “standard of living” that includes “adequate food.”
While more international aid started to enter the country in 2018, interviews with humanitarian workers from international and nongovernmental organizations operating in Venezuela clearly state that the aid is not sufficient to meet the population’s urgent needs. At the same time, the government has not only failed to acknowledge the extent of the country’s needs and request the scale of assistance the crisis demands, but has in many cases imposed barriers on the activities of international humanitarian organizations.
The Maduro government is largely to blame for the lack of a coordinated international response to Venezuela’s crisis. By failing to acknowledge the full scope of the crisis and invite key UN agencies to independently assess the situation and coordinate an effective response to it, Venezuelan authorities are contributing to the suffering of the Venezuelan people. Instead of threatening and harassing concerned Venezuelans who call attention to the country’s problems, they should make every effort to collect and publicize data about the health and food security crises. While Venezuelan authorities are within their rights to reject particular offers of assistance, doing so only heightens their responsibility to work towards alternatives that can fully address the urgency of the country’s needs. Efforts undertaken by Venezuelan authorities during the presidency of Nicolás Maduro have failed to do so.
Recommendations
The UN should prioritize addressing Venezuela’s quickly deteriorating humanitarian situation. The UN’s senior leadership and all relevant UN bodies should engage in proactive diplomacy to press Venezuelan authorities to allow UN agencies to lead and implement a large-scale humanitarian response that will ensure the Venezuelan population receives necessary humanitarian assistance to address its urgent needs.
The UN Secretary-General António Guterres should:
- Publicly acknowledge that Venezuela is facing a complex humanitarian crisis and prioritize the adoption by UN bodies and UN agencies involved in humanitarian assistance of measures to address it, including those recommended in this report;
- Make clear to Venezuela’s leadership that it is responsible for ensuring that the UN can implement a humanitarian response commensurate with the gravity of the crisis;
- Designate the UN Emergency Relief Coordinator (ERC), who is also the head of OCHA and is responsible for coordinating humanitarian action to respond to emergencies, to negotiate with competent Venezuelan authorities to:
- Grant UN staff and humanitarian non-government organizations (NGOs) full access to official disease, epidemiological, food security, and nutrition data so they can carry out an independent and comprehensive humanitarian needs assessment of the full scope of the crisis, as well as permission to conduct their own independent assessments;
- Ensure the implementation of a UN-led large scale humanitarian response in Venezuela;
- Ensure the UN Country Team has the express mandate to deal with the serious humanitarian crisis that Venezuela is facing and that it is fully mobilized and equipped to do so;
- Ensure that the UN humanitarian response has the necessary staffing and resources on the ground to address the crisis;
- Eliminate obstacles to implementing a large-scale humanitarian operation, including legal permits for humanitarian staff to stay in the country and for organizations to import food, medicines, and medical supplies;
- Advocate for OCHA, UNICEF, WFP, UNHCR, WHO, and other UN and NGOs to scale up their presence to facilitate coordination and implementation of a large-scale response; and
- Ensure that in keeping with the principles of Human Rights Up Front, all UN staff inside and outside Venezuela ensure that the human rights of the Venezuelan people are given priority when it comes to deciding on how to address the humanitarian crisis.[4]
The Inter-Agency Standing Committee should:
- Implement the process to decide upon a humanitarian System-Wide Scale-Up Activation to address Venezuela’s humanitarian crisis; and
- Ensure its members collaborate in the implementation of the system-wide scale activation in Venezuela.
The UN Security Council should:
- Regularly meet to address Venezuela’s humanitarian crisis and its impact across Venezuela’s borders;
- Request regular reports from the Secretary-General and UN ERC on the humanitarian crisis and the response to it; and
- Request and discuss all reports, resolutions, and other documents from the High Commissioner for Human Rights and the Human Rights Council.
- In her upcoming report on the situation in Venezuela, to be presented before the UN Human Rights Council in July, the UN High Commissioner for Human Rights should:
- Document the violations to the rights to health and food in Venezuela;
- Urge Venezuelan authorities to release disease, epidemiological, food security, and nutrition data that would enable UN humanitarian agencies to conduct a comprehensive needs-based assessment of the humanitarian situation in Venezuela; and
- Recommend that the Human Rights Council create an International Commission of Inquiry that would look not only into abuses committed by Venezuelan authorities during their crackdown on dissent, but also into violations of the rights to health and food.
The UN Human Rights Council should:
- Continue to monitor closely the humanitarian situation in Venezuela and address it during its upcoming sessions; and
- Adopt a resolution to create an International Commission of Inquiry to investigate violations of the rights to health and food, in addition to the crackdown on dissent since 2014, as follow-up to the UN High Commissioner for Human Rights’ upcoming report on Venezuela.
The Executive Director of the World Health Organization (WHO) should:
- Collaborate with the UN in the implementation of large-scale response to address Venezuela’s humanitarian emergency led by the UN; and
- Ensure that Venezuela is fully reporting data in accordance with its obligations under the International Health Regulations (IHR) and agreements with PAHO/WHO and other UN agencies.
Lima Group members, the United States, and European governments should:
- Organize a high-level meeting, inviting representatives from key UN humanitarian organizations and Venezuelan civil society groups working in-country, to develop a humanitarian assistance plan that could increase levels of humanitarian assistance into Venezuela in the short term, including by providing additional support to civil society groups already operating in the country;
- Channel humanitarian assistance into Venezuela through the UN, ensuring it respects the principles of humanity, neutrality, independence, and impartiality in the provision of assistance;
- Continue to impose and enforce targeted sanctions against key Venezuelan officials implicated in human rights violations and ensure that any other sanctions on Venezuela include exceptions that allow for the importation of food, medicine, and medical supplies; and
- Ensure that targeted sanctions against specific Venezuelan individuals involved in human rights abuses are carefully enforced.
Venezuelan authorities should:
- Release all available epidemiological data so OCHA can coordinate an independent, comprehensive assessment of the full scope of the crisis; and
- Grant UN humanitarian agencies and NGOs full access to the country so they can implement a large-scale humanitarian response to address the crisis.
The governments of Colombia and Brazil should:
- Continue to make efforts to ensure Venezuelans in their territories have access to adequate health services, in accordance with the international obligation to protect the right to health of migrants and refugees;
- Continue to monitor surveillance data to identify health priority needs among Venezuelan migrants and refugees, and collaborate with national and local public health authorities, as well as PAHO, to respond to increases in infectious diseases and poor maternal and neonatal outcomes;
- Maintain political will and facilitate access to transit permits, border mobility cards, and/or temporary residency status, as applicable;
- Invest in health services to support dramatic rises in healthcare utilization;
- Continue to promote integration to improve the housing situation and economic opportunities for Venezuelans abroad, and to minimize resentment among local populations in remote and underserved areas at the Venezuelan border; and
- Continue to work with UN humanitarian agencies, other Latin American governments, NGOs and the international community to create, fund, and implement a concerted and comprehensive plan to assist displaced Venezuelans outside of the country, which recognizes that such displacement tends to be protracted.
Methodology
This report is based on 156 interviews with health care professionals, Venezuelans seeking or in need of care for an array of illnesses who had recently arrived in Colombia and Brazil, representatives from international and nongovernmental humanitarian organizations, UN officials, and Brazilian and Colombian government officials. The interviews were conducted primarily during research missions to the Venezuelan border with Colombia (Cúcuta) and with Brazil (Boa Vista and Pacaraima) in July and August 2018. Some of the interviews—including all of the interviews with doctors or other health professionals in various locations in Venezuela—were conducted via telephone, email, or online platform before and after the research trips. We did not conduct in-person research in Venezuela for this report out of security considerations for our staff and the people we would be interviewing.
Human Rights Watch and Johns Hopkins researchers visited seven public hospitals or health centers in Colombia and Brazil. We interviewed 13 health professionals working there, as well as 11 representatives from UN agencies and more than 14 government officials responding to the influx of Venezuelans. We also interviewed 71 Venezuelans who had crossed the border into Colombia or Brazil, including many who were hospitalized at the time of the interview.
Researchers conducted 25 interviews with doctors or nutritionists working in Venezuela, and seven other interviews with an epidemiologist and representatives of medical associations in several states. The interviewees worked in Caracas and 15 states: Anzoátegui, Apure, Barinas, Bolivar, Carabobo, Delta Amacuo, Lara, Mérida, Miranda, Nueva Esparta, Sucre, Táchira, Vargas, Yaracuy, and Zulia. We also interviewed more than a dozen humanitarian workers from international and nongovernmental organizations, including some based in Venezuela.
Interviews were conducted by Human Rights Watch and/or Johns Hopkins University staff in Spanish. Interviewees were informed of how the information gathered would be used, and informed that they could decline the interview or terminate it at any point. In some interviews, we paid reimbursement for transportation. One focus group was carried out in Colombia; the rest were key informant, individual interviews. The names of some sources have been replaced with pseudonyms, and the names of some health care professionals have been withheld for security concerns, as indicated in relevant citations.
Health information is also drawn from reports by WHO, PAHO, and other UN offices, as well as from a thorough analysis of information published by Venezuelan organizations monitoring the situation on the ground, and information provided to us by Venezuelan health professionals working throughout the country. We requested information from UN agencies working on humanitarian crises worldwide on their response in Venezuela, and their responses are included in this publication.
To obtain the official position, in February 2019, we sent a letter to Jorge Arreaza, Venezuela’s foreign minister, requesting information Venezuelan authorities’ views regarding the extent of the crisis and the policies it was implementing to address it. We had not received a response at the time of writing. We reviewed public statements made by high-level Venezuelan authorities, as well as the limited available information produced by the Health Ministry. We also conducted an extensive review of official documents, news accounts in state media outlets, Twitter feeds of government officials, and other official sources to evaluate the Venezuelan authorities’ position and assessment of the humanitarian crisis that Venezuela is facing, as well as their response to the shortages.
This report covers events and data as of March 17, 2019, when it went to print.
Health Crisis
Healthcare Infrastructure
During the initial years of Hugo Chávez’s presidency, progress in the provision of healthcare was “rapid and initial results were promising.”[5] In fact, national health indicators showed an overall improvement in health care during the early 2000s,[6] with increases in life expectancy (from 71.8 to 74.1 years) and declining infant mortality (from 26.7 to 14.6 deaths per 1000 live births) between 1998 and 2013, the period of Chavez’s rule.[7]
But Venezuela’s health system has been in decline since 2012, with conditions worsening drastically since 2017.[8]
The health system has suffered from severe shortages of medicines and health supplies, hospitals without regular access to utilities, health workers emigrating from Venezuela, and a deterioration in emergency services and the capacity to respond to disease outbreaks.[9] A November 2018 nationwide survey by Doctors for Health (Médicos por la Salud), a network of residents working in public hospitals, found that of the 40 hospitals included in the survey from 24 states, 76 percent had reported a lapse in laboratory testing and 70 percent a lapse in radiology services. Thirty-three percent of hospital beds were not available for patients. Many hospitals also reported shortages in basic necessities for the provision of medical care: 67 percent had seen electricity shortages and 70 percent had seen shortages in water. A previous survey in 104 public hospitals and 33 private hospitals nationwide indicated that, as of March 2018, 88 percent of hospitals had reported shortages in medications and 79 percent had shortages in surgical supplies.[10]
People seeking care have been asked to bring in their own medical supplies like syringes and scalpels, as well as food for family members in the hospitals.[11] Due to inflation and shortage of medicines, people have turned to the black market to find needed medications, despite lack of quality guarantees, though many still cannot afford them.[12]
Health care workers have been leaving the country, further exacerbating worsening health system conditions. PAHO reported in July 2018 that 22,000, or about a third, of 66,138 registered physicians in 2014 had already left Venezuela.[13] Many others have left since then as the crisis deepened.[14]
Mortality
The Venezuelan Ministry of Health stopped releasing official data on maternal and child mortality in 2015. In early 2017, the health minister published data for 2016, which indicated that infant deaths rose by 30.1 percent and maternal deaths by 65.8 percent in 2016.[15] As described in the chapter below on the Venezuelan government’s responsibility, the minister was promptly fired, and no statistics have been published since then. In January 2019, The Lancet published an article based on government statistics indicating that infant mortality had increased 40 percent between 2008 and 2016. While infant mortality has risen throughout the region, in Venezuela, the increase has been sharper, with rates returning to levels last seen in the 1990s.[16]
Other data also indicates that maternal and infant mortality is a big concern in Venezuela. UNICEF data shows a near doubling of infant mortality rates over the past five years, increasing by 76 percent, from 14.6 deaths per 1,000 live births in 2012 to 25.7 deaths per 1,000 live births in 2017.[17]
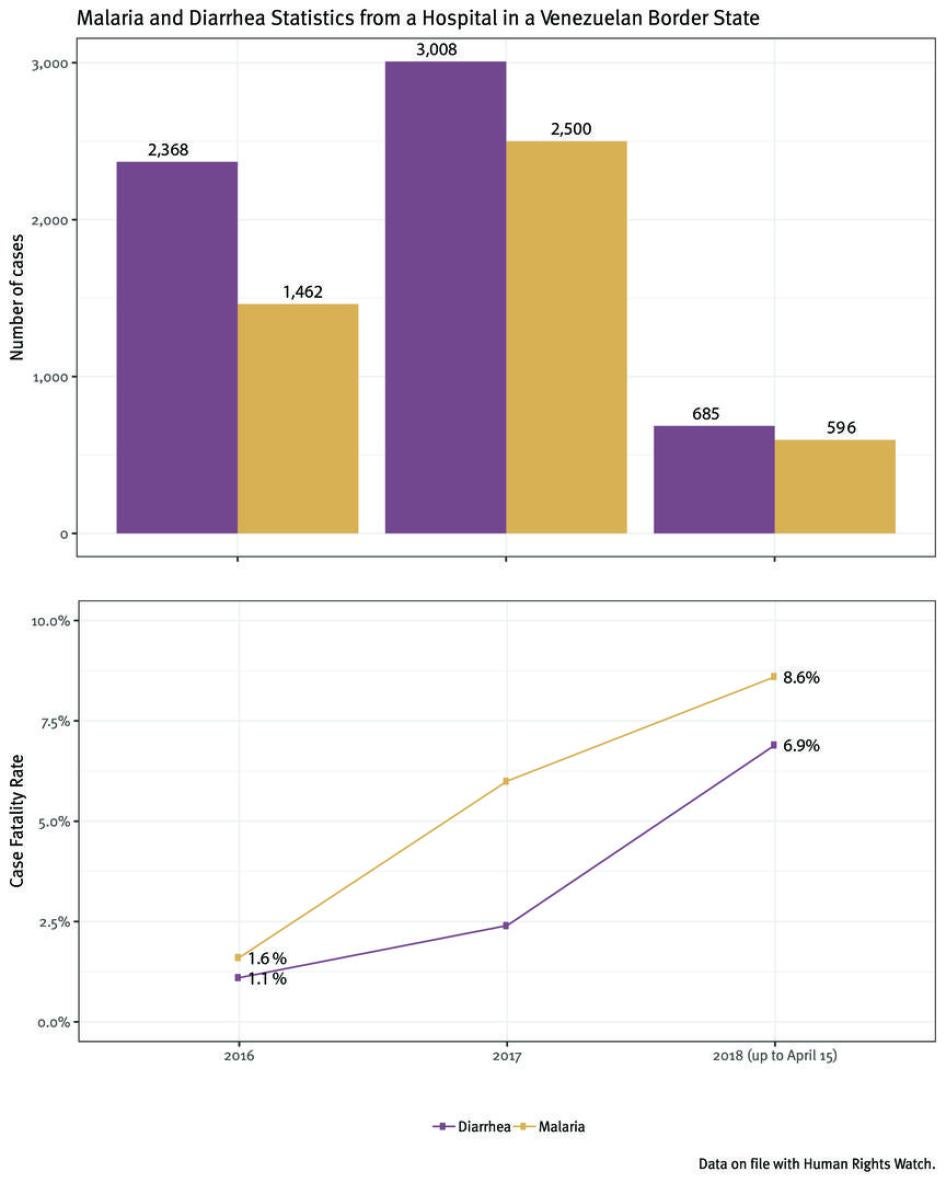
Data from a hospital in a border state in Venezuela shows a quickly deteriorating situation; from 2016 to 2018, neonatal deaths increased by 54 percent at the hospital, and the number of infant deaths overall doubled. The hospital also reported significant increases in admissions of patients with malaria and diarrhea, as well as cases of measles and diphtheria, all of which can cause maternal and infant mortality.[18]
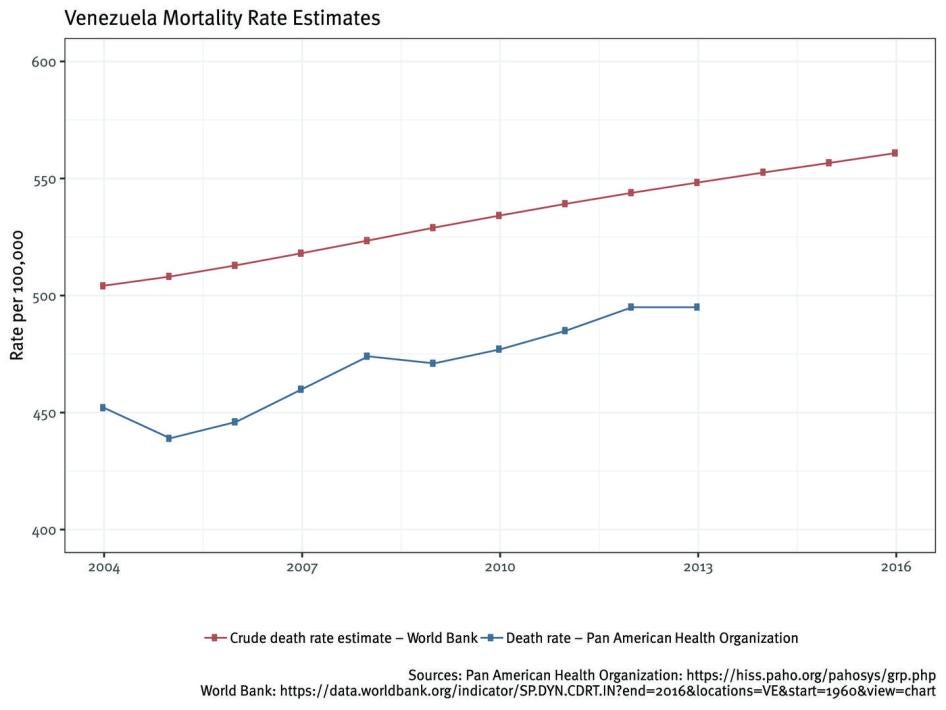
Mortality rates for the Venezuelan population as a whole also appear to be increasing, though data is less recent and pre-dates the crisis. From 2004 to 2014, the number of deaths per 100,000 population annually increased by almost 20 percent, from 450 to 537, which is in contrast to other countries in the region that have reported slow but consistent declines in mortality in recent decades.[19] It is likely that declines in access to quality health services and medicines have exacerbated this trend in the past several years, but recent national mortality statistics are not available.
In addition, there are widespread shortages of basic contraception. Condoms, birth control pills, and intrauterine devices have not been available at public hospitals since 2015. Pharmacy shortages have led to a contraception black market where a month supply of birth control pills, for example, can cost 14 times the minimum monthly income. Venezuela had among the highest teenage pregnancy rates in Latin America prior to the economic collapse, and maternal mortality in 2015 was 40 percent higher than the regional average. According to the director of Venezuela’s largest network of family planning clinics, the number of patients presenting with complications from clandestine abortions has increased, as have the number of women seeking permanent sterilization.[20]
Vaccine-Preventable Diseases
Vaccine-preventable diseases have seen a resurgence in Venezuela. These outbreaks suggest that vaccination coverage in Venezuela is insufficient.
From July 2016 through early January 2019, 2,512 suspected cases of diphtheria (1,559 confirmed cases) appeared in Venezuela, 270 of them fatal. Cases have been seen in several states throughout the country with children under age 15 having the highest incidence rate.[21] By contrast, between 2006 and 2015 not a single case of the disease was reported in Venezuela.[22]
No cases of measles were recorded in Venezuela between 2008 and 2015, except for a single case in 2012.[23] Measles reemerged in June 2017.[24] By February 2019, 9,399 people were suspected to have measles (6,242 confirmed) and 76 had died. In 2018, there were 508 confirmed measles cases among indigenous populations; 62 deaths were reported.[25] Other countries—Brazil, Colombia, Ecuador, Peru, and Argentina—have all seen imported cases of measles from Venezuela. As of November 30, 2018, these countries had 10,140 confirmed cases of measles, a drastic increase from just four cases in these five countries in 2016 and 2017. There were other cases reported in the United States, Canada, Mexico, Chile, Antigua and Barbuda, and Guatemala.[26]
As of March, both diphtheria and measles outbreaks were ongoing in Venezuela, according to PAHO.
Malaria
The number of confirmed malaria cases in Venezuela has consistently increased in recent years—from nearly 36,000 in 2009 to more than 414,000 in 2017, according to WHO.[27]
Venezuela saw a 69 percent increase in malaria from 2016 to 2017, the fastest growth rate in the world.[28] Nine states had reached epidemic levels, with Anzoátegui state seeing a 1,341 percent increase from 2016 to 2017.[29]
In 2017, Venezuela reported its highest number of malaria cases since 1988.[30] Studies have attributed this to severe shortage of medications and vector-control activities, and the propagation of illegal mining activities, where standing water from mining operation
promotes mosquito breeding.[31]
The increase in malaria within Venezuela has threatened progress towards malaria control within the country and region.[32]
HIV
It is difficult to estimate recent HIV trends in Venezuela: HIV testing has been greatly reduced because of a lack of test kits and no surveillance data on new HIV diagnoses has been published since 2016. Similarly, statistics on HIV-related mortality are not available after 2015. However, according to the last data available, both new HIV infections and HIV-related deaths have been sharply increasing, and Venezuela is the only country in the world where large numbers of individuals living with HIV have been forced to discontinue their treatment as a result of the lack of availability of ARV medicines.
In 2016, the Venezuelan Ministry of Health estimated that 120,000 Venezuelans were living with HIV.[33] In 2016, the government reported 6,500 new HIV cases, an increase of 24 percent compared to 2010. However, this number is widely believed to be artificially low because of the shortage of testing kits for HIV.[34] HIV transmission may also be occurring as a result of blood transfusions.
HIV-related morbidity has also increased as a result of delayed diagnosis and poor clinical management of HIV, including lack of access to HIV medicines.[35] A 2018 PAHO report estimated that nearly nine of ten Venezuelans living with HIV registered by the government (69,308 of 79,467 people, or 87 percent) were not receiving ARV treatment, though the actual number of people who need ARVs is unknown.[36] Despite improvements in HIV medicines over the last decade, allowing one dose “triple therapy” regimes with significantly fewer side effects than early HIV drugs first discovered 30 years ago, the death rate among Venezuelans living with HIV was 38 percent higher in 2015 compared to nine years earlier, in 2006.[37] While the UN’s Joint Programme on HIV/AIDS (UNAIDS) has called for “zero AIDS deaths” by 2030, the lack of HIV medicines and laboratory tests to monitor viral load suggest that, without intervention, individuals living with HIV will die at rates far above those in neighboring countries.[38] None of the 339 blood banks in Venezuela had the supplies to test for HIV.[39]
Tuberculosis
The number of Venezuelans with TB increased from 6,000 in 2014 to 7,800 in 2016, and preliminary reports indicate that there were more than 13,000 people with TB in 2017.[40] The 2017 TB incidence rate (42 per 100,000) was the highest in Venezuela in 40 years.[41] In addition, the number of individuals with drug resistant TB, which is very difficult to treat and has a high mortality rate, nearly doubled between 2014 and 2017.[42]
The deteriorating health system and lack of medical supplies has curtailed the ability to test for TB. Physicians have stated that patients are unable to receive treatment in regional health centers, and instead must travel to large urban centers in order to be treated.[43] According to WHO, Venezuela’s national TB program had only 14 percent of its budget funded for 2018.[44]
Nutrition Crisis
The Venezuelan government stopped releasing official data on nutrition in 2007.[45] However, other sources, including information gathered by Venezuelan health professionals and nongovernmental groups, indicate worrying increases in levels of malnutrition.
In 2018, FAO indicated that between 2015 and 2017, 11.7 percent of Venezuela’s population—3.7 million people—was undernourished, up from less than 5 percent between 2008 and 2013.[46] In February 2019, a spokesperson for WHO confirmed that “Venezuela had indeed experienced an increase in the number of undernourished persons,” based on a joint report by FAO, PAHO, UNICEF, and WFP. [47]
Declining Food Security
The majority of Venezuelan households are now food insecure, meaning they lack sufficient access to safe and nutritious foods, according to the most recent available data.[48] The 2017 National Living Conditions Survey, carried out by three prestigious Venezuelan organizations, found that 80 percent of households were food insecure and 87 percent were living in poverty, up from 48 percent in 2014. The survey also showed 89 percent of households reporting they had insufficient income to buy food, and 61 percent of those interviewed reporting going to bed hungry.[49] Additionally, respondents reported a decline in the quality of food they were able to afford, opting for cheaper, but less nutritious foods.[50] Subsequently, in the 2018 National Living Conditions Survey, the researchers found a 48 percent increase in the number of poor households during 2018.[51]
Many factors explain this. First, Venezuela, which imports more than 70 percent of its food, has seen a 67 percent drop in food imports from the start of 2016 to the end of 2017.[52] Secondly, hyperinflation makes it impossible for many Venezuelans to purchase food in the regular markets.[53] They therefore rely on boxes with food items subject to government set prices, but these do not reach all Venezuelans who need them, provision of boxes is intermittent, and receipt is often linked to political support of the government.[54]
Increasing Prevalence of Acute Malnutrition
It is difficult to know the full extent of acute malnutrition in Venezuela as the government has not made data available and the prospect of government retaliation makes hospital workers afraid to record accurate data on malnutrition.[55] However, two NGOs in the country have been monitoring acute malnutrition and are able to provide some insight into the scope of the nutrition problem.
Caritas, a non-governmental organization supported by the Catholic Church, has been collecting data on malnutrition in children under age 5 in seven states throughout the country. For each state that Caritas observed, four to seven vulnerable sites were surveyed, with 725 to 1445 samples taken at each site. The assessment found an increase in childhood acute malnutrition from 2016 to early 2018 followed by a decline in some states surveyed.
Cáritas reported that MAM and SAM among children under age 5 increased from 10 percent in February 2017 to 17 percent in March 2018—a level indicative of a crisis, based on WHO standards.[56] Subsequent reports found that the overall rate in those states had decreased to 13.5 percent in July and 9.6 percent in September, but rates increased in the same period from 11.6 to 13.4 percent in Miranda state, and from 6 to 11.8 percent in Sucre state.
The non-profit Bengoa Foundation also found evidence of deteriorating nutritional conditions amongst children. Their study observed preschool children enrolled in school feeding programs in 10 different schools around the country. Three of the schools that Bengoa surveyed saw acute malnutrition rise from 3.3-3.4 percent in the 2014/2015 school year, to 15.5 percent in 2017. Several schools surveyed in the state of Anzoátegui had acute malnutrition rates of 16.7 percent.[57] Similar to areas assessed by Caritas, acute malnutrition prevalence in sites assessed by the Bengoa foundation surpassed crisis levels established by WHO.
The Caritas and Bengoa Foundation studies were of select populations within Venezuela and cannot be considered representative of the country as a whole. However, their data indicate high levels of acute malnutrition in at least some vulnerable communities.
Further data also shows malnutrition occurring in adults, particularly in pregnant women. Twenty-one percent of pregnant women in low-income communities were found to have acute malnutrition in a July-September 2018 Caritas survey.[58] Additionally, the 2017 National Living Conditions Survey reported that 64.3 percent of the survey population had lost weight in the previous year, with an average weight loss of 11.4 kilograms (nearly 25 pounds) in adults.[59]
Increasing Hospital Admissions with Acute Malnutrition
Venezuelan hospitals reported an increase in the number of children admitted for acute malnutrition, as well as an increase in consultations regarding acute malnutrition in 2018. The proportion of children being admitted to hospitals who were acutely malnourished in early 2018 was alarmingly high, ranging from 18 to 40 percent, in five different locations around the country.[60]
In mid-2018, The Venezuelan Society of Childcare and Pediatrics reported that 72 percent of children who sought emergency care at hospitals showed some level of poor nutrition as a result of an inadequate diet.[61] The group also reported a rapid increase in children at the hospitals with diet-related illnesses such as wasting and pellagra.[62] Wasting, or extreme thinness, is a form of acute malnutrition that results from insufficient caloric intake, whereas pellagra is caused by a vitamin deficiency. Both can be fatal if untreated.
A pediatric hospital in Venezuela indicated that in 2014 and 2015 around 30 children were admitted annually with severe acute malnutrition. This number jumped to more than 95 admissions annually in both 2016 and 2017. The proportion of children admitted for severe acute malnutrition in that hospital, compared to the total number of children who visited the hospital for the first time, rose from 5.4 in 2014 to 15.8 in 2016 and to 20 percent in 2017.[63]
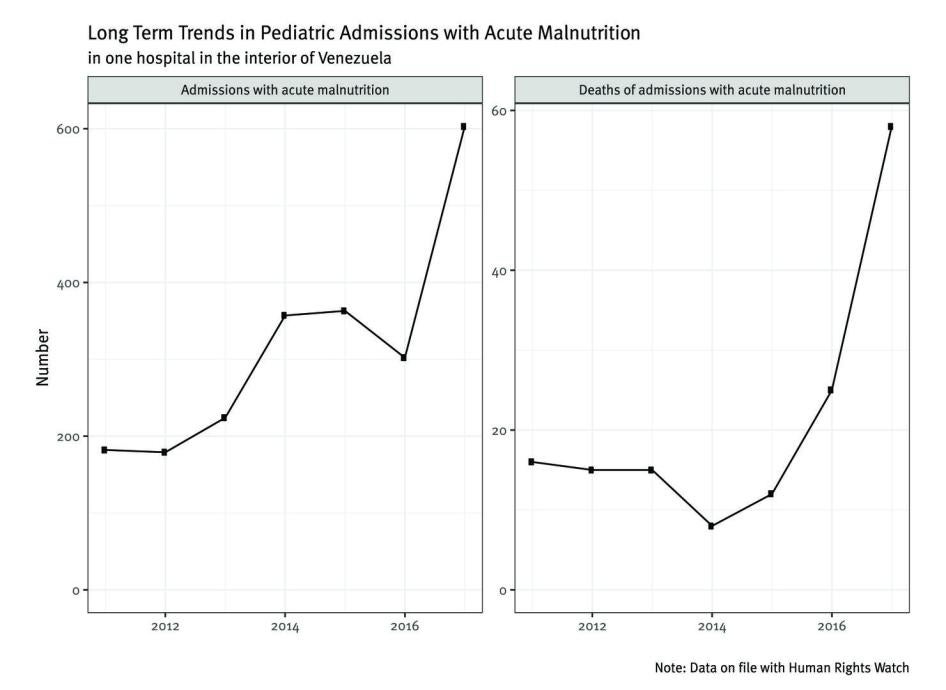
In one Venezuelan state, another hospital recorded between 180 and 220 children admitted annually with acute malnutrition between 2011 to 2013. Admissions rose to over 300 in 2014 before reaching over 600 children admitted with acute malnutrition in 2017—about a threefold increase in three years.[64]
Admission data shared with Human Rights Watch and Johns Hopkins University by health professionals from other hospitals around Venezuela shows high rates of acute malnutrition in children, with many of them dying of it. However, actual numbers are likely underreported due to healthcare workers’ fear to report the diagnosis of malnutrition; some hospitals even prohibit the diagnosis.[65]
Impact Across Venezuela’s Borders
Impact in Colombia
The unavailability of medicines, supplies, health providers, and basic health services are becoming a primary driver of migration from Venezuela to Colombia. Nearly 1,200,000 Venezuelans have fled to Colombia in recent years.[66]
Over the past two years, the Colombian Department of North Santander, which borders Venezuela, saw a sharp rise in “public health events” reported via surveillance systems among Venezuelans: from 182 in 2015 to 5,094 in 2018.[67] Colombia’s Epidemiological Surveillance System (Sivigila) reported that from January through August 2018, 2,398 public health events had occurred in patients from abroad, an almost threefold increase compared to the same period in 2017 (863 cases). The events reported among Venezuelans include malaria (36.8 percent), gender violence (12.6 percent), acute malnutrition in children under age 5 (6.6 percent), HIV/AIDS (6.2 percent) and TB (4 percent). The departments with the highest notification of Venezuelan patients were North Santander (30.1 percent), Guainia (17.2 percent), La Guajira (12.8 percent), Arauca (4.9 percent) and Vichada (4.3 percent).[68]
Infectious Disease
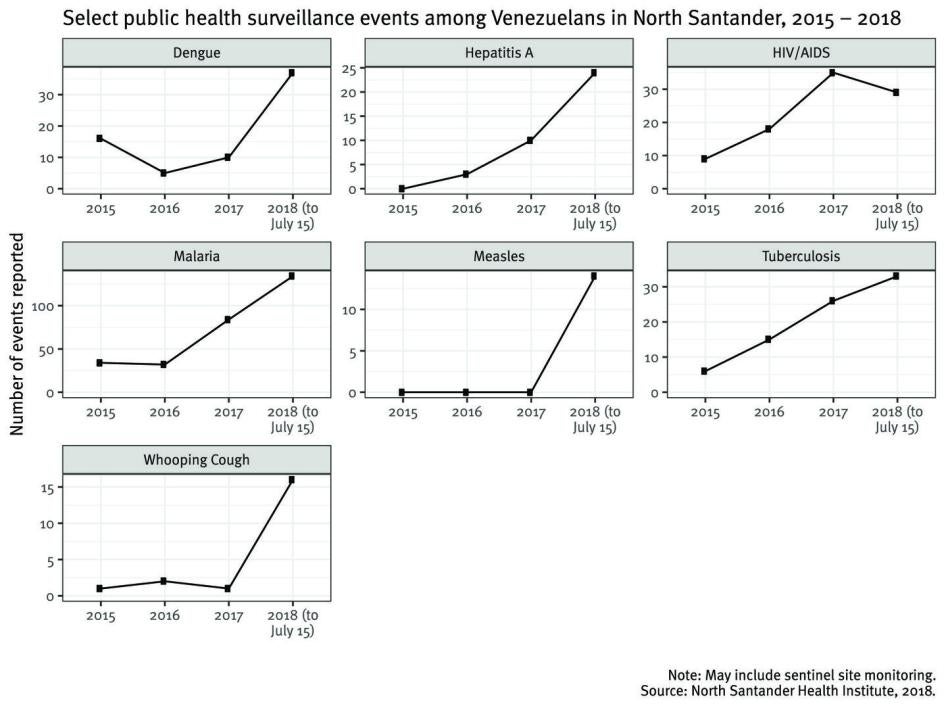
The most frequently reported infectious diseases among Venezuelans on the Colombian side of the border in 2018 were malaria, dengue, TB, HIV/AIDS, and Hepatitis A, all of which had increased since 2015. Vaccine-preventable diseases also increased greatly, from 1-4 events annually in 2015-2017 to more than 200 in 2018; the majority of the 2018 cases were whooping cough and measles.[69]
The increasing infectious disease caseload is likely due to both growing numbers of arrivals and deterioration of population health within Venezuela. One of the efforts to combat the border health crisis is the provision of vaccinations by Colombian authorities; they provided 58,580 and 789,292 in 2017 and 2018, respectively, at three border crossings in North Santander (in addition to lower numbers elsewhere) to vulnerable populations, the majority of whom are Venezuelan.[70] This means there was a 1,274 percent increase during this period.
Women’s Health and Gender-Based Violence
There are at least 454,000 Venezuelan women migrants in Colombia.[71] Many of them face challenges accessing health care as well as threats of sexual exploitation and abuse, trafficking, and sexual and reproductive rights violations. Over 12 percent of reported public health events in 2018 were categorized as gender-based violence, and some evidence suggests indigenous women face even greater threats.[72]
Maternal and Infant Health
According to a 2018 report by the government of Colombia, more than 8,000 pregnant Venezuelan women had entered Colombia who were expected to give birth in the country; the majority of this population did not have any type of prenatal care in Venezuela.[73] Among all pregnancies recorded in 2018, 673 were among children aged 13-17, 57 of them members of indigenous groups.[74]
The number of children and pregnant mothers from Venezuela provided care at the Colombian Institute of Family Welfare (Instituto Colombiano de Bienestar Familiar) rose from 22,113 in 2017 to almost 55,544 between January and September 2018 in all its programs.[75]
Health surveillance in North Santander demonstrates an increasing number of maternal and peri-/neonatal health events among Venezuelans (Figure 2). Forty-five Venezuelan women experienced serious illness tied to pregnancy or childbirth and seven died in 2018, whereas prior to the crisis in 2015, only two cases of extreme maternal morbidity and no cases of maternal mortality were reported in North Santander.[76]
Similarly, low birth weight and peri-/neonatal mortality among Venezuelan infants have risen drastically; four newborns died in 2015 compared to 211 in 2018.[77] Declines in maternal and infant health most likely reflect the unavailability of care in Venezuela with Colombian physicians describing a surge in demand for prenatal care and increased numbers of deliveries among women reporting insufficient prenatal care.[78] Erasmo Meoz University hospital in Cúcuta, the only tertiary hospital in North Santander, reports delivering 2,944 Venezuelans in 2018.[79]
Migration Burden on the Health System
According to the Departmental Health Institute, in 2017 and 2018 in North Santander, emergency medical services treated 34,492 Venezuelans in public facilities and an additional 12,144 cases at mobile clinics.[80] In 2018, mobile health units were scaled up with the aim of reducing the burden at health facilities. While the government has the capacity to address Venezuelan health needs, sustainability is a concern; both WHO and UNHCR are currently providing support to public facilities, but the Colombian government bears most of the cost.
In July 2018, Colombian officials said the government had provided Venezuelan immigrants 2,200 million Colombian pesos (about US$730,660) in non-emergency care owing to judicial rulings entitling the Venezuelans such care, and that does not include vaccinations, which are offered free to all comers.[81] The Colombian government is also supporting additional care in selected individual cases, to the extent that resources allow, on a humanitarian basis through special permission; for example, this is being done with some cases of childhood cancer.
Erasmo Meoz University Hospital, the only tertiary hospital in North Santander, treated 14,953 Venezuelan patients in 2018.[82] Demand for medical attention, meanwhile, has increased among both Venezuelans and Colombians who lived in Venezuela for a long time and returned to Colombia (the so-called “returnees”). However, official figures underestimate the extent of the burden because returnees are reported as Colombian. The increased caseload has translated to longer wait times, capacity concerns, and increased costs for Colombian health facilities. Space in intensive care units is limited as are referral options for Venezuelans because most lack Colombian insurance. Specialty hospitals, usually in major cities, are often unreachable because of cost, or they may not have access depending on their migration status.[83]
Nutrition
In an April 2018 survey conducted by the International Rescue Committee (IRC), food was the priority need for those living in Venezuela and the second most-often reported need for Venezuelans in Cúcuta (80 percent); as of April 2018, an estimated 611,000 food insecure Venezuelans and returnees were in Colombia.[84] Cases of severe acute malnutrition (SAM) among Venezuelan children under age 5, according to Colombian official data, increased since 2015 when no cases were reported to 2, 13, and 360 in 2016, 2017, and 2018, respectively. Three Venezuelans died due to malnutrition in 2017, and 11 did so in 2018.[85]
The Red Cross has initiated screening at several health posts, and shelters and community kitchens also have nurses that offer screening, but programs are not widespread and follow-up presents a challenge because populations are mobile. We did not have access to Red Cross data, but one communal kitchen told us it had identified ten children with acute malnutrition who were receiving supplementary food.[86]
The Human Rights Watch and Johns Hopkins team conducted a rapid screening of 115 children 6-59 months of age at a communal kitchen near the Cúcuta border, and found no cases of severe or moderate acute malnutrition. However, the team found that eight children (7 percent of the total) were at risk of acute malnutrition.[87] In North Santander more generally, children identified as malnourished are provided supplementary foods by the Colombian government in coordination with WFP, but it is difficult to assess if coverage is adequate given the lack of available data on prevalence of acute malnutrition and challenges estimating population size.
Impact in Brazil
Nearly 100,000 Venezuelans have fled to Brazil in recent years.[88] Most of them entered the country through Roraima state, which borders Venezuela, and have stayed there given that it is a remote state with limited connections to the rest of Brazil, let alone to other parts of the region. Brazilian and UN authorities have relocated over 5,250 Venezuelans to other parts of the country.[89]
Many Venezuelans crossed the border to seek medical care, while others have sought care once living in Roraima. In February 2019, Roraima’s governor signed a decree declaring that the state’s public health system had reached a “state of calamity” as a consequence of the increased influx of Venezuelans. This declaration should help the state in obtaining emergency medicines and supplies.[90]
Infectious Diseases
The impact of the Venezuelan crisis on transnational public health is dramatically evident in Roraima.
An outbreak of measles, a vaccine-preventable infection, that started in Venezuela in 2017 due to lapses in vaccination coverage, has now crossed the border to Brazil. The last confirmed cases of measles in Brazil had occurred in 2015. In February of 2018, the first new cases were reported in Roraima, followed by cases in Amazonas, which has the largest number of confirmed cases as of February 2019 (9,804).[91] As of February 2019, a total of 10,394 cases had been confirmed in Brazil, including 12 deaths.[92]
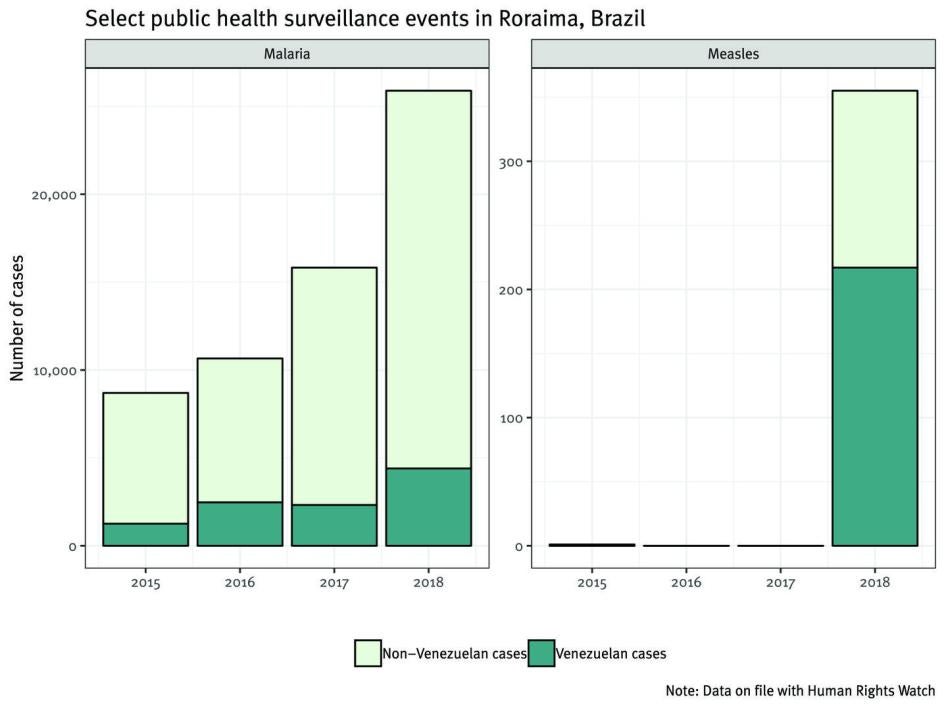
The strain of the measles virus (D8) in Brazil is identical to the strain causing the outbreak in Venezuela. As of February 2019, the majority (61 percent) of confirmed cases in Roraima had occurred among Venezuelans, particularly among indigenous people, but the rapid spread among Brazilians highlights gaps in vaccination coverage, especially in Boa Vista.[93] To control the outbreak, public health authorities conducted a three-day vaccination campaign in August 2018, where 38,744 doses of measles vaccine were administered among children under age 5 in Roraima.[94] Measles vaccination coverage in Boa Vista improved from 66.8 percent to 95.3 percent following the campaign.[95] As of February 2019, four people—three Venezuelans and one Brazilian—had died from measles associated with this outbreak in Roraima.[96]
Malaria has also surged in Roraima following the dramatic rise of malaria in Venezuela, particularly in Bolivar, the Venezuelan state bordering Roraima. The number of cases of malaria among Venezuelans increased from 1,260 in 2015 to 2,470 in 2016 and 4,402 in 2018, and has continued to rise since.[97] Physicians told us that compared to Brazilians, Venezuelans were more likely to die from malaria, were more likely to arrive to the hospital very sick, and their management was often complicated by malnutrition.[98]
Cases of TB and HIV have also been increasing among Venezuelans in Roraima. Between January and December of 2018, 60 new cases of TB among Venezuelans had been identified by the Roraima health authorities. This was more than the total number of TB cases among Venezuelans in the preceding five years (2013 to 2017), when there was a total of 32 TB cases reported among Venezuelans in Roraima.[99] The number of cases in 2018 represents an almost seven-fold increase compared to the same period in 2017. This increase strains the Brazilian health system, since TB treatment is complicated and labor intensive.
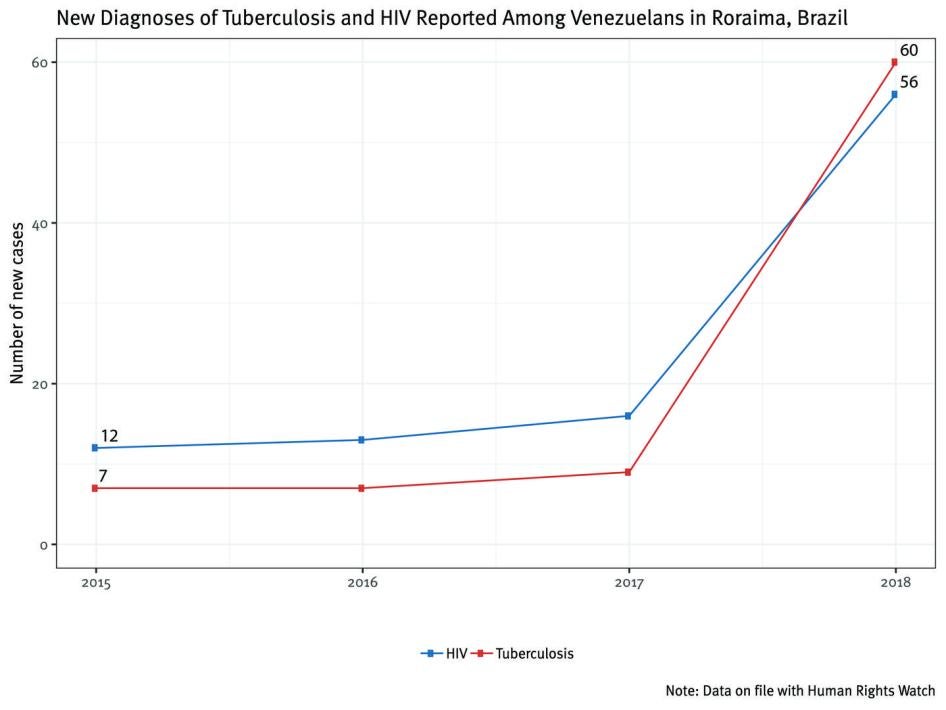
According to Roraima’s Department of Health Surveillance, there were 56 new cases of HIV among Venezuelans in 2018.[100] This represented more than a three-fold increase from 2017. At the Specialty Clinic Colonel Mota, which is the primary source of outpatient HIV care in Roraima, 171 Venezuelans were receiving ARV therapy for HIV as of August 2018.[101] Physicians at the clinic told us that Venezuelan patients presented to care very sick and often malnourished or with life-threatening opportunistic infections. More than half of the patients at the Roraima General Hospital infectious disease ward in August 2018 were Venezuelans being treated for AIDS symptoms. Four patients reported that ARV therapy had been unavailable in Venezuela for at least seven months, and prior to that ARV medication shortages were frequent. They were forced, therefore, to interrupt life-saving medications or take inadequate therapy, which can lead to HIV-drug resistance and limits future options for therapy.
Migration Burden on the Healthcare System
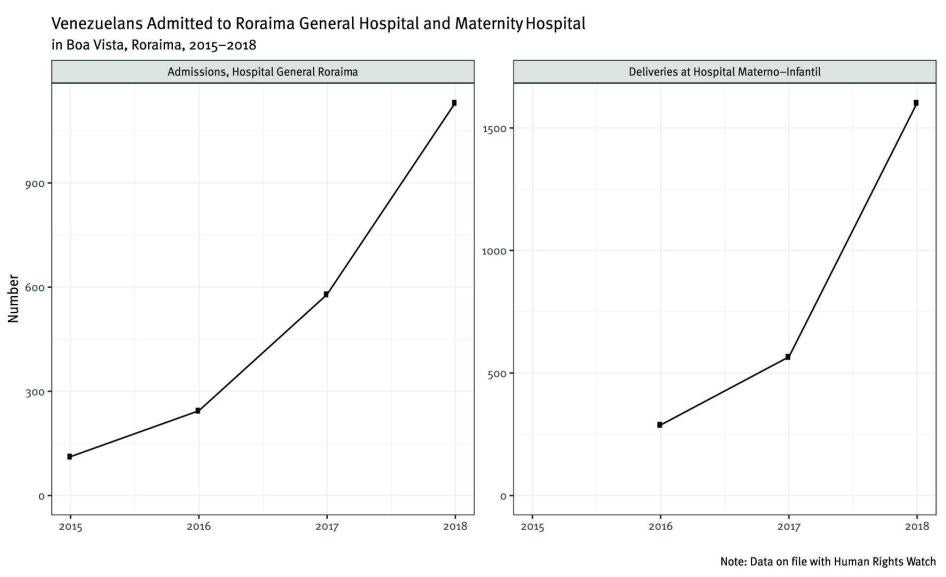
The influx of Venezuelans to Roraima has severely strained the state’s healthcare system. The largest hospitals in Roraima— the General Hospital of Roraima (306 beds) and the Maternity Hospital (266 beds), both in Boa Vista—experienced dramatic increases in utilization in the first half of 2018. At the General Hospital of Roraima, the number of Venezuelans hospitalized more than doubled compared to the same period in 2017, and urgent care and emergency room visits almost quadrupled. During the first quarter of 2018, deliveries among Venezuelan women at the Maternity Hospital were 2.5 times higher than during the same period in 2017, and doctors projected the numbers would to continue to rise.[102]
Markedly increased patient volume at these two hospitals was straining resources. Hospital directors reported shortages of basic medications and supplies, including antibiotics, cardiac medications, intravenous fluids, syringes, and EKG leads.[103]
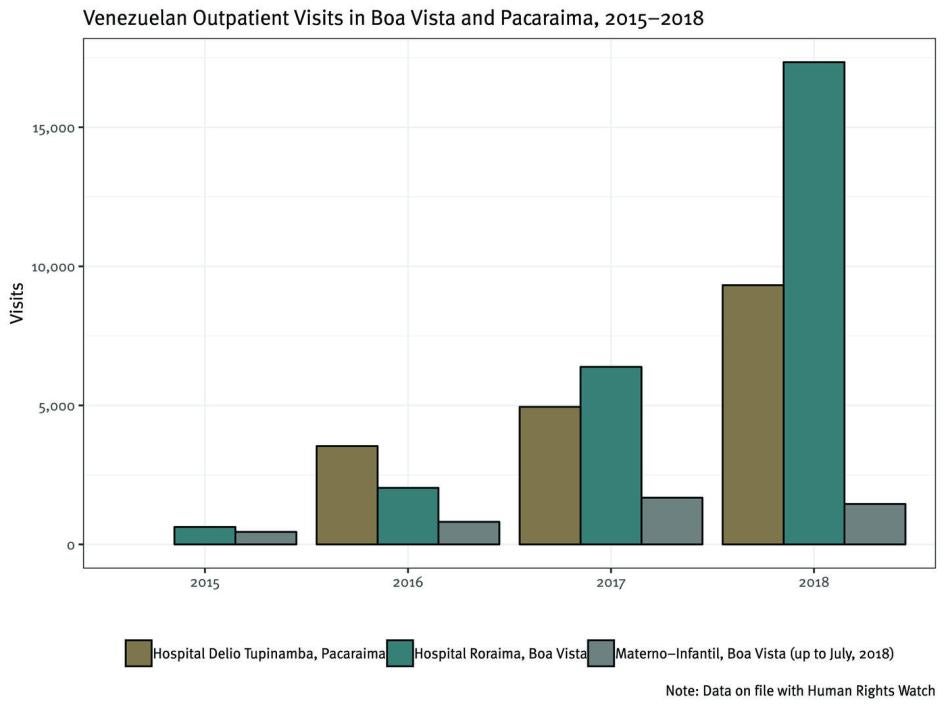
In addition to increased volume, the healthcare system has been strained by the severity of illness among Venezuelan patients, which reflects the scarcity of care and medications in Venezuela. Unsurprisingly, health problems are most severe among the poorest migrants. Venezuelans living in shelters and in the street reported to Human Rights Watch and Johns Hopkins University staff significant health needs: 35 percent of the people interviewed said they needed care for a chronic condition (asthma, diabetes, cardiovascular disease, HIV, TB, or seizure disorder), and 60 percent reported weight loss of over 10 pounds prior to arrival in Brazil. More than 80 percent of Venezuelan women reported food insecurity during pregnancy.[104] Malnutrition and untreated chronic conditions resulted in complications and difficulty to treat cases. At the General Hospital of Roraima, for example, more than half the patients admitted to the oncology ward were Venezuelans with metastatic malignancies, many without option for cure.[105] At the Maternity Hospital, a housing complex for mothers with newborns in the neonatal intensive care unit was primarily occupied by Venezuelans and the hospital had to borrow additional incubators to care for a growing number of infants born prematurely. The hospital director reported that Venezuelan women had a much higher risk of complications due to lack of prenatal care, malnutrition, anemia, and malaria during pregnancy.[106]
To alleviate the burden on hospitals, basic healthcare in Brazil is provided as part of the federal government’s Welcome Operation (Operação Acolhida). The Armed Forces have deployed physicians, pharmacists, nurses, and public health officials to Roraima to provide care to Venezuelans.[107] Healthcare teams visit each shelter two to three times a week, where they care for common conditions such as diarrheal illnesses, intestinal parasites, respiratory infections, skin infections, and malnutrition. In addition, physicians have been deployed to the border town of Pacaraima where they staff a screening and vaccination post at the immigration point of entry.
As of August 2018, Venezuelans who apply for asylum or residency in Pacaraima (but not in Boa Vista) were being vaccinated against measles, mumps, rubella, tetanus, whooping cough, and yellow fever unless they refused or produced documentation of adequate vaccination. Between March 24, 2018 and August 30, 2018, 4,455 Venezuelans received medical services at this site. In addition, a military-style healthcare facility was inaugurated in June 2018 with private rooms for clinical examination and phlebotomy, a pharmacy stocked with commonly used medications, and a room with hospital beds for observation and capacity for simple procedures. In September 2018, the federal government started providing vaccination for applicants in Boa Vista.[108]
The Venezuelan Government’s Responsibility
The humanitarian crisis in Venezuela is related to a broader collapse of the country’s economy. Many analysts have argued that the government’s own policies have played a role in causing the economic crisis or allowing it to persist.[109] Regardless of the situation’s underlying causes, the government is obligated to make every effort to use the resources at its disposal to meet its minimum obligations under international law and reverse the erosion in Venezuelans’ access to adequate health services and food. However, under the presidency of Nicolás Maduro, the Venezuelan government has denied the crisis, hidden health statistics and data, harassed health professionals who speak out about the reality on the ground, and made it harder for sufficient humanitarian assistance to reach the Venezuelan people. Through these policies and practices, authorities have contributed to the worsening humanitarian crisis documented in this report.
The Rights to Health and Food
The ICESCR—ratified by Venezuela in 1978—guarantees everyone the right to “the enjoyment of the highest attainable standard of physical and mental health,” as well as the right to an adequate “standard of living” that includes “adequate food.”[110] The right to health is also provided for in the Venezuelan Constitution.[111]
Venezuela’s government is obliged to work toward the progressive realization of these rights over time “by all appropriate means” and “to the maximum of its available resources.”[112] The Committee on Economic, Social and Cultural Rights, which provides authoritative guidance on states’ implementation of the ICESCR, has affirmed that states also have an absolute and immediate obligation to ensure “minimum essential levels” of all covenant rights, “including essential primary health care.”[113]
In 2013, the UN special rapporteur on the highest attainable standard of physical and mental health noted that, “[w]hile several aspects of the right to health are understood to be progressively realizable, certain core obligations cast immediate obligations on States, including the provision of essential medicines to all persons in a non-discriminatory manner.”[114] These essential medicines, according to the rapporteur, include painkillers, anti-infectives, anti-bacterials, antituberculars, anti-retrovirals, blood products, cardiovascular medicines, vaccines, and vitamins. The UN Human Rights Council, for its part, has repeatedly stressed that states should maintain essential medicines that are affordable, safe, effective, and of good quality.”[115]
Under the Convention on the Rights of the Child, ratified by Venezuela in 1990, states should guarantee “the right of the child to the enjoyment of the highest attainable standard of health and to facilities for the treatment of illness and rehabilitation of health.” The Convention specifically states that states parties should take appropriate measures “to diminish infant and child mortality, “to combat disease and malnutrition,” and “to ensure appropriate pre-natal and post-natal health care for mothers.”[116]
The Committee on Economic, Social and Cultural Rights has noted that the right to adequate food “is realized when every man, woman and child, alone or in community with others, has the physical and economic access at all times to adequate food or means for its procurement.” The right to adequate food implies that it is available “in a quantity and quality sufficient to satisfy the needs of individuals” and that it is accessible in ways that “do not interfere with the enjoyment of other human rights.”[117] The Office of the High Commissioner for Human Rights (OHCHR) has emphasized that:
The right to food is not a right to be fed, but primarily the right to feed oneself in dignity. Individuals are expected to meet their own needs, through their own efforts and using their own resources. To be able to do this, a person must live in conditions that allow him or her either to produce food or to buy it…. The right to food requires States to provide an enabling environment in which people can use their full potential to produce or procure adequate food for themselves and their families.[118]
Similarly, the UN special rapporteur on the right to food has interpreted that right as requiring “regular, permanent and unrestricted access, either directly or by means of financial purchases, to quantitatively and qualitatively adequate and sufficient food.”[119]
The ICESCR requires states parties not only to make individual efforts, but to work “through international assistance and cooperation” to ensure the realization and protection of all covenant rights globally.”[120] This speaks primarily to the principle that relatively wealthy states should provide assistance and cooperation to states that need it. However, it also implies that states have at least some degree of responsibility to seek international assistance and cooperation when they lack the independent means to fulfill their obligations under the ICESCR.[121]
Venezuela’s government may have valid reasons for eschewing particular sources or types of assistance, but it should endeavor to identify appropriate sources of external support to the extent necessary to address the country’s health crisis and shortages of food.
Denial of the Crisis
The public denial of Venezuela’s humanitarian crisis has been a continuous government policy for several years. In addition, high-level authorities have publicly provided misleading or false information on the extent of the crisis.
On May 16, 2018, President Maduro said that “everything [that has been said] about measles and diphtheria is a lie, we vaccinate the whole community for free” and that “with regards to food, Venezuela has unique policies, which have enabled us to carry on with a program allowing us to maintain levels of food that are necessary for the people.”[122] Days later, the undersecretary of health, Indhriana Parada, gave a speech at WHO highlighting the “achievements” of the Venezuelan health system. She claimed that “in Venezuela there is no humanitarian crisis” and that “Venezuela guarantees access to basic medicines to the most vulnerable groups through distribution policies.”[123] In the case of malaria, she claimed government measures had “reduced incidence by 50 percent.”[124] Similar statements have been made in recently by other high-level officials.[125]
To the extent the government of Venezuela has acknowledged the existence of shortages, it has done so without recognizing the full extent of the problem nor all the factors that contribute to them, including its own policies and practices.
For example, a July 2018 report by PAHO, UNAIDS, and the Venezuelan Health Ministry acknowledges shortages of the materials needed to test and prevent HIV, malaria, and TB. It blames lack of financing, insufficient pharmaceutical producers in Venezuela, and the black market for medicines, among other reasons.[126]
In September 2018, Foreign Affairs Minister Jorge Arreaza stated before the UN Human Rights Council that “there is no humanitarian crisis in Venezuela,” but instead an “economic crisis,” which he claims is caused by sanctions imposed by the US and the European Union, which he called “coercive unilateral measures” that were making it “difficult for Venezuela to receive and import the basic needs to provide nutrition and health to our people.”[127]
Most sanctions—including some imposed by the United States, Canada, the European Union, and several Latin American governments—are limited to canceling visas and freezing assets of key officials implicated in abuses and corruption.[128] They in no way target the Venezuelan economy.
In 2017, the United States also imposed financial sanctions, including a ban on dealings in new stocks and bonds issued by the government and its state oil company.[129] They do include an exception for transactions to purchase food and medicines. On January 28, 2019, the United States expanded sanctions to include the Central Bank of Venezuela and the state-owned oil firm PDVSA.[130] To the extent that these latest sanctions have an impact on the Venezuelan authorities’ ability to import medicines and food, they could worsen the current humanitarian crisis. However, it is impossible to argue that these sanctions have caused the crisis because as this report shows, the crisis precedes them.
Hiding Health Statistics and Information
The Venezuelan government has tried to conceal the crisis by failing to produce official health information on a regular basis. Most notably, the government, after publishing weekly epidemiological bulletins since 1938 with information about more than 72 reportable illnesses, stopped publishing them in 2015.[131]
After nearly two years in which Venezuela’s Health Ministry did not publish these monthly bulletins, it suddenly released, in May 2017, epidemiological bulletins for half of 2015 and all of 2016. The bulletin corresponding to the last week of 2016 was especially noteworthy as it showed a 30 percent increase in infant mortality, a 65 percent increase in maternal mortality, a resurgence of diphtheria, and increases in the incidence of malaria, Zika, TB, and Hepatitis A.[132]
Following the publication of this information, President Maduro fired then Health Minister Antonieta Caporale and replaced her with a staunch supporter, Luis Lopez.[133] The epidemiological bulletins were promptly taken down from the Health Ministry’s official website and have not been posted again. Since then, no additional bulletins have been published, nor have authorities published any other official health data regarding the topics that were covered in seven decades of epidemiological bulletins. Accordingly, no official information on these health issues in Venezuela is publicly available for 2017 and 2018.
This was not the first time the government fell into “epidemiological silence.” The OHCHR reported in June 2018 that “the Government [of Venezuela] refused to release information required to assess the dimension and consequences of the health crisis, such as the weekly epidemiology bulletins and the yearbook on mortality.”[134] The Venezuelan human rights group PROVEA has reported that during the Chávez and Maduro years, the government has suspended epidemiological information three times.[135]
The lack of official information does not mean the government lacks the data or the ability to collect it. In fact, the Venezuelan government regularly provides information to PAHO, which then includes the official data conveyed by Venezuelan authorities in its own reports. For example, the epidemiological updates on diphtheria, measles, and other illnesses published by PAHO include information that, as indicated in the updates themselves, is “data from the Venezuelan Ministry of Popular Power for Health and reproduced by PAHO/WHO.”[136]
Several doctors interviewed by Human Rights Watch in various parts of the country said they continue to gather and systematize data, and report it to national health authorities, but it is not made public by the government. This is the case, for example, of a doctor in Caracas, who explained that he works in a “sentinel” hospital, which is part of the government’s food and nutritional surveillance system (SISVAN) that evaluates the nutritional status of Venezuelans. The doctor explained that health authorities “come every month and ask for the data [on malnutrition]. That is why I know that they have the data, month by month, at least from our hospital. It is not that I bring it to them, it is that they come to request it. They have it but fail to publish it.”[137] Another doctor in the interior of the country told us they report data but “the numbers don’t appear anywhere.”[138]
One doctor interviewed by Human Rights Watch provided us with statistics on child malnutrition for one of the Western states of the country, which she had obtained from a colleague at the National Institute for Nutrition.[139] Another doctor provided Human Rights Watch data that the hospital where he works systematically gathered and analyzed in 2016, 2017, and 2018 on births, maternal mortality, mortality rates, as well as cases of malaria and diphtheria, among other illnesses. The doctor said the information had been shared with authorities.[140] And a group of doctors provided Human Rights Watch with a copy of a document that contained information on child mortality, malnutrition, and malaria incidence in one Venezuelan state that they had given to state health authorities, the ombudsman, and the Attorney General’s Office. The document claims that the response was “epidemiological silence and a denial of reality” from authorities.[141]
Harassment and Retaliation Against Health Professionals Reporting on the Crisis
In January 2018, President Maduro called those who drew attention to the humanitarian crisis “bandits” and “traitors to the fatherland.”[142] In a country with no judicial independence, where critics have been arbitrarily jailed and subjected to abuse, and where hunger and access to social services, including health, has been used as a mechanism of social and political control, these words serve as threats that need to be taken seriously.[143]
In October 2016, Human Rights Watch released a report that documented instances of retaliation against medical personnel who spoke out against the crisis.[144] During research in 2018 for this new publication, we found that government and hospital authorities have continued to harass and retaliate against health professionals, but now not only for protesting the shortages, but also for reporting on statistics and the real reasons why patients are being hospitalized or die.
Independent media outlets in Venezuela and the local group Espacio Público, which monitors free speech in the country, have reported several instances in which health professionals suffered retaliation or harassment for speaking out about the crisis in 2018.
In February 2018, members of the Bolivarian National Intelligence Service (SEBIN) reportedly threatened Dr. Feder Álvarez with detention after he spoke publicly about the death of six children at a hospital due to food poisoning after eating food not fit for human consumption.[145]
Also in February, the Venezuelan Society of Puericulture and Pediatrics said that hospital staff allegedly threatened to fire doctors from a hospital in Nueva Esparta state after they demonstrated to call attention to the crisis, and that members of the Bolivarian National Guard did not allow doctors in another hospital to demonstrate, calling them “guarimberos”—a term Venezuelan authorities use to describe government opponents.[146]
In July, seven pediatricians from a hospital in Cojedes state were fired months before their contract ended and after participating in a demonstration about the health crisis, according to Espacio Público. One of the doctors allegedly said hospital authorities had accused them weeks earlier of being “guarimberos.”[147]
In October, members of Venezuela’s investigative police (CICPC) reportedly detained five nurses as they participated in a demonstration on medicine shortages in Anzoátegui state, and held them for two days.[148]
In February 2019, a nurse working at the main children’s hospital in Caracas said security guards and military personnel forced her into a room where they threatened her with their firearms while asking why she was providing food and taking pictures of patients, according to news reports. She was allegedly held for 40 minutes and forced to sign a piece of paper she could not read, she said.[149]
Also in February 2019, Venezuelan officials raided the Mavid Foundation, an organization that has been supporting access to medicines for people living with HIV. HIV activists connected to the Mavid Foundation, Jonathan Mendoza, Wilmer Alvarez, and Manuel Armas Jhas, were detained in a raid, according to the Global Network of People Living with HIV.[150]
The OHCHR has also reported that the government has been threatening, and in some cases arbitrarily arresting, doctors and patients speaking out about the health situation.[151]
For example, local media reported that in May 2018, security forces violently dispersed a demonstration by doctors from the Adolfo Pons Hospital in Zulia state, who were protesting the scarcity of medicines and medical supplies. State police officers allegedly beat several doctors and detained two; one of them had several cuts on his face and a broken nose, according to Venezuelan press accounts.[152] In March 2019, members of security forces and armed pro-government groups allegedly threatened parents of children being treated in the main pediatric hospital in Caracas with rape and detention if they continued to “spread [their] vicious lies” about what was happening inside the hospital.[153]
Each of the 25 doctors and medical personnel interviewed by Human Rights Watch nationwide who work in public hospitals in Venezuela or represent networks of doctors who do, touched on the issue of censorship of health information. They said that hospital authorities forbade them from providing statistical information to people outside of the hospital, from talking about the health crisis in public or to hospital administrators, or from including specific details of diagnoses in patients’ records.[154]
Two doctors explained that hospital administrators in public hospitals had imposed restrictions on what can be included in patients’ medical records, specifically related to child malnutrition. They said they had received an “implicit” or “verbal order” not to include “malnutrition” as a diagnosis in the medical histories or records of patients.[155]
A doctor who teaches residents in a graduate program in a public hospital said residents are threatened with being expelled from the program or their hospital if they include a malnutrition diagnosis in medical records, so they do not list it at the top of such records.[156] Another doctor said that any reference to the patient being malnourished can only be added at the very end of the medical history or report, after several other illnesses and conditions are listed. That way, a doctor said, when the cause of hospitalization or death is reported, it does not mention malnutrition.[157] As a consequence of this practice, doctors said, any available statistics will not show the real degree of malnutrition in patients because it is being purposely hidden and under-reported.[158]
Many doctors continue to gather data on malnutrition and child mortality, but do so on the sly for fear of retaliation.[159] Some have come up with alternative ways to gather data without raising suspicions by hospital administrators, such as having residents pretend that the data will be used for a personal academic project on which they are working.[160] One of them took hand-written notes from medical records and hid them to share with us for this publication, and shared official data from the hospital under the condition that sources and hospitals would not be identified in this publication.[161]
Nearly all doctors and medical personnel interviewed by Human Rights Watch insisted on remaining anonymous for fear of retaliation. For example, a doctor from a pediatric hospital who provided us with information on malnutrition and on shortages of basic medicine and medical supplies at the hospital told us:
I wish to be working here, even in these horrible conditions, so that I can help, so that I can see the situation and share the information. I share information with reporters, and with organizations like yours. This is why I don’t want you to mention me. Because I want to stay here. If not, who will tell these stories? I cannot risk being fired.[162]
Several doctors told us hospital authorities have continued to harass and retaliate against medical professionals who speak out about the crisis. In some cases, doctors interviewed by Human Rights Watch said that the retaliation included suspending the person from work, sending her on “forced holidays,” forcing her to retire, or transferring her to a location where she would be downgraded in her assignments.[163] Another form of pressure has been the presence of security forces and armed pro-government gangs inside hospitals.[164]
The ability to obtain limited data from doctors in Venezuela, despite the courage many continue to show, is becoming more difficult given the large numbers of medical professionals who have left the country. The OHCHR has reported that in recent years, according to local sources, many medical doctors and nurses emigrated to other countries in the region, “mainly due to low wages and the lack of conditions to provide adequate health services.”[165]
Insufficient Assistance Reaching Venezuela
The Venezuelan government has sought some assistance from key UN agencies, but according to humanitarian actors, UN agencies, and the Venezuelan health ministry itself, the help requested is insufficient to meet the urgent needs of the population. All humanitarian actors interviewed by Human Rights Watch and Johns Hopkins University have said that they are willing and able to provide additional assistance to Venezuela, which is much needed, and that the lack of an adequate and comprehensive assessment of the full extent of the crisis, due to the government’s suppression of information about it, makes it impossible to plan an adequate response to the current situation and to prevent further deterioration of Venezuelans’ health.
UN Agencies
According to publicly available information and information provided by UN agencies to Human Rights Watch and Johns Hopkins University, the Venezuelan government has sought some humanitarian aid, in particular from UNICEF and PAHO. In February 2019, a spokesperson for WHO said PAHO was providing medicines and vaccines to Venezuelan hospitals, as well as supporting the maintenance of services in high-complexity priority hospitals, which included training of health personnel and the prevention of infectious diseases.[166] On March 1, 2019, OCHA said that “within the framework of existing agreements with the Government, UN agencies were working to respond to the humanitarian needs of the population.”[167]
In response to an information request submitted by Human Rights Watch, UNICEF said in April 2018 that the Venezuelan government was “expanding the cooperation with the UN System in critical areas such as health and nutrition,” mentioning, among other initiatives, that UNICEF was supporting a measles immunization campaign, a program to provide nutritional assistance, anti-malaria treatment, anti-retroviral treatment, and HIV tests and diphtheria antitoxin.[168] By the end of 2018, UNICEF had provided measles vaccinations to 990,000 children age 5 and under.[169] UNICEF has also distributed 100 tons of nutritional supplements for 150,000 children in Venezuela.[170]
In June 2018, after a visit to the country, PAHO reported that it had increased its activities in Venezuela and in neighboring countries, deploying more than 60 staff members and establishing six field offices (five in Colombia and one in Brazil).[171] This is in addition to the PAHO center in Caracas.[172] It said it was providing support to Venezuela’s Health Ministry to implement a national plan to stop the outbreaks of measles and diphtheria, including by vaccinating children and indigenous populations, and purchasing lab supplies to diagnose diphtheria and measles. It also provided quick tests to diagnose malaria and said it would provide 150,000 treatments for different types of malaria in 2017 and 2018. PAHO also provided the Venezuelan government with support to design and implement a vaccination campaign launched in April 2018 to immunize nine million people.[173] By June 2018, PAHO had trained more than 8,000 medical personnel, including 3,500 vaccinators.[174]
The July 2018 report by PAHO, UNAIDS, and the Venezuelan Health Ministry said that UNICEF, UNAIDS, and humanitarian nongovernmental groups had donated ARV treatment for children and adults, as well as HIV tests and medicines to treat malaria and TB.[175] In September 2018, the Global Fund to Fight AIDS, TB and Malaria, with the support of UNAIDS, PAHO, and civil society groups, approved a US$ 5 million allocation to coordinate support to combat HIV, TB, and malaria in Venezuela.[176]
While the provision of this assistance is a welcome step, information provided by UN agencies and interviews with key informants, including health professionals and humanitarian actors working in Venezuela, show that humanitarian assistance reaching people in Venezuela is still inadequate to address the urgent needs of the population.
The July report in which the Venezuelan government, PAHO, and UNAIDS participated states that ARV treatment that the ministry is obtaining through the PAHO Rotary Funds and purchases from Indian pharmaceutical companies, together with donations from PAHO, UNAIDS, and UNICEF “are insufficient to cover required needs.” The report estimated that available “limited” medication would cover only one or two months of treatment of some people living with HIV.[177] The report lays out a three-year plan that would cost more than $122 million to address all needs in this area.[178]
The UNICEF letter to Human Rights Watch notes that “more needs to be done by all to reach everyone affected by the crisis.”[179] Similarly, Grant Leaity, UNICEF deputy emergencies director, told Human Rights Watch in February 2018 that “the government ha[d] taken measures, but they are not sufficient [nor] adequate” and that UNICEF was not supplying the government “in any significant quantity.”[180]
PAHO, for its part, has reported that “immediate action is required to address short-term priorities, to reduce the impact of health workforce migration, rationalize existing resources while mobilizing additional resources, with the purpose of addressing disease outbreaks and increasing capacity of the system to provide comprehensive care for priority conditions.”[181] For instance, as of June 2018, PAHO had provided standard emergency medical kits, each of which provides medicines and medical supplies for 10,000 people, to 11 Venezuelan hospitals, and it was planning to distribute an additional 40 kits in 21 priority hospitals.[182] The distribution of these kits continued in 2019.[183] In addition, in October, as a part of its Safe Hospitals Initiative, PAHO distributed more than 3,000 boxes of medicines and supplies across 18 hospitals, 13 comprehensive community health areas, and eight health institutions.[184] However, Venezuela is home to more than 200 hospitals and these kits are not reaching many patients who need them.[185]
Although no comprehensive, official data to assess the success of the vaccination plan exists, local experts have said that it does not cover the needs of the population. The Venezuelan Puericulture and Pediatrics Society’s president said that 2.9 million children were excluded from the program, as it covered only 70 percent of the demand.[186] He added that “the 89,660 doses of biological material bought by the ministry through the PAHO Rotary Fund excludes approximately 411,000 women, out of the 550,000 who become pregnant every year.”[187] Félix Oletta, a former health minister and member of the Venezuelan Public Health Society, said in September that the vaccination rate for members of vulnerable communities, mostly from indigenous groups, is under 20 percent.[188] Similarly, the non-governmental organization United Doctors Venezuela warned that 3.5 million diphtheria-tetanus vaccines for people between the ages of 19 and 39 [were announced by WHO/PAHO], but the National Institute of Statistics, found more than five times that many Venezuelans (17.3 million) within that age range.[189]
Regarding food shortages, in April 2018, a representative of WFP told Human Rights Watch that WFP can only work in countries where a specific request by the government is in place, “which has not been the case with Venezuela.”[190] Even though David Beasley, WFP director, has said the situation in Venezuela is “catastrophic,” as of January 2019, WFP had no operations in the country because it lacks authorization from the Venezuelan government.[191]
At time of writing, FAO had not responded to an information request regarding its activities in Venezuela. In March 2018, José Graziano da Silva, FAO’s director, stated that hunger “continued to grow” in Venezuela in 2017.[192] On January 15, 2019, UNICEF, FAO, and the Venezuelan government signed an agreement to support a project to feed children in schools.[193] Even though FAO’s January – March 2019 “Early Warning Early Action report on food security and agriculture” report recognizes there has been a “dramatic increase in food insecurity” in Venezuela, it attributes it to an economic crisis and includes Venezuela in the list of countries and regions they consider “on watch.”[194]
In November 2018, the UN announced the first emergency funding for Venezuela under Maduro, a total of $9.2 million in health and nutrition assistance.[195] These funds have been allocated to UN agencies working on Venezuela, including UNICEF, UNFPA, WHO, UNCHCR, and International Organization on Migration.[196] No additional funds have been allocated to Venezuela by the Central Emergency Response Fund (CERF) since.[197]
In May 2018, CERF also provided $6.2 million in assistance to Venezuelan migrants in need of “life-saving assistance.”[198] The focus of this emergency relief is to “help the countries neighboring Venezuela deal with the consequences of large numbers of Venezuelans leaving the country.”[199]
Meanwhile, UN agencies have provided humanitarian assistance to Venezuelans outside of the country.
OCHA’s 2019 Global Humanitarian Overview report includes a Regional Refugee and Migrant Response Plan to address the flow of Venezuelans into neighboring Latin American and Caribbean countries.[200] This plan, in which 17 UN agencies, 14 non-governmental organizations, five donors, and two financial institutions participate, is geared towards addressing the needs of Venezuelans who have recently left the country.[201] WFP has provided assistance to more than 100,000 Venezuelans in Colombia and Ecuador.[202] At the Brazilian border with Venezuela, UNHCR has established 13 shelters that house more than 6,850 Venezuelans who receive shelter, medical care, and food.[203] The International Organization for Migration (IOM) is also active in the region.[204] In Ecuador, WFP and UNICEF contribute to a government initiative to provide food and blankets to Venezuelans.[205] The European Union has announced that it would provide €35 million in humanitarian and development assistance for Venezuelans in and outside of Venezuela.[206] Germany alone, since the beginning of the crisis, has provided €14.6 million to Venezuela’s neighboring countries via WFP and UNHCR.[207]
Non-governmental Groups
Human Rights Watch conducted more than a dozen confidential interviews with staff from international and Venezuelan organizations that attempted to provide humanitarian assistance in Venezuela.[208] They all reported difficulties when trying to establish operations in the country, and those who were able to start operations said they faced an array of government-imposed obstacles to provide assistance to Venezuela’s population in need. The obstacles include delays in official approvals for operations or for releasing aid supplies from customs; orders by higher-level hospital or government authorities to suspend implementation of ongoing aid initiatives; and limits on getting donated supplies into public hospitals.
Two doctors interviewed by Human Rights Watch also mentioned that hospital administrators had prohibited them from receiving donations, generally of baby formula or food, for patients.[209] In November 2018, the University Hospital in Caracas rejected a donation of medicines and medical supplies from the international humanitarian group, Doctors Without Borders.[210] A document that appears to be a press release signed by hospital authorities and circulated on social media says the medicines offered by Doctors Without Borders do not comply with local regulations, and that “Venezuela has enough resources to obtain all the medicines that the Venezuelan people need to reestablish their health, and is not susceptible to misery that undermines its dignity.”[211]
All the humanitarian workers interviewed by Human Rights Watch said that their agencies would be able to provide much more aid and support to Venezuelans in need if the government did not deny the crisis and instead sought additional help. Given the barriers the government has put up to their own work, these groups have been looking for local counterparts to implement their projects, putting greater strain on the work of already overstretched Venezuelan organizations.
Meanwhile, local Venezuelan organizations can obtain private donations of medicine or food in the country through door-to-door courier services, but they are expensive and only allow shipping small quantities of aid. For example, Acción Solidaria, a non-governmental group that has received donations from 17 countries since May 2016, has provided an increasing number of medicines to patients seeking aid—750 ARV doses for HIV and 3,217 for other conditions in 2016; 1,050 ARV treatments for HIV and 21,100 treatments for other conditions in 2017; and 1,300 ARV treatments and 19,000 for other conditions up until September 2018. However, the total number of people seeking aid at their offices has consistently increased from 250 to more than 1,500 a month between 2016 and 2018. Acción Solidaria has limited capacity to process requests for medication and has, on average, been able to cover only half of the needs it registers.[212]
The vast majority of humanitarian workers interviewed by Human Rights Watch said they did not want to be identified in this report, fearing they would not be able to continue working in the country if they did.
Other Offers of Aid
The International Federation of the Red Cross has more than doubled its budget to operate in Venezuela from five to 13 million dollars, according to an interview to a high Red Cross official published by an Argentine outlet.[213]
The Lima Group, composed of Canada and 13 Latin American governments, has repeatedly offered humanitarian aid to Venezuela.[214] Some of its member states—for example, Colombia and Brazil—did so separately as well. Canada is channeling aid through various UN agencies, and has contributed about $2.21 million total to the humanitarian needs resulting from the Venezuela crisis.[215] The United States has offered aid through its State Department and USAID agency.[216] And it announced another $48 million for the regional humanitarian crisis in September 2018, and an additional 20 million in January 2019.[217] The United Kingdom’s Department for International Development (DFID) allocated £6.5 million in February from its reserve to support humanitarian agencies across the region. Due to the “Maduro regime’s denial of a humanitarian crisis,” the UK opted not to disclose the organizations they are supporting.[218]
The European Union has been providing emergency aid to Venezuela since 2016, and, as noted above, recently announced it will contribute an additional €35 million in humanitarian and development assistance to Venezuela and the surrounding affected countries.[219] In the 2019 EU Humanitarian Aid budget, €13.5 million was allocated for humanitarian aid and food assistance in Central American nations, Colombia, and Venezuela.[220] In February 2019, 25 countries gathered at the OAS-hosted Conference on Humanitarian Assistance in Support of Venezuela pledged a total of $100 million.[221]
Several Latin American presidents have explicitly asked Maduro to accept help from their countries’ governments and from the international community by opening a “humanitarian channel” to receive aid.[222]
A September 2018 UN Human Rights Council resolution—adopted by 27 states worldwide including nine Latin American states—said the Venezuelan government should open its doors to humanitarian assistance to address “scarcity of food and medicine, the rise of malnutrition” and “the outbreak of diseases that had been previously eradicated or kept under control in South America.”[223]
In 2019, after the United States, Canada, the European Union, and some Latin American governments decided to send humanitarian aid to Venezuela’s borders, Venezuelan authorities refused to allow it into the country and used excessive force to disperse demonstrations supporting the opposition-led effort to bring aid into Venezuela.[224] Maduro stated that Venezuela was not a “country of beggars” and that the “humanitarian crisis does not exist.”[225] Diosdado Cabello, a powerful Chavista politician, claimed that the aid was a “military intervention” in disguise, while Delcy Rodríguez, vice president, stated that it was a way of getting “biological weapons” into the country. While Venezuelan authorities are within their rights to reject particular offers of assistance, doing so only heightens their responsibility to work towards alternatives that can fully address the urgency of the country’s needs. Efforts undertaken by Venezuelan authorities during Maduro’s presidency have failed to do so.
Acknowledgments
This report was researched and written by Shannon Doocy, associate professor at the Department of International Health at Johns Hopkins Bloomberg School of Public Health, Kathleen Page, M.D., associate professor of medicine at Johns Hopkins School of Medicine, and Tamara Taraciuk Broner, senior Americas researcher at Human Rights Watch. Diederik Lohman, former Health and Human Rights director at Human Rights Watch and current visiting global scholar at Drexel University's Dornsife School of Public Health, participated in conceptualizing this research project and reviewed several products that preceded and contributed to this report.
The report was edited and reviewed by Chris Beyrer, M.D., Desmond M. Tutu Professor of Public Health and Human Rights at Johns Hopkins Bloomberg School of Public Health and director of the Center for Public Health and Human Rights, and Paul B. Spiegel, M.D., professor of Johns Hopkins Bloomberg School of Public Health and director of the Johns Hopkins Center for Humanitarian Health.
It was also edited by Daniel Wilkinson, Americas managing director at Human Rights Watch; Dan Baum, senior researcher/editor; Margaret Knox, senior researcher/editor; Juan Pappier, Americas researcher; César Muñoz, Americas senior researcher; Joe Amon, clinical professor at the Department of Community Health and Prevention at Drexel University Dornsife School of Public Health; Joe Saunders, deputy program director; Chris Albin-Lackey, senior legal advisor; and José Miguel Vivanco, executive director of the Americas Division. Brian Root, senior quantitative analyst, reviewed the report and prepared the graphics. Human Rights Watch’s Americas Division associates Delphine Starr and Megan Monteleone contributed to the report production. Americas Division interns Hannah Smith and Angel Zapata provided valuable research support. The report was prepared for publication by Fitzroy Hepkins, administrative manager; and José Martinez, senior administration coordinator. It was translated into Spanish by Gabriela Haymes.
We would like to thank the generous support of the Desmond Tutu Professorship in Public Health and Human Rights at the Johns Hopkins Bloomberg School of Public Health.
We would also like to thank the numerous Venezuelan organizations, health professionals, and human rights defenders that contributed to this report, many of whom asked not to be identified.
Human Rights Watch is also deeply grateful to the Venezuelans who shared their testimonies with us after fleeing their country in search of medical treatment and food. Many of them expressed the hope that, by telling their stories, they could help prevent others from undergoing the same suffering that pushed them to leave home.