“We Are Also Dying of AIDS”
Barriers to HIV Services and Treatment for Persons with Disabilities in Zambia
Map of Zambia
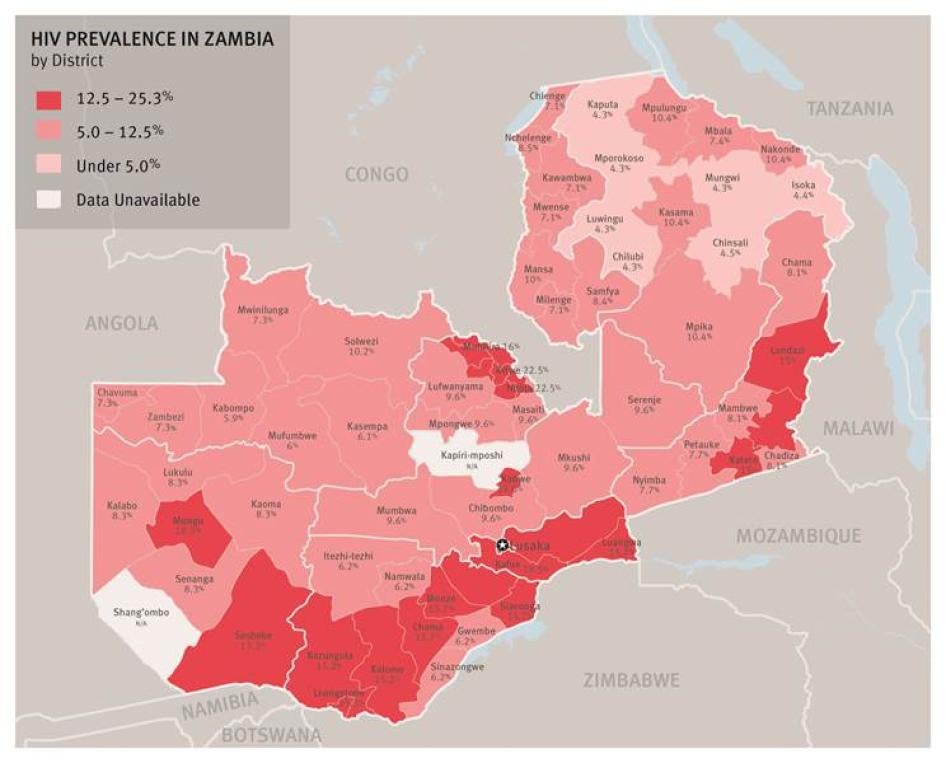
Human Rights Watch conducted field research in the highest prevalence districts in Southern, Copperbelt and Lusaka provinces. SOURCE: Zambia HIV/AIDS Epidemiological Projections Report 1985-2010 (Central Statistical office).
Glossary
|
Cerebral palsy |
An impairment of muscular function and weakness of the limbs caused by lack of oxygen to the brain immediately after birth, brain injury during birth, or a viral infection. Often accompanied by poor motor skills, it sometimes involves speech and learning difficulties.[1] |
|
Developmental disability |
An umbrella term that refers to any disability starting before the age of 22 and continuing indefinitely (i.e. that will likely be life-long).[2] It limits one or more major life activities such as self-care, language, learning, mobility, self-direction, independent living, or economic self-sufficiency.[3] While this includes intellectual disabilities such as Down syndrome, it also includes conditions that do not necessarily have a cognitive impairment component, such as cerebral palsy, autism, and epilepsy and other seizure disorders. Some developmental disabilities are purely physical, such as sensory impairments or congenital physical disabilities. It may also be the result of multiple disabilities. While autism is often conflated with learning disabilities, it is actually a developmental disability. |
|
Disabled persons’ organizations (DPOs) |
These are formal groups of people who are living with disabilities and who work to promote self-representation, participation, equality and integration of all people with disabilities. |
|
Intellectual disability |
An “intellectual disability” (such as Down Syndrome) is characterized by significant limitations both in intellectual functioning (reasoning, learning, problem solving) and in adaptive behavior, which covers a range of everyday social and practical skills. “Intellectual disability” forms a subset within the larger universe of “developmental disability,” but the boundaries are often blurred as many individuals fall into both categories to differing degrees and for different reasons. |
|
Psychosocial disability |
The preferred term to describe persons with mental health problems such as depression, bipolar disorder, and schizophrenia. Psychosocial disability relates to the interaction between psychological differences and social/cultural limits for behavior, as well as the stigma that society attaches to persons with mental impairments.[4] |
Summary
When you go for VCT [voluntary HIV counseling and testing], you are looked up and down, people say, “Why should you be in the line? Who could give you HIV?” They don’t expect disabled women to be sexually active.
—Yvone L., a Zambian woman with a physical disability, Lusaka,
November 2013
The problem is that deaf people have no detailed information on AIDS. We can go to the hospital but there is no sign language...The deaf do not know about adherence to medication and it can be a killer.
—Franklyn C., a Zambian man who is deaf and has received training to be a counselor for HIV testing and counseling, Kitwe, January 2014
There has been significant progress around the world in recent years toward providing universal access to HIV prevention, treatment, care and support programs. However, as the United Nations has acknowledged, such progress has excluded people with disabilities because of the lack of adequately targeted and accessible services for such persons.
The global epicenter of the HIV pandemic remains in eastern and southern Africa. Half of all new HIV infections occur in these regions annually, and they are home to 17 million people living with HIV. It is increasingly recognized that persons with disabilities are often more vulnerable to HIV infection than anyone else because of their lower education and literacy levels, higher poverty, and greater risks of physical and sexual violence.
Zambia has made important progress in scaling-up HIV prevention and treatment services over the past decade. However, more than 1 in 10 adults in Zambia are living with HIV, and 46 thousand adults and more than 9,000 children are infected with HIV every year. There are nearly two million persons with disabilities in Zambia, and like any other Zambian, they face a high risk of HIV infection. Yet, adults and children with disabilities have been systematically left behind in the national HIV response, with limited access to HIV prevention information and significant barriers to HIV testing and treatment.
This report examines the barriers faced by persons with physical, sensory, psychosocial and intellectual disabilities in accessing HIV services, including HIV prevention education and information, condoms, testing, treatment and long-term support for adherence. It also examines the exposure of persons with disabilities to significant risk factors for HIV.
We found that persons with disabilities face several key barriers to HIV services, and hence to realizing their right to the highest attainable standard of health. While some of these are the same for all people living with HIV, and not only for persons with disabilities, other barriers disproportionately limit or uniquely affect persons with disabilities. Key barriers include: 1) pervasive stigma and discrimination both in the community and by healthcare workers; 2) lack of access to inclusive HIV prevention education and information in schools, community settings, and through mass media; 3) obstacles to accessing voluntary testing and HIV treatment services; and 4) lack of appropriate support for adherence to antiretroviral treatment (ART).
1. Pervasive Stigma and Discrimination
In Zambia, disability is often considered a curse or punishment caused by evil spirits or as a result of witchcraft, for example in response to the actions of family members. Taboos regarding their sexuality result in a lack of respect for the sexual and reproductive rights of persons with disabilities. Individuals with different disabilities told Human Rights Watch that they are often viewed as being asexual and are confronted with negative attitudes about their right to marry and have children. As a result, persons with disabilities sometimes do not have access to HIV prevention, testing, or treatment services.
All persons living with HIV experience stigma and discrimination. However, persons with disabilities face “double” stigma because of their disabilities and HIV status, perpetuating their social isolation, hampering the linkage and adherence to treatment, and limiting their ability to form intimate relationships. This increased stigma further inhibits disclosure of their positive status in the community and even within their family and circle of peers.
2. Lack of Access to Inclusive HIV Prevention Education and Information
Children with disabilities are unable to access HIV prevention information on an equal basis with other children because of lack of access to education in general. Discrimination within the family, admission barriers and lack of physical accessibility keep many children with disabilities out of school where they might receive HIV prevention information. Even when children are able to attend school, children with disabilities are often excluded from programs providing HIV information, or cannot access inclusive materials.
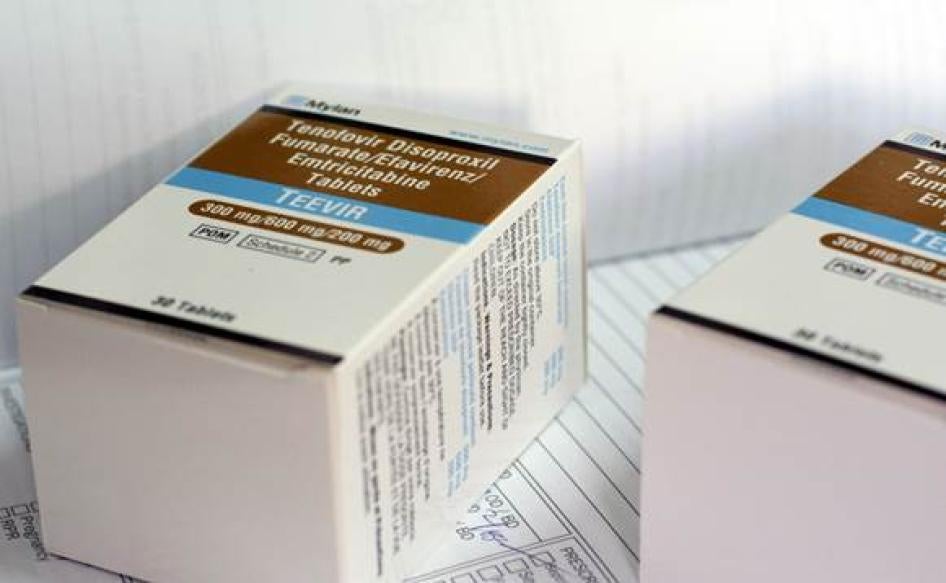
Antiretroviral drugs, like those pictured here, often do not have Braille symbols, making it difficult for blind people to identify various medications. © 2014 Justin Purefoy for Human Rights Watch
Similarly, adults with disabilities often cannot access general HIV information disseminated through print and mass media because of the lack of materials produced in simplified formats, braille, large print, or with sign language symbols. Persons with sensory or physical disabilities experience difficulties in accessing and using condoms due to the lack of accessible information and peer education. Community-based sensitization activities often exclude persons with disabilities due to physical and communication barriers and social isolation. Human Rights Watch found high rates of sexual and intimate partner violence among women and girls with disabilities, which increases their risk for HIV infection. The vulnerability of women and girls with disabilities is compounded because they lack equal access to information about gender-based violence, HIV prevention and social protection services.

Dominic Vwalya (left), who is blind and living with HIV, is accompanied here by a volunteer health worker to a local health center in Lusaka. © 2014 Justin Purefoy for Human Rights Watch
3. Barriers to Voluntary HIV Testing and HIV Treatment Services
Persons with disabilities told Human Rights Watch about the lack of effective pre- and post- HIV testing counseling because of inadequate training of healthcare workers on how to communicate with and address the concerns of people with disabilities. Persons with disabilities, in particular those who are deaf or blind, reported that healthcare workers do not adequately elicit personal health information, undertake diagnosis, prescribe medication, and counsel people with disabilities when they visit health facilities for antiretroviral treatment or in relation to opportunistic infections.
Persons with disabilities often experience a lack of confidentiality in HIV testing because of communication barriers and the need to involve a third person for interpretation. Representatives of the national organization of persons with psychosocial disabilities told Human Rights Watch that some individuals with psychosocial disabilities in mental health units in general hospitals are not ensured of their free and informed consent for HIV testing. Health workers and medical staff from three mental health units interviewed by Human Rights Watch reported varying application of HIV testing consent procedures in healthcare settings as well as confusion concerning the testing policy.
4. Lack of Appropriate Support for Treatment Adherence
Persons with disabilities who are receiving antiretroviral treatment often depend on the availability of a family member or friend for mobility or communication assistance to keep up with scheduled appointments. When this support is not available, however, accommodations are rarely made for their circumstances, such as re-scheduling appointments or providing a longer supply of medicine to individuals. Instead, healthcare workers label persons with disabilities as “defaulters,” requiring them to have more frequent appointments and limiting their supply of medicine as a consequence of missing an appointment.
* * *
These barriers deny persons with disabilities their right to health and other rights affected by one’s well-being, such as to work, to privacy and to freedom of movement. Zambia has ratified a number of international and regional human rights treaties including the Convention on the Rights of Persons with Disabilities (CRPD), which obligates governments to provide persons with disabilities the same range, quality and standard of free or affordable health care and programs as provided to other persons, including population-based public health programs. This means that persons with disabilities should be able to access HIV services on an equal basis with others.
In line with the CRPD, Zambia’s 2012 Persons with Disabilities Act directs the government to provide equal access to sexual and reproductive healthcare and public health programs. The 2012 draft Constitution guarantees persons with disabilities enjoyment of all the rights and freedoms in the Bill of Rights on the basis of accessibility and non-discrimination. In addition, the Zambian government has recognized persons with disabilities as a vulnerable population at risk for HIV; yet, it has not implemented specific interventions and strategies to provide inclusive HIV services for persons with disabilities.
International donors and United Nations agencies said that they were aware of the lack of inclusive and targeted HIV services for persons with disabilities in Zambia, and admitted that they had not done enough to ensure that funding for HIV services is allocated without discrimination and equitably benefits persons with disabilities who are just as if not more vulnerable to HIV.
The Zambian government should protect the fundamental rights of persons with disabilities by fully implementing the 2012 Persons with Disabilities Act. The African Union has called on member states to develop preventive and curative HIV services for the most vulnerable groups, including persons with disabilities. Zambia should take all appropriate steps to eliminate the pervasive stigma and discrimination persons with disabilities face in accessing HIV services and provide inclusive and targeted HIV prevention, testing and treatment services for persons with different disabilities.
As a regional leader in developing and expanding comprehensive HIV services, Zambia could become a model for inclusion of persons with disabilities. However, Zambia cannot achieve its goal of universal and equitable access to HIV prevention, treatment and care, if it leaves behind persons with disabilities in its national HIV response.
One of those being left behind is Daniel L., a shy but determined 13-year-old who is deaf and HIV-positive. He lost both his parents to HIV and has experienced stigma and neglect from his own family, who failed to enroll him in HIV treatment for some time, because they considered him to be doubly cursed and a burden. He told Human Rights Watch that he cannot talk to anyone about living with HIV and taking antiretroviral medicine as a deaf adolescent: “No one at the clinic or at home can sign with me. I can’t tell them [school friends] because I don’t want them to insult me.” Daniel becomes worried about his future but as he told Human Rights Watch, “I will fight to survive.”[5]
Key Recommendations
To the Government of Zambia and the National Assembly
To the National AIDS Council, Ministry of Gender and Child Development, Ministry of Community Development, Mother and Child Health, and the Ministry of Health
- Implement targeted disability-specific HIV services as well as ensure accessibility of existing mainstream HIV services to persons with different disabilities.
- Make hospitals and health centers accessible for persons with disabilities including through ramps, accessible examination and counseling rooms and toilets, and the availability of sign language interpreters.
- Develop a code of ethics for HIV testing, diagnosis and counseling services for persons with disabilities and provide training on it to health workers providing HIV services. Train all health workers on the rights of persons with disabilities, including their right to sexual and reproductive health.
- Ensure that HIV testing, treatment, care and support services adhere fully to ethical principles of confidentiality and the need for free and informed consent.
- Strengthen home-based care, peer services and mobile clinics for HIV service delivery to persons with disabilities.
- Ensure inclusive and targeted programs to prevent sexual violence against women and girls with disabilities and to provide treatment and support services for survivors.
To the Zambia Agency for Persons with Disabilities
- Develop and implement initiatives to combat stigma and discrimination against persons with disabilities in all areas of life, including in the area of public health.
To the Ministry of Community Development, Mother and Child Health, the Ministry of Health, and the Central Statistics Office
- Support research on HIV risk factors and prevalence among persons with disabilities, either through existing national surveys (such as the Demographic and Health Survey, Sexual Behavior Survey and Antenatal Care Surveillance Survey) or through targeted research. Ensure that the information can be disaggregated by type of disability, age and gender.
To UN Agencies, Donor Agencies working on HIV/AIDS, Donor Countries, and the Global Fund
- Assist the government of Zambia, through technical and financial support, with the design and implementation of inclusive HIV programming within each stage of the HIV continuum of prevention and care for persons with disabilities.
Methodology
Field research for this report was carried out in Zambia in November 2013 and January-February 2014 across the provinces of Lusaka, Southern and Copperbelt. These regions were selected because they are geographically diverse and they have the highest number of adults and children living with HIV in the country. Within each province, we focused on urban and peri-urban districts.
The report is based on 205 in-depth interviews with 64 individuals with disabilities, 15 parents of children with disabilities, 9 special education teachers as well as 117 nongovernmental organization (NGO) representatives, government officials, healthcare workers, and other individuals.
Of the 52 adults and 12 children with disabilities[6] interviewed, 27 had physical disabilities, 12 were deaf, 9 were blind or had low vision, 2 had intellectual disabilities, 11 had psychosocial disabilities and 3 had multiple disabilities. Of these, 29 self-reported as living with HIV. Of those who self-reported as HIV-positive, some reported a pre-existing disability while others acquired their disability as a result of HIV.
Interviews were facilitated by NGOs providing community health services to adults and children living with HIV as well as disabled people’s organizations (DPOs), organizations providing HIV services, and disability rights activists. Human Rights Watch also met with field staff from government bodies, namely the Zambia Agency for Persons with Disability (ZAPD) and the Ministry of Community Development, Mother and Child Health. Because of these referrals, we expect that the individuals we spoke with were more likely to be linked to HIV and general social services, compared to individuals with disabilities not known by these organizations.
Interviews covered a range of topics related to the experiences of persons with disabilities in accessing HIV prevention, testing services and treatment. Conducting interviews on HIV poses a number of methodological and ethical challenges. We took great care to interview adults and children in a friendly and sensitive manner, and ensured that the interview took place in a private setting. Interviews were conducted mainly at interviewees’ homes or at NGO premises in locations where the interviewee’s privacy was protected. Information about the HIV status of the adults and children interviewed was kept strictly confidential.
Before each interview, Human Rights Watch informed interviewees of its purpose, the kinds of issues that would be covered, and how the information would be used. We then asked if they wanted to participate. We informed them that they could discontinue the interview at any time or decline to answer any specific question, without consequence. Interviews with adults and children with disabilities and their families were carried out in English, Bemba, Nyanja, Lozi, Tonga and sign language with consecutive interpretation as needed.
Interviewees did not receive any material compensation. Unless otherwise noted, we have disguised the identities of all interviewees in this report to protect their privacy. The identities of a number of other interviewees including some government personnel have also been withheld at their request.
With permission from the Ministry of Community Development and Mother and Child Health, Human Rights Watch visited seven primary healthcare sites, two mobile clinics and five tertiary hospitals. We also visited two children’s homes for orphaned and vulnerable children affected by HIV, four government education facilities with special education units for children with disabilities, and two Victim Support Units (VSUs) at local police stations.
We conducted interviews with 41 healthcare workers including eight voluntary counselling and testing (VCT) and ART counselors, eight nurses, seven doctors, five clinical officers, two psychologists and five home healthcare workers. These interviews concerned their experiences in providing HIV services to persons with disabilities. We also sought their opinion on measures that could be taken to improve access to HIV services by persons with disabilities.
Human Rights Watch also interviewed 18 local and national government officials from the Ministry of Community Development, Mother and Child Health, Ministry of Education, Science, Vocational Training and Early Education, Ministry of Home Affairs, Ministry of Justice, the National HIV/AIDS/STI/TB Council and the Zambia Agency for Persons with Disabilities; and 33 representatives of local NGOs, organizations providing HIV services including faith-based organizations, international NGOs, and United Nations agencies.
Human Rights Watch consulted with international disability rights experts at various stages of the research and writing and reviewed a number of official documents from the Zambian government, as well as relevant reports from donors, UN agencies and NGOs.
In May 2014, Human Rights Watch presented preliminary findings to the Ministry of Health, the Ministry of Community Development, Mother and Child Health, the Ministry of Education, Science, Vocational Training and Early Education, the Ministry of Gender and Child Development, the Ministry of Justice, the Zambia Agency for Persons with Disabilities, and the National HIV/AIDS/STI/TB Council.
I. Background
HIV/AIDS Epidemic in Zambia [7]
Globally, approximately 35.3 million people are living with HIV.[8] Eastern and southern Africa remain the epicenter of the pandemic, with 48 percent of the world’s new HIV infections and 17.1 million of all those with HIV living in these regions.[9] Zambia has a generalized HIV epidemic—that is, an epidemic that affects all segments of society. In 2012, the prevalence of HIV in Zambia was about 12.7 percent within the 15 to 49 age group, with more than 700,000 adults and children estimated to be living with HIV.[10]
In 2004, the Zambian government introduced free access to antiretroviral therapy (ART) in the public health sector. In June 2005, the government declared the ART service package (including counseling, x-rays, and CD4 testing[11]) free of charge.[12]
Zambia has made significant investment and progress in scaling-up HIV prevention and treatment services over the past decade. The number of HIV counseling and testing sites has increased from 56 in 2001 to 1,800 in 2012[13] and the number of health facilities providing ART services (in both the private and public sectors) has increased from 107 in 2005 to 564 in 2013.[14] Between 2005 and 2013, the number of adults and children on ART increased from 57,164 to 580,118, representing an increase from 23.5 percent treatment coverage for those needing ART to 81.9 percent.[15]
However, the Zambian government has acknowledged that it faces a number of challenges in ensuring universal access and utilization of HIV services – including an “inadequate focus on vulnerable populations.” [16] In 2008, the Kampala Declaration, adopted by the African Campaign on Disability and HIV & AIDS, called on African governments to ensure that “National AIDS strategic plans recognize persons with disabilities as vulnerable to the impact of HIV and AIDS” and provide inclusive services. [17]
Zambia’s 2012 Persons with Disabilities Act mandates the government to “provide persons with disabilities with the same range, quality and standard of free or affordable health care as provided to other persons, including in the area of sexual and reproductive health and population based public health programmes.” [18] The draft 2012 National Disability Policy states that “people with disabilities have similar sexual desires as the non-disabled and are equally affected by the pandemic.” [19] Furthermore, the Zambian government recognized persons with disabilities as a “vulnerable population” in its third National AIDS Strategic Framework (NASF 2011-2015). [20]
Persons with Disabilities in Zambia
According to the World Health Organization (WHO), more than one billion people worldwide – 15 percent of the world’s population - live with physical, sensory (deafness, blindness), intellectual or psychosocial disabilities, or a combination of these.[21]
There is limited data on people with disabilities in Zambia, including how many adults and children are living with disabilities and their specific housing, education, and healthcare needs. There is wide disparity in the available statistics, from 2.0 percent in the 2010 National Census[22] to 13.3 percent, based on a 2006 national representative survey of living conditions among people with disabilities conducted by the Zambia Federation of Disability Organizations (ZAFOD), in collaboration with SINTEF Health Research and other partners.[23] WHO has previously estimated that 15.3 percent of the population in African countries has a significant or moderate disability.[24]
The 2010 census reported 251,427 persons with disabilities in Zambia, including 66,043 children and young people in the 5 to 19 year age group.[25] However, national educational data indicates that this number likely underestimates the number of people with disabilities. In comparison to the census data, the Ministry of Education reported that 198,394 children with special learning needs (comprising children with hearing, physical, intellectual, visual, specific learning and other disabilities) were enrolled in Grades 1-9 in basic schools in 2010.[26]
The prevalence of disability is likely higher than the government figures indicate due to social factors that isolate people with disabilities and the limitations in data collection. Because of fear and shame, and traditional beliefs that disability is associated with misfortune in the family caused by witchcraft,[27] many adults and children with disabilities remain hidden in their homes away from the public and may not be included in any data on persons with disabilities.
Furthermore, while the government expanded the number of disability categories in the 2010 census,[28] data on disability was collected through a dichotomous (yes/no) response to questions about the existence of a disability, rather than an approach that captured “variations in the intensity of the disabilities.”[29] Such an approach would likely understate the prevalence by capturing only the most severe forms of disability. Using the SINTEF estimate of 13.3 percent prevalence (based on capturing disability across a spectrum of degrees of severity), there would be approximately 1.9 million persons with disabilities in Zambia.[30]
There is no internationally accepted definition of disability. The 2006 Convention on the
Rights of Persons with Disabilities (CRPD), a landmark treaty so far ratified by 147 countries including Zambia, describes persons with disabilities as including those “who have long-term physical, mental, intellectual or sensory impairments which in interaction with various barriers may hinder their full and effective participation in society on an equal basis with others.”[31] Zambia’s Persons with Disabilities Act defines disability as a “permanent” impairment resulting from the interaction between health conditions and external contextual factors.[32] However, by requiring the existence of a “permanent” condition, it is narrower than the CRPD, which does not exclude temporal impairment in its scope.
According to Zambia’s 2010 Census, physical and sensory disabilities were the most common type of disability in the country, with 43.6 percent of persons with disabilities reporting some sensory impairment (partially sighted, blind, deaf, hard of hearing). A total of 32.7 percent had a physical disability, 6.8 percent reported a psychosocial disability, and 4.7 percent had an intellectual or learning disability.[33]
Vulnerability of Persons with Disabilities to HIV
Internationally, growing evidence indicates that people with disabilities have greater exposure to all of the risk factors[34] for HIV including lower education and literacy levels, poverty, and risk of physical and sexual violence, and hence may be disproportionately affected by HIV.[35] In Zambia the limited data on persons with disabilities also suggests that they are more vulnerable to the risk factors for HIV.[36]
Persons with disabilities in Zambia have limited access to education and a low level of literacy. The 2010 Census indicated a literacy rate of 58.6 percent among persons with disabilities in comparison to 70.4 percent for persons without disability.[37] According to the census, 34.4 percent of persons with disabilities had never attended school, in comparison to 20.9 percent of persons without disabilities.[38]
In Zambia and in many other countries, disability and poverty are inextricably linked.[39] Worldwide, as many as 50 percent of disabilities, are directly linked to poverty.[40] Poverty can lead to disability through malnourishment, lack of access to health services, poor sanitation, or unsafe living and working conditions.[41] In turn, having a disability can “entrap a person in poverty by limiting their access to education, employment, public services and even marriage.”[42] In Zambia, more than 60 percent of the population lives below the poverty line with more than 40 percent living in extreme poverty.[43] Persons with disabilities are disproportionately affected by poverty. In its survey on living conditions among people with disabilities in Zambia, SINTEF found that 57.2 percent of people with disabilities aged 15 years and over had never been employed.[44]
National data indicates that women in Zambia face multiple forms of discrimination and abuses including gender-based violence, adding another risk factor for HIV.[45] International research also indicates that women with disabilities are likely to be disproportionately affected by violence.[46] According to the 2004 Global Survey on HIV/AIDS and Disability, “individuals with disability are up to three times more likely to be victims of physical abuse, sexual abuse, and rape.”[47] A 2010 survey of children and young adults with disabilities found high levels of physical and sexual violence against children and young people with disabilities in Zambia.[48]
These risk factors indicate that persons with disabilities are likely to be more vulnerable to HIV infection. While there is little data on how people with disabilities are affected by HIV, emerging data from the region and internationally indicates that there is at least an equal, if not greater rate of HIV prevalence among people with disabilities.[49] In Zambia, preliminary studies also indicate that persons with disabilities are just as if not more vulnerable to HIV infection.[50]
II. Barriers to HIV Services and Poor Quality of Care
“I’m a human being who has feelings…People say how did you become positive? They should understand that HIV does not spare the disabled.”
—Dominic Vwalya, a blind pastor from Lusaka, November 2013
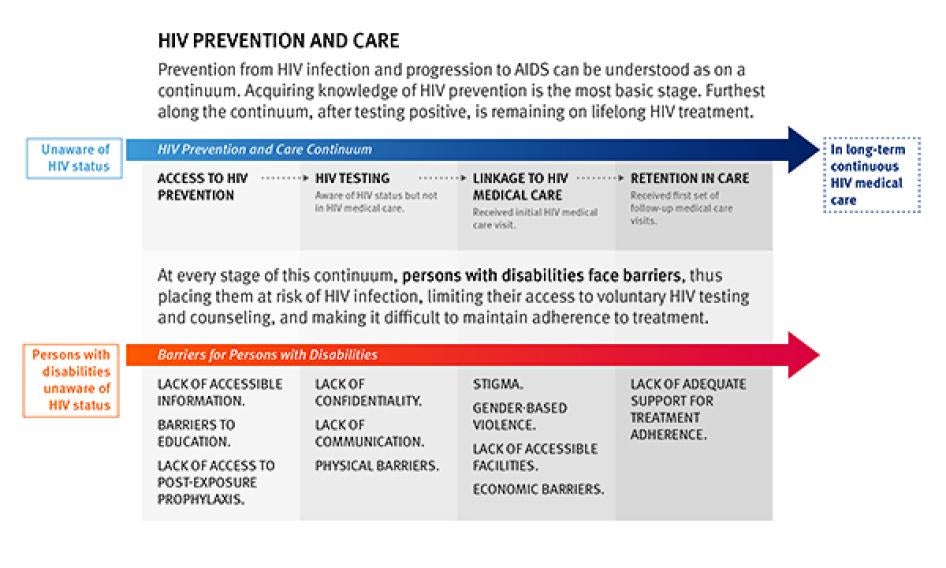
Prevention from HIV infection and progression to AIDS can be understood as on a continuum. At the most basic is acquiring knowledge of HIV prevention. Further along the continuum are such steps as being able to access HIV testing and then, if testing positive, gaining access to treatment and care, and being able to remain on lifelong treatment.
At every stage of this continuum, persons with disabilities face stigma, discrimination and communication and information barriers, thus placing them at a risk of HIV infection, limiting their access to voluntary HIV testing and counseling – which is a critical entry point for linkage to antiretroviral treatment and care – and making it difficult to maintain adherence to treatment.
Pervasive Stigma and Discrimination
Social Isolation in the Community
In Zambia, disability is often considered a curse or punishment caused by evil spirits or witchcraft, in response to the actions of family members. Carol A., the mother of a 14-year-old boy who has paralysis in his arms and legs due to meningitis, told Human Rights Watch that people in her community say things like, “Maybe the grandfather is sucking the child’s blood and selling it so he can add years to his life.”[51] People with disabilities told Human Rights Watch that community members also say a person acquired his or her disability because “they stepped on a charm,” or they have “been bewitched” by unseen spirits.[52]
Persons with different disabilities experience stigma and discrimination in different ways. Franklyn C., who is deaf, told Human Rights Watch: “In the community they see you using your hands and they think you are part human, part animal and don’t want to associate with you.”[53]
Persons with psychosocial disabilities and those living with epilepsy are often feared or viewed as being violent. Samson B., who is receiving treatment for psychosis, said: “Sometimes people say that they should not come near me because I am mentally disturbed and maybe I will throw stones at them.”[54]
Persons with disabilities are often called by denigrating and stigmatizing names. For example, individuals with psychosocial and intellectual disabilities are called “chibulu” (one who doesn’t understand), “wofunta” (mad) or “silu” (insane).[55] People with psychosocial disabilities are also called “a Chainama,” based on the name of the main psychiatric hospital in Zambia, the Chainama Hills Hospital.[56]
Patrick M., a 43-year-old man with a physical disability, described how social and physical isolation limit access to HIV information: “Health workers come from town and speak to a group of people gathered, but if you can’t go, you don’t get the information. You are cut from it. People with disabilities are left in the house.”[57]
Stereotypical views regarding the sexual and reproductive lives of people with disabilities also impede access to sexual and reproductive health and HIV prevention information. Susan M., a single mother with a physical disability, told Human Rights Watch: “People think that people with disabilities can’t have boyfriends, girlfriends...They can’t feel sex...They must be just staying at home as a disabled.”[58]
Inocente T., a man who is blind, told Human Rights Watch that some people in his community “believe that someone who has a disability should not indulge in sex. There is stigma…[but] we are human beings like any other person.”[59] Such views impede the ability of people with disabilities to access condoms. As Leonard C., a man with physical and visual disability explained: “We are too shy to go to the shops to get condoms…even to the clinic” because of the fear of what members of the community will say when people with disabilities are seen getting condoms.[60]
Patrick M., the 43-year-old man with a physical disability, said:
Sometimes people think that when you marry someone disabled, you will have children with the same disease. They think that you can’t do anything in society. Can’t get married. People in the community discouraged women from marrying me. People don’t like us. They think that disability will pass to our children. We will just have another problem...People are surprised that I have six children. They say ‘Wow, so these are your children?’ ”[61]

Human Rights Watch found that people with disabilities, like Jane Chalembwa (pictured here), the mother of three children, are often confronted with negative attitudes in Zambia about their right to marry and have children. © 2014 Justin Purefoy for Human Rights Watch
Stigma and Discrimination in Healthcare Settings
“We don’t counsel people with disabilities about HIV prevention, as there is no point.”
—James S., a home outreach volunteer for rehabilitation services, Livingstone, November 2013
Stigmatizing environments and attitudes within health facilities also create barriers for persons with disabilities and their caregivers in accessing health information, testing and treatment. The mother of a child with cerebral palsy and intellectual disability, told Human Rights Watch: “If we mothers have ‘too big’ children on our back, we get stares and negative comments from people at the clinic…Stigma barricades you and your child.”[62]
While most people interviewed by Human Rights Watch did not experience direct discrimination by healthcare workers, some health workers made assumptions about whether people with disabilities can understand health information or held mistaken beliefs about their vulnerability to HIV. Samson B., a man with a psychosocial disability, told Human Rights Watch: “I see that they think that because I’m mentally disturbed, there is no need [for the health workers] to talk to me about HIV.”[63]
While some people with disabilities rely on their caregivers and family members for HIV prevention information,[64] others do not feel they can access HIV information. Lusa Kabemba, a blind woman who provides services for women with visual disabilities told Human Rights Watch, “A lot of people in the compounds who don’t have the information I have would rather just die because of the stigma.”[65]
Many persons with disabilities interviewed told Human Rights Watch that they are often confronted by perceptions that they are asexual or do not have a right to full sexual and reproductive lives.[66] Yvone L., who has a physical disability and works with women with disabilities, said: “When you go for VCT [voluntary counseling and testing] you are looked up and down, people say, ‘Why should you be in the line? Who could give you HIV?’ They don’t expect disabled women to be sexually active.”[67]
In some cases, persons with disabilities said that health workers providing pre- and post-HIV test counseling could be helpful or in some cases harsh or hurtful to them. Philip M., who has a physical disability and is the father of six children, said: “When they find that a disabled person is affected [positive], some [nurses] will encourage that person, but some will use bad words, like: ‘You know the way you are and you start doing this? How are you going to live? You can’t work.’”[68] Michael C., a 30-year-old man with a physical disability told Human Rights Watch: “They say ‘Why should you get involved in sex if you are disabled. You don’t even feel sorry for yourself.’…But we have a right to have sex.”[69]
Women with disabilities also said that health workers expressed negative and stigmatizing attitudes toward pregnant women with disabilities. Yvone L. said, “If you go for pregnancy care, they counsel you publicly as if you have done something wrong and everyone is free to make comments…‘Why should you become pregnant?’ Everyone gets shocked.”[70]
Many persons with disabilities interviewed told Human Rights Watch about their preference for peer counselors at general health facilities or testing facilities for people with disabilities. Gordon K., a 26-year-old deaf man in Kitwe, explained: “Some of us deaf, we are afraid to even talk about it…Afraid to discuss topics of sex, HIV…so it is better with a deaf counselor.”[71] Candice L., a blind woman, told Human Rights Watch: “VCT is the starting point. It would be good to have our own VCT where we could test each other on our own, then we could refer to a clinic. We are being left out.”[72]
Double Stigma and Linkage to HIV Treatment & Adherence
After testing positive for HIV, individuals with disabilities face difficulty linking to ART because of stigma or fear of loss of confidentiality. The experience of stigma by persons with disabilities is not dissimilar to many people without disabilities who are living with HIV. However, persons with disabilities face compounded barriers because their fear of HIV-related stigma is heightened by lack of accessible HIV information and negative attitudes about their sexual and reproductive lives by health workers and people in the community.
For example, Bruce A., who has a physical disability and lives in a small farming community outside of Livingstone, told Human Rights Watch that he is scared to start ART and has not continued his follow-up appointments after receiving his positive HIV test because he fears that women in his community will be further discouraged from forming an intimate relationship with him: “The women’s families already tell them not to marry a cripple.”[73]
Persons with disabilities are also affected by internalized stigma, which impacts their linkage to treatment. Ruth L., an ART counselor in Ndola, told Human Rights Watch: “Some people with disabilities look down upon themselves, become withdrawn after VCT – they don’t want to follow-up for treatment.”[74] Lucy B., who is blind and recently finished secondary school, said: “Most of us with disability are not free to talk about our [HIV] condition…We are ashamed because we are seen as a double burden to society.”[75]
Jacob T., a 44-year-old deaf man, told Human Rights Watch about how he and his wife (who is also deaf) struggled to accept their positive status: “I was so ashamed in front of the doctor – I didn’t even know what it was to be HIV-positive – others will look down at you – for some time, we didn’t tell anybody except me and her…I was worried that I have made a mistake because I have been going with others – I kept that a secret to myself.”[76] He said that he and his wife experienced heightened fear of HIV-related stigma because of negative community attitudes about their right to a full sexual and reproductive life as a deaf couple.
Several persons with disabilities told Human Rights Watch that they preferred not to seek ART at their local or closest health facility providing ART because of their fear of stigma.[77] Matthew C. who has a physical disability, explained: “There is no privacy in the clinic – you can meet others from our community there and don’t want them to know your status…some of us would prefer to go for ART to a clinic far away.”[78] While this fear of HIV related stigma is not unique to persons with disabilities, many of them told us that they face a heightened concern for privacy because of the double stigma they face in the community - related to both their disability and HIV status.
HIV-related stigma also creates barriers for individuals with disabilities in adhering to treatment. Persons with disabilities are often reliant on relatives or others to take them to medical appointments or communicate information to them, and therefore have to tell them about their status, depriving them of confidentiality and risking a stigmatizing response.
According to the Persons With Disabilities Act 2012, the government (through the Zambia Agency for Persons with Disabilities) is obligated to “carry out programmes and conduct campaigns…to raise public awareness…to combat stereotypes, prejudices and harmful practices relating to people with disabilities in all areas of life.”[79] However, to date legislation has had little impact on the prevailing negative societal attitudes and effects of stigma on persons with disabilities.
Barriers to HIV Prevention Services
Lack of Access to Inclusive HIV Prevention Education in the Classroom
Schools play an important role in addressing the knowledge gap in HIV prevention among children and young people. In Zambia, HIV education in schools is predominantly provided through the “Life Skills Education Framework” and is integrated with the teaching of core curriculum subjects, rather than being delivered as a comprehensive, stand-alone unit.[80]
However, because of lack of effective access to education, children with disabilities are unable to access HIV prevention information on an equal basis with others. According to one study, children with disabilities are almost three times more likely to have never attended school in Zambia than children without disabilities in the same household.[81]
Stephen M., a deaf youth from a peri-urban area explained, “We have discrimination in our own homes...Hearing siblings come first...Even my father refused to pay [my] school fees but my brothers and sisters went to school.”[82] In some communities, children with disabilities are denied the chance to go to school. One rehabilitation home care worker told Human Rights Watch: “It’s a challenge for disabled children to go to school, especially those with intellectual disabilities...Disabled children are looked at as useless.”[83]

Child with physical disability in a special education facility in Ndola. © 2014 Rashmi Chopra/ Human Rights Watch
Yet even when children with disabilities are able to attend schools, they are often left out of instruction on HIV because of stereotypical perceptions of teachers that children with disabilities do not need to learn about HIV or due to the lack of appropriate materials. Anita C., a special education teacher for children with intellectual disabilities, explained, “We get no adapted materials...Once in a blue moon, we get HIV materials…If we have money, we buy some or make some...These children [with intellectual disabilities] are vulnerable – we need pictures and other materials to educate them.”[84] To date, the Life Skills learning materials are not available in braille, large print, sign-language symbols or simplified formats.[85]
Special education teachers and head teachers also told Human Rights Watch that while their schools provide peer-based extra-curricular HIV prevention education to students through programs such as “Anti-AIDS Clubs” or “Safe Love Clubs,” special education teachers are typically not involved in such initiatives and children with disabilities are often not encouraged to participate in these activities.[86] As one teacher for deaf students said: “Sexuality and HIV education is just for the hearing and their teachers.”[87] Of the 44 students with disabilities interviewed, only a few had participated in such clubs.[88] Special education teachers and students with disabilities are also typically excluded from special HIV prevention programming in schools.[89] For example, the “Delayed Sexual Debut” project involving training of peer youth educators and teacher champions across 13 schools in three districts in Zambia in 2012 did not include special education teachers or students attending special education units.[90]
Lack of Appropriate HIV Prevention Information
Persons with disabilities lack access to inclusive HIV information and communication, particularly persons with visual, hearing or intellectual disabilities. Few print materials are produced in braille, large print, or with sign language symbols.[91] Most organizations working on HIV prevention who spoke to Human Rights Watch said that small volumes of materials are produced in braille and sign language with limited dissemination for special events such as World AIDS Day.[92] George Mizinga, a blind man who runs an organization in Livingstone for persons with disabilities, told Human Rights Watch: “Some material is translated into braille in Lusaka but it rarely reaches here.”[93] Several DPOs and teachers told Human Rights Watch that available HIV materials in braille often contain outdated information.[94]
Deaf counselors and sign language interpreters told Human Rights Watch about the need to develop signs for technical terms associated with HIV and sexual and reproductive health and the need for standardization of sign language vocabulary.[95] Deaf people also raised their concerns about the compounded barriers faced by deaf people who are not literate. A deaf man explained: “They don’t consider the deaf who can’t read...Recently, there was a campaign on male circumcision but it didn’t get to the deaf.”[96]
DPOs representing different disabilities also told Human Rights Watch about the lack of materials in simplified language or visual formats for people with intellectual and learning disabilities and people with low literacy levels.
Many people whom we interviewed expressed a need for peer-to-peer communication and the importance of peer verification of information.[97] Jacob T., a 44-year-old deaf man, said, “I see posters and pamphlets but I learned about male circumcision at the deaf church…better to educate from deaf to deaf.”[98] One deaf counselor told Human Rights Watch, “Some [deaf] are afraid to even talk about it...afraid by subjects of sex, condoms... We teach each other about why AIDS comes.”[99] However, people with disabilities are rarely included in peer-based programming, and HIV counselors with disabilities receive little training and support on peer to peer counseling.[100]
While a few NGOs are actively working on inclusion of persons with disabilities in community-based sensitization activities, Human Rights Watch found that people with disabilities in many communities are excluded from activities involving theatre, mobile outreach and community meetings and clubs due to physical and communication barriers and isolation within the community. Rosemary T., a counselor who works with a community-based sexual and reproductive health program in five districts in the Copperbelt province, told Human Rights Watch: “Communication is a barrier to disabled people coming to the meetings...The youth in the districts asked for training in sign language because they were having trouble communicating with the deaf.”[101]
Despite their vulnerability to physical and sexual violence, Human Rights Watch found that women and girls with disabilities and their families are often excluded from community-based initiatives to prevent gender-based violence (GBV). Since the passage of The Anti-Gender-Based Violence Act in 2011, there has been an increase in community mobilization initiatives to raise awareness about prevention of and protection from gender-based violence.[102] However, most of these initiatives do not address persons with disabilities and parents of children with disabilities. Anti-GBV clubs formed by community members typically do not involve persons with disabilities in their leadership or membership and do not conduct inclusive activities for people with disabilities.[103]
Community workers and healthcare workers told Human Rights Watch that women and girls with disabilities who have been victims of sexual violence are also typically unable to access information about post-exposure prophylaxis (to reduce the risk of HIV infection) because of communication barriers and isolation from health and protection services. Information materials about the Anti-Gender-Based Violence Act, Victim Support Unit services at police stations, post-exposure prophylaxis and access to protection services are not provided in braille, large print, simplified formats or sign language.[104] The Anti-Gender-Based Violence Act contains limited provisions about equal access to services by people with disabilities. The National Guidelines for the Multidisciplinary Management of Survivors of Gender Based Violence in Zambia do not address treatment, care and support of women and children with disabilities.[105]
Sylvester Katontoka, an activist with a psychosocial disability, suggested that the government and organizations providing HIV services need to work more closely with DPOs to identify community leaders and outreach methods that can assist in mobilizing people with disabilities who are living in fear and isolation.[106]
Lack of Access to Condoms
People with sensory or physical disabilities told Human Rights Watch that they experience a number of challenges in accessing and using condoms, including the lack of accessible information and education.[107]
George Mizinga, who is blind, told Human Rights Watch of the need for education on condom use: “Condom use is difficult for the blind. It’s more difficult to teach a blind person to use a condom. They have to be able to touch - you can’t just show them and say do it like this.”[108] Dominic Vwalya, a 40-year-old blind man, said: “A blind person probably relies on their partner to help with using a condom. I can do it by feeling, but I’m not going to see whether it is damaged. The expiry date can be a problem. The one selling might give you the expired ones.”[109]
Michael C., a 30-year-old man with a physical disability, told Human Rights Watch that people with physical disabilities need specialized instructions on how to use condoms: “If one has weak limbs or a downward posture...no one is willing to give information on how to use them and it is difficult sometimes if you have to rely on the partner.”[110]
Several women with physical disabilities also said that they had trouble: “We want to access female condoms but we are too shy to move from where we are to the clinic.”[111] Most of the people with disabilities interviewed by Human Rights Watch said they preferred obtaining condoms from DPOs and other local community-based organizations providing services to persons with disabilities, rather than from clinics or shops. They also expressed the need for peer-based training on condom use.
FaithFaith, 25, became deaf when she contracted cerebral malaria at the age of 5. She attended a special school only for a few years, dropping out because her family could not afford the transportation costs and did not believe she would benefit from schooling. Faith did not learn formal sign language properly and cannot read. She now communicates through a mix of formal sign language and traditional signs that are understood and translated by her brother and mother with whom she lives. Faith found out she was HIV-positive in 2012 after giving birth to her daughter, who is also HIV-positive. Her husband verbally abuses her and is often absent. Faith did not know about HIV prevention until she tested positive. Sensitization meetings and workshops on HIV prevention in her local community are not conducted in sign language. She relies on her mother and brother to accompany her to appointments for antiretroviral treatment and to help her understand information provided by the clinic about antiretroviral treatment for her and her baby. They also help Faith care for her baby. There is no sign language interpreter at the clinic she visits. Faith does not like going to the clinic because people in the waiting area often stare at her when she is signing and make comments about how someone like her can be HIV-positive. One healthcare worker told Faith and her mother that someone like Faith should not be allowed to have any more children. |
Barriers to Voluntary HIV Counseling and Testing Services
Voluntary HIV counseling and testing is the entry point for critical linkages to care and treatment. In Zambia, HIV counseling and testing is either provided at voluntary HIV testing sites where individuals self-present for testing, or at the initiation of healthcare providers. In the latter case it is initiated as a routine offer of testing (such as to pregnant women in antenatal care to prevent mother-to-child transmission of HIV) or as a diagnostic service in clinical settings for patients who present with symptoms that could be attributed to HIV.[112] Despite progress, voluntary testing in the general population, at 24.3 percent (tested in past 12 months) has remained low due to a number of factors including HIV stigma and fear of social rejection, fear of rejection by family or intimate partner and concerns about antiretroviral treatment.[113]
Information and Communication Barriers
Persons with disabilities told Human Rights Watch about the lack of effective counseling services because of inadequate training of healthcare workers in how to communicate with and address the concerns of people with disabilities. Paul C., who has a psychosocial disability told Human Rights Watch: “VCT counselors need to be better trained...need to provide more than a test...not just about taking the test but about counseling that the result is not a death sentence.”[114]
Healthcare workers told Human Rights Watch about the lack of training and support provided to them in relation to people with psychosocial or intellectual disabilities.
Thomas L., a VCT counselor at a district clinic in Ndola, told Human Rights Watch:
We have some blind and deaf clients. Communication is a challenge. We don’t have anyone trained in sign language and have to write to communicate with the deaf. At the VCT, sometimes the deaf will come with someone to translate, sometimes we will refer them to the central hospital.[115]
Raymond L., a VCT counselor at a district clinic in Livingstone, explained the challenges they face in attending to persons with disabilities:
We have had people who are a bit slow, or with mental illness. It is hard to counsel someone who is mentally challenged. They are not getting it. They are not taking it seriously. We don’t get any training in that. Training would help. Sometime a person is violent when you want to prick them. It would be good to have workshops on people with disabilities.[116]
Felix B., a HIV counselor who provides testing and counseling services to pregnant women at a health center in Livingstone, told Human Rights Watch:
I can remember seeing a girl with a mental disability brought here by a neighbor. She had been raped. She was seven months pregnant when she came in. She was mentally ill...She had VCT. It was difficult to communicate with her. We communicated with her through the woman who brought her. She could understand what I was saying, but she was not responding, touching herself in strange ways, sucking her finger, scratching her head.[117]
According to Zambia’s National Guidelines for HIV Counseling and Testing, HIV testing services should comprise pre-test counseling (which includes providing information about the HIV test and responding to the client’s understanding of HIV/AIDS) and post-test counseling (which includes providing information about additional testing and positive living as well as making appropriate referrals and linkages to care and treatment services).[118] The Guidelines require that “counseling should always be adapted to the needs of the client.”[119] However, due to communication barriers and lack of training of HIV counselors, persons with different disabilities often do not have access to information and counseling on an equal basis with others.
Lack of Confidentiality in HIV Testing
Confidentiality of HIV test results is a cornerstone principle of medical ethics recognized as a best practice. Individuals with disabilities, however, often experience a lack of confidentiality because of communication barriers and the need to involve a third person for interpretation.
Chipo Tembo, a deaf woman who went alone for her first HIV test, told Human Rights Watch: “They [the clinic] didn’t have any sign language. They did a test and asked me to come back. I came back with my mother, but I would have preferred her not to find out then.”[120]
Many deaf people interviewed by Human Rights Watch shared their concern for lack of confidentiality by the sign language interpreter present during the testing and counseling session. Mackenzie Mbewe, a deaf man, told Human Rights Watch: “When you go with an interpreter, there is no confidentiality. They [the interpreters] can’t keep secrets…That is why we want nurses and doctors to be trained to interpret because they have ethics. Ethics training for interpreters would also be a good idea.”[121]
Lidia A., a deaf woman from Kitwe told Human Rights Watch about how confidentiality can also be breached by family members of friends: “Even if the interpreter is a friend of a family member, information spreads quickly...If it’s the wife, the husband will know quickly.”[122] In a few instances, deaf people told Human Rights Watch of their preference to access HIV testing facilities outside of their local communities because they are afraid that their status will be disclosed to community members by a known sign language interpreter.[123]
Zambia’s National Guidelines for HIV Counseling and Testing require that “it is essential that confidentiality be maintained when conducting HIV testing of any type.”[124]
Concerns about Free and Informed Consent in HIV Testing
HIV testing without consent, like violations of confidentiality, is contrary to medical ethics and best practices.
Representatives of MHUNZA, the Mental Health Users Network of Zambia, the national DPO of persons with psychosocial disabilities, told Human Rights Watch, that some people with psychosocial disabilities attending psychiatric units in general hospitals as in-patients are not ensured of full and informed consent for HIV testing.[125] Psychiatric clinical officers and medical staff from three psychiatric units interviewed by Human Rights Watch reported varying application of HIV testing consent procedures in the healthcare setting as well as confusion concerning the testing policy.[126]
The Guidelines distinguish between voluntary HIV testing, where the “client/patient has to actively and freely choose to take an HIV test, for example visiting a VCT centre” and routine or provider-initiated testing and counseling (PITC) or diagnostic counseling and testing (DCT), where the testing is conducted on the basis of “opt out screening.”[127] In the latter context, “the test is automatically performed unless the individual concerned raises an objection and opts out.”[128]
Medical staff from two psychiatric units told Human Rights Watch that they inform patients that the HIV test is being performed as part of other diagnostic tests and refer them for further pre-test counseling if they refuse or are uncomfortable with the testing.[129]
In the third psychiatric unit, healthcare workers told Human Rights Watch about differing testing practices and confusion about the government’s testing policy in health settings. A psychologist at the psychiatric unit told Human Rights Watch of the practice of testing for treatment purposes and disclosing the result to the patient only if they have accepted voluntary testing:
It is mandatory to run tests including HIV tests. There is a Ministry of Health policy that distinguishes between diagnostic testing and VCT. You can do diagnostic testing if you need to know a patient’s status for their treatment. They say that when you agree to be admitted, you agree that they can draw blood. You do baseline tests, including HIV...but the policy is not clear and nobody checks how it is applied. If we test someone and find out that they are positive, and have a low CD4 count, we will talk to them and try to get them to do VCT. … If we know that a patient is positive, we would try to get them to do VCT before they are discharged, but if they will not consent, we don’t tell them. So many people are positive and it influences all their other conditions, so we need to know their status to treat them better – you could be dealing with an OI [opportunistic infection] and not know.[130]
A clinical psychiatric officer at the same hospital told Human Rights Watch:
There is mandatory HIV testing when the patients come. If they are positive, they need to know so that they know which medications to start with. Else we’re killing them. We counsel them – can we examine, test and tell them? But we already know. HIV mimics a lot of other psychiatric disorders, that’s why we have to look for HIV.[131]
Another clinical psychiatric officer told Human Rights Watch about the need for routine HIV testing in mental health units: “If we suspect that an acute patient might be positive, we ask for an HIV test...drug reactions are one of the reasons why we test people for HIV when they are admitted. Carbamazepine interacts with ARVs and can cause drug resistance because it causes the ARVs to be cleared from the blood faster.”[132]
Staff from all three psychiatric units expressed the need for more training on ethical standards and application of the testing policy, and may be using terms such as ‘mandatory’ or ‘routine’ in imprecise ways to describe current practices. Staff said that applying HIV testing policies was especially difficult for patients considered to be in an “acute condition.”
The Guidelines provide that while both voluntary and routine HIV tests require a person’s full written or verbal consent, testing can be done without explicit consent in a number of circumstances including where “patients [are] unable to give consent (unconscious, mentally impaired) in whom HIV testing is deemed essential for management and no next of kin is available.”[133]
Free and informed consent is critical in the provision of HIV services. Exceptions to this requirement under Zambian guidelines, such as on the grounds of mental impairment, are not compliant with articles 12 and 25 of the Convention on the Rights of Persons with Disabilities.[134] The pending 2014 Mental Health Bill provides for “supported decision making” for persons with disabilities as required for implementation of the right to exercise legal capacity, in line with article 12 of the CRPD.[135] The CRPD obligates governments to ensure free and informed consent in medical care and treatment including through training and promulgation of ethical standards for public and private health care.[136]
Barriers to Treatment, Care, and Support
Barriers to Treatment Adherence
A high level of adherence is crucial for the success of antiretroviral therapy (ART). According to the World Health Organization (WHO), “adherence to ART is well-recognized as an essential component of individual and programmatic treatment success.”[137]The World Health Organization found that “higher levels of drug adherence are associated with improved virological, immunological and clinical outcomes and that adherence rates exceeding 95 percent are necessary in order to maximize the benefits of ART.”[138]Lack of adherence can lead to the development of drug resistance, illness, or death.
The lack of “treatment literacy” or counseling for individuals with disabilities creates significant barriers in adhering to treatment.
Many of the people with disabilities interviewed by Human Rights Watch, in particular deaf and blind people, reported that healthcare workers do not adequately elicit personal health information, diagnose, and prescribe medication and counsel people with disabilities when they visit health facilities for scheduled appointments for ART or in relation to opportunistic infections. Several deaf people on ART told Human Rights Watch about the lack of information exchange about their condition during their initial and follow-up appointments due to communication barriers including the lack of sign language interpretation.
One deaf ART patient in Lusaka told Human Rights:
“We communicate by writing a little...She [the counselor] doesn’t ask me anything - just counts my tablets and points to how many I take.”[139]
Chipo Tembo, a deaf woman, also explained:
“I write and they write…we use the broken English of my deaf culture. It is very difficult because sometimes I try to explain why I feel ill, but I’m not sure they understand me and give me the right medicine to take.”[140]
Another deaf patient on ART told Human Rights Watch about the lack of counseling on the importance of adherence:
“The doctor doesn’t teach how to take them…they just do the basics...He just says to take this medicine and come back and get some more without giving any other information like why not to skip the medication.”[141]
Sometimes, interpretation is available at hospitals, however. For example, Noreen C. who takes her deaf 14-year-old nephew to the health clinic for his ART appointments in Kitwe, explained: “We have limited capacity to talk to Samuel because we don’t sign. When I asked the doctors to tell him the effects of stopping taking his medicine, they brought a sign language interpreter.” Yet “usually they don’t have one,” Noreen C. said. “We worry if he will get the support he needs without someone to sign with him.”[142]
Dominic Vwalya., who is blind, told Human Rights Watch that blind people become more anxious about ART because they do not get accessible information about antiretroviral drugs and side effects from the counselors:
There are instructions attached to the medicine inside the box. How was I going to read to know the instructions? Or what if there was no one at home to read English? The instructions say: There might be reactions, you might feel a rash, headaches, constipation, abnormal urine, you must take much water. I had to ask another one who is taking the same medicine about these things.[143]
Many people with psychosocial disabilities told Human Rights Watch about their anxiety due to the lack of information given to them about the interaction and effects of taking ARV and psychotropic drugs. Gabriel L., a 38-year-old man from Lusaka, said he cannot access ART and mental health treatment at the same location and that he is not provided information about the combined burden of the two drug regimens by his ART counselor or by the clinical officer prescribing psychotropic drugs.[144] He told Human Rights Watch: “We have patient rights to information...about HIV and psychotropic medicines...but we are not told about this by anyone, about the dosage and interaction...These are very strong drugs...We must know about it.”[145]
Several persons with disabilities told Human Rights Watch that they wanted information about taking psychotropic drugs in addition to ARV medicine, but were scared to tell their ART counselor about their psychosocial disability (and disclose they were on psychotropic medication) because of their fear of being stigmatized as a “mad” person.[146] While in some locations mobile health clinics are being piloted at health care sites providing ART, integration of HIV services with mental health service provision remains low.[147]
The Persons with Disabilities Act obligates the government to ensure that health professionals “provide care of the same quality to people with disabilities as to others”[148]; to provide “systems to avail appropriate facilities and personnel to local health institutions for the benefit of people with disabilities;”[149] and “include the study of disability and disability related issues in the curriculum of training institutions for health professionals.”[150] Many healthcare workers providing HIV services interviewed by Human Rights Watch expressed the need for training on how to address communication challenges and provide psychosocial support to persons with disabilities.
Lack of Appropriate Adherence Monitoring
Strict adherence to ART is supported by ongoing monitoring of how a patient is maintaining the prescribed medicine regimen, which can be influenced by social and clinical factors. ART counselors assess adherence at regular intervals when patients attend scheduled appointments to collect a prescribed supply of medicine.
More than half of the persons with disabilities interviewed who disclosed that they were enrolled in ART told Human Rights Watch that they sometimes experience difficulty in keeping scheduled appointments due to the lack of availability of a family member or friend who can act as a guide for the blind, provide mobility assistance to persons with physical disabilities or communication assistance to deaf people or persons with intellectual disabilities.
The majority of persons with disabilities interviewed who were enrolled in ART, told Human Rights Watch that no accommodation is made for their circumstances, such as appointment re-scheduling or providing a longer supply of medicine on an individualized basis. Instead, individuals with disabilities were often told they had “defaulted” and were given a shorter supply of medicine as a consequence of missing an appointment.[151]
Dominic Vwalya., who is blind, said:
If you miss an appointment, they [ART counselors] become suspicious that you are not taking medicines. I need a guide to get to an appointment – this is difficult. When there were some bad times, I couldn’t go on the actual date. Since I missed an appointment, they put me on a two-week supply which was a challenge – as I need to take my nephew or niece (who are at school) to go with me to the appointment...They need to be pulled out of school to come with me.[152]
Persons with disabilities told Human Rights Watch that they feel stigmatized by being labeled as a “defaulter” by healthcare workers and are burdened with increased transportation costs and difficulties in arranging mobility or other assistance when they are required to attend appointments more frequently.[153]
Candice L., who is also blind, told Human Rights Watch:
One time, my children were doing year 9 exams so they couldn’t accompany me. I had medicine for that day and another day. I didn’t go that day. The counselor said: “You are a defaulter so you have to come back to the clinic in one week.” I usually get a three-month supply of ART, [but] I was given supply of only one week. I didn’t like being called a “defaulter.” I had done nothing wrong. So I refused and went to another clinic.[154]
In a few instances, persons with visual and physical disabilities and healthcare workers told Human Rights Watch that these circumstances were anticipated and resolved as a result of mobile and home outreach services.[155] However, most people with disabilities interviewed told Human Rights Watch they did not have access to these services.[156]
ART counselors told Human Rights Watch that they find it more difficult to adapt adherence management protocols for people with disabilities due to communication barriers and concerns about lack of follow-up alternatives, especially where there are no mobile or outreach services available. Ruth L., an ART counselor in Ndola told Human Rights Watch:
You have to counsel patients if you are giving them a lot [supply of medicines]. Usually you want to monitor side effects but sometimes there are reasons to give an even longer supply. But we worry that if we give too many medicines to someone far away, they may sell it...We also want to check CD4 and viral load.[157]
According to the national ART protocols on adherence management, a defaulter status is recognized “when a person who has been located as late or lost to follow-up chooses not to return to care.”[158] However, healthcare workers and persons with disabilities enrolled on ART told Human Rights Watch about the use of the term in connection with patients who had missed appointments but were still linked to care. The protocols also provide guidance on tracking and follow-up of patients who miss appointments including SMS messaging, home visits and contact with community workers.[159]
The Convention on the Rights of Persons with Disabilities obligates governments to develop universally designed services “which should require the minimum possible adaptation and the least cost to meet the specific needs of a person with disabilities” and “to promote universal design in the development of standards and guidelines.”[160]ART protocols and guidelines should be designed to ensure that they address the needs of people with physical, sensory, intellectual and psychosocial disabilities.
Lack of Adequate Adherence and Positive Living Support
“People with disabilities are often the most challenged because they are without a support network.”[161]
—Dr. David M., ART doctor in a health center in Lusaka, November 2014
According to the World Health Organization, “Adherence to ART may also be challenging in the absence of supportive environments” and “informing and encouraging people receiving ART and their families and peers are essential components of chronic HIV care.”[162] Studies show that there is an association between peer support and high rates of adherence and retention.[163]
Many persons with disabilities and health workers told Human Rights Watch that social isolation, stigma and a culture of secrecy about HIV inhibits disclosure of positive status within the family and in the community and hence limits opportunities for support. The sister of a young woman with an intellectual disability told us: “She cannot come out...She thinks it taboo to say I slept with someone and got it...It becomes something heavy in our culture.”[164]
She also told Human Rights Watch that her sister told her that she feared disclosure because a number of people in their local community believe she should not be leading a full sexual and reproductive life.
Persons with disabilities face heightened barriers to disclosure because of the lack of accessible information on living with HIV and lack of accessible and inclusive positive living support programs, including peer support programs. Philip M., who has a physical disability, told Human Rights Watch: “I know there are some people who are on ART in my community but it is hard for them to talk about it...We cannot talk about it...It is a secret.”[165]
Candice L., who is blind, explained the importance of support structures:
How do you know what time to take your drugs? Some people have talking watches or listen to the radio, or they rely on relatives at home. Sometimes we need encouragement. That is why it is good to open up. My children tell me when it’s time for me to take my ART. People without support miss their treatment, so it is very important to be open in family and community...The able-bodied, they came out together but for us, it is very difficult.[166]

A health worker dispenses antiretroviral medications at Chreso Ministries VCT (Voluntary Counseling & Testing) and ART (Antiretroviral Treatment) Centre in Lusaka. 2014 Justin Purefoy for Human Rights Watch
Particular Challenges Facing Children and Young People with Disabilities
Several children and adults with sensory disabilities and their caregivers in Lusaka and Kitwe told Human Rights Watch about the impact of parents and guardians not disclosing to them that they are in fact taking ARV drugs.[167]
Lucy B., an 18-year-old who is blind and has been raised by her aunt and uncle after her parents passed away, told Human Rights Watch:
I was born positive but I did not know my status and found out on my own at age 10. I was taking the pills for some time. My aunt and uncle said the medicine was for meningitis and they said to take the medicine every day as it is good for the health. I felt bad...guilty and disappointed when I found out. I kept it to myself but I became frustrated and angry whenever anyone mentioned HIV. I only told them that I knew when I was 14. I found out the medicines don’t cure. I became so angry I stopped taking them. Now I am on the second line. I understand I have something worse in my body than being blind – so I have to push on.[168]
Pastor Tembo who works within the deaf community told Human Rights Watch: “Deaf children don’t know what they have and why they are taking medicine. They ask the teachers.”[169] Noreen C., who knows very limited sign language and has been taking care of her 14-year-old deaf nephew since his mother passed away, attempted to explain to him only recently about the medicines he has been taking since age 7.[170] She told Human Rights Watch, “He needs to know why he takes the medicines. It is very hard for us. It would be better if there was information and support for talking about HIV and ART. We need someone who can communicate with him about these things.”[171]
Lack of disclosure about HIV treatment to children living with HIV is not unique to children with disabilities.[172] However, children with disabilities lack access to inclusive youth peer based adherence support. Caregivers of children with disabilities also lack access to accessible age sensitive information on ART for children with disabilities as well as adequate support structures for themselves.[173]
Most children and young adults with disabilities interviewed had not participated in support groups that provide youth peer support for positive living. While the government has long supported the establishment of “youth-friendly corners” (YFC) in health facilities, with the aim of delivering a standard package of health services including voluntary HIV testing, peer counseling and outreach activities, these have not expanded beyond pilot stage due to resource constraints.[174] In its Adolescent Health Strategic Plan 2011-2015, the government acknowledged that “One major weakness is that the YFC package of services does not include specific services for the disabled adolescents.”[175]
The government has stated a renewed focus on establishing a comprehensive package of adolescent-friendly health services (ADFHS) across all communities and health facilities. While it has recognized the need for these services to be accessible by adolescents with disabilities, it has not articulated any specific strategies for inclusion of adolescents with different disabilities.[176]
HIV and Nutrition“Some days I just take tea and bread – I can’t even get nshima (maize porridge)...Now I am begging for food from my relatives and the church since I can’t get any work. If I don’t eat, I don’t take the [HIV] medicine.” Jacob T., a deaf man from Lusaka who is enrolled in ART, February 2014. More than a third of the persons with disabilities enrolled in ART Human Rights Watch interviewed said lack of food was a major obstacle in maintaining adherence of their antiretroviral treatment. Sixty percent of all Zambians live below the poverty line and 42 percent live in extreme poverty, below the food poverty line. [177] Studies indicate that persons with disabilities are more likely to live below the poverty line because of their lack of education and employment. [178] Erica M., who is deaf and living with HIV has been sexually abused and abandoned by the two fathers of her children, she has no income support. She told Human Rights Watch: “Often from morning to night there is no food. We will starve without any help. I am now trying to give the baby solid foods but there is no food to feed the child.” [179] DPOs and persons with sensory disabilities also reported the lack of education and communication in braille, sign language and simplified formats about local sources of nutritious food and healthy eating. [180] The Joint United Nations Programme on HIV/AIDS (UNAIDS) has emphasized the importance of food security and nutrition because “lack of food and poor nutritional status may hasten progression to AIDS related illnesses and undermine adherence and response to antiretroviral therapy.” [181] |
III. Vulnerability of Children and Women with Disabilities
Neglect of Children with Disabilities and Impact on HIV Treatment
There are about 670,000 children orphaned by AIDS in Zambia – children who have lost their mother, father, or both (double orphans).[182] A significant number of these orphans are themselves HIV-positive. AIDS orphans are particularly vulnerable to abandonment and neglect.[183] While there is no data collected about children with disabilities who are also orphaned by AIDS, Human Rights documented instances of neglect in providing medical care to orphan children with disabilities who are HIV-positive.
Health workers, teachers and community workers told Human Rights Watch that caregivers of children with disabilities who are HIV-positive have to take on the responsibility of supporting the child with access to rehabilitation or other required services, adherence to HIV treatment, taking the child for regular monitoring appointments and ensuring they have sufficient nutritious food. A home outreach volunteer told Human Rights that people in the community or in the child’s family say: ”This child is cursed again and again...he won’t reach far...will die on the way.”[184]
In some cases, the caregiver does not believe limited resources should be spent on children with disabilities or is unwilling to acknowledge that the child is HIV-positive. This was the case with Emanuel B., a 12-year-old boy who has an intellectual disability, living in Lusaka.[185] He lived with his grandfather and older sister after his mother passed away. Despite his sister’s efforts in trying to ensure that he kept his healthcare appointments, Emanuel’s grandfather abused him verbally and kept throwing away his ARV medicine, because he did not believe Emanuel deserved any support or care, referring to him as “worthless.” Two years ago, Emanuel’s health deteriorated so much that he was brought to a hospice for children and later to an orphanage for children affected by HIV, where he now lives. Emanuel is now fully supported in his medical, educational, and nutritional needs and understands that he is on ART, although he sometimes becomes depressed about his family.[186]
A pastor who runs a school for deaf children in Lusaka told Human Rights Watch about Daniel L., a 13-year-old boy whose HIV treatment was delayed by his aunt who has been looking after him since his parents passed away.[187] The teachers at the school noted that Daniel was unwell and had puss on his body, when he started attending school at the age of 8. They found that Daniel’s aunt had taken him for HIV testing and had been advised to start him on treatment as soon as possible. However, his aunt delayed follow-up and initiation of treatment due to concerns about the increased cost of caring for Peter whom she already considered a burden because of his disability.[188]
Nandi Banda is a blind secondary school student who lost her mother to HIV and is under the care of her grandparents because she was abandoned by her father. Nandi told Human Rights Watch: “[My father] doesn’t like me because I am blind and [HIV] positive. He has not registered me for anything – bank account, passport...I don’t have a legal identity. I feel like I am living like an alien. He sees me as a useless thing. I am now fighting the battle of my life to be accepted. If something happened to my grandparents, what would I do?”[189]
Vulnerability of Women and Girls with Disabilities to Sexual Violence
Human Rights Watch found that sexual violence is a significant risk factor for HIV infection for women and girls with disabilities in Zambia. According to the 2007 Zambia Demographic and Health Survey, 47 percent of all women in Zambia experienced physical violence and 20 percent experienced sexual violence sometime in their lives.[190] In the majority of cases, violence against women was perpetrated by current or former intimate partners.[191] Victim Support Units and health providers throughout the country have also recorded increasing rates of child sexual abuse.[192]
No national data exists in Zambia on violence against people with disabilities. Women and girls with disabilities would appear to be at greater risk of being victims of gender-based violence as a result of their isolation, limitations in physical mobility, communication barriers, and lack of support structures.
Janet K., a blind woman from Lusaka told Human Rights Watch, “If you go around town, you find blind women sexually abused for a few kwacha (Zambian currency). Harassment is very high.”[193] Margret M., who lives with a physical disability in Livingstone, told Human Rights Watch, “In the villages and compounds they think that disabled ladies are HIV-free, so sometimes there is rape. They think, she’s always home; she’s HIV-free.” Margret also described how some women with disabilities who were poor faced difficult choices and had limited opportunity to negotiate safer sex. “They take money, even though they know that [the man] is HIV affected. They say: ‘I love you, I’ll look after you.’ Do you think that she can refuse to have sex? Especially someone who is in a wheelchair? They come with money. She can’t refuse. She doesn’t have a chance to say, ‘Let’s go for an HIV test.’[194]
About a third of the women with disabilities interviewed told Human Rights Watch that they had been victims of intimate partner sexual and physical violence. Malala C., a 36-year-old woman with a physical disability from Livingstone, told Human Rights Watch that her husband physically abused her:
He receives comments from people asking him why he’s married to a disabled woman...He beats me, one day he wanted to chop off my legs with a knife and he continued to say that I haven’t even paid a dowry so I can move out [of the home]. I went to the police who educated him but placed no charges. He has worsened, drinking a lot. If I could find something to do I would leave but I’m dependent on him.[195]
Health workers and family members told Human Rights Watch that women with disabilities are frequently abandoned by their partners.[196] Sarah L., whose daughter is deaf and HIV-positive with three children told Human Rights Watch: “Men come and give her babies...and they leave her.”[197]
Human Rights Watch found that women with disabilities feel that they are less able to negotiate safe sex practices, including the use of condoms. Brenda T., who has a visual disability and is HIV-positive, told Human Rights Watch that her husband pressured her to have sex without condoms:
He said, “You are married to me...you are my wife, my traditional wife – no way [we] can use condoms.” He was positive and sick but he never disclosed to me. He knew about condoms and HIV but because I am disabled, he wanted to use me – so I could be dumped away. He just wanted to use me. He said: “It is embarrassing to stay with a partially sighted woman and if you become completely blind...I can’t take [you] to friends.” I stayed with him because we were in a traditional marriage. When I found out I was positive, I felt very bad about why my husband kept using me even though he was positive. If he had used condoms, I wouldn’t be sick [HIV-positive].[198]
Human Rights Watch found that instances of sexual violence against girls and women with disabilities are often not reported because of a number of factors: concerns about stigma and being ostracized in the community, because the violence is perpetrated by a caregiver or family member, or due to pressure from the perpetrator to accept material compensation to keep it hidden. Betty L., a Victim Support Unit officer, explained: “There are a high number of unreported cases...people with disabilities feel rejected in society. They feel if they report they won’t be listened to...some don’t have anyone to speak for them.”[199] Erica M., a deaf woman who was sexually abused by a man known to her family, told Human Rights Watch: “I didn’t tell anyone...I kept it to myself because he said take money to buy food and keep it secret...If I tell my mother she will say I am bad.”[200]
Sexual violence against women and children with psychosocial and intellectual disabilities in particular remains hidden. Patience L., a nurse at a district clinic in Livingstone, told Human Rights Watch:
The mentally disabled get pregnant because of rape. We see a lot of sexual abuse of mental patients. But if someone is mentally disabled and the family hasn’t seen the rape, how would you know? If a woman can’t communicate, the family might only find out about the rape when the woman gets pregnant. Mental illness and intellectual disability are the most difficult to deal with. The neighbors will take advantage of her – sometimes they lure her with sweets.[201]
Health workers at “One Stop Centers” for child sexual abuse in tertiary hospitals in two provinces and counselors at victim support units in two districts in Lusaka told Human Rights Watch about the increasing incidence of sexual abuse of children with disabilities, in particular girls with intellectual disabilities and epilepsy.[202] In most of these cases, the child had either been abused by a caregiver or a neighbor or known person from the community when the child was left at home alone or left to wander the compound. In one case, staff from a shelter for victims of gender-based violence, were called to investigate the abuse of a 16-year old girl with intellectual disability who had given birth to three children, suspected to be the result of rape by her father. The staff member told Human Rights Watch: “She doesn’t know who is impregnating her...she can’t give any information.”[203] Home outreach workers and parents of girls with intellectual disabilities also told Human Rights Watch about the practice of keeping their children locked indoors due to their fear of sexual violence against them in the community.[204]
The vulnerability of women and girls with disabilities is compounded because they lack equal access to information about gender-based violence and HIV prevention as well as to social protection services.
IV. Relevant International, Regional, and Domestic Law
International Legal Obligations
The Zambian government is obliged under international and regional law to protect the rights of people with disabilities, including their right to health.
At the international level, Zambia is a party to core human rights treaties, which provide for the protection of basic civil, political, economic, social and cultural rights including specific guarantees relating to the right to health. These include the International Covenant on Civil and Political Rights (ICCPR),[205] the International Covenant on Economic, Social and Cultural Rights (ICESCR),[206]the Convention on the Elimination of Discrimination against Women (CEDAW),[207] the Convention on the Rights of the Child (CRC),[208] and the Convention on the Rights of Persons with Disabilities (CRPD) and its Optional Protocol.[209]The CRPD makes explicit that the human rights enumerated in other major human rights documents apply with equal force and in particularly important ways to persons with disabilities.
At the regional level, Zambia is party to several treaties including the African Charter on Human and Peoples’ Rights,[210] the African Charter on Human and Peoples' Rights on the Rights of Women in Africa (the Maputo Protocol),[211] and the African Charter on the Rights and Welfare of the Child.[212]
These treaties are supplemented by regional and international standards that provide guidance derived from international law on the provision of inclusive HIV and sexual and reproductive health services.
Right to Health
The human right to the highest attainable standard of health is enshrined in numerous international and regional human rights instruments, including the Universal Declaration of Human Rights, the ICESCR, the CRC, CEDAW, and the CRPD.[213] The ICESCR obligates governments to take steps individually and through international cooperation to progressively realize this right via the prevention, treatment, and control of epidemic diseases and the creation of conditions to ensure medical service and attention to all.[214]
The ICESCR obligates governments to ensure that health services are available, accessible, acceptable, and of good quality.[215] Availability comprises the availability of functioning healthcare services, medical personnel, and drugs, as well as safe water and sanitation. Accessibility means that health facilities should be accessible for everyone, without discrimination, and located within safe physical reach and economically affordable for all; it also comprises the right to seek and receive information on health services. Acceptability means that all health facilities need to adhere to ethical standards, including the principle of confidentiality.[216]
The CRPD provides certain protections to persons with disabilities as part of their right to the highest attainable standard of health, including the right to a range of healthcare services of adequate quality as close as possible to their communities.[217] Under article 25, persons with disabilities are entitled to “the same range, quality and standard of free or affordable health care and programmes as provided to other persons, including in the area of...population-based public health programmes.”[218] Governments are obligated to ensure that health professionals “provide care of the same quality to persons with disabilities as to others, including on the basis of free and informed consent by, inter alia, raising awareness of the human rights, dignity, autonomy and needs of persons with disabilities through training and the promulgation of ethical standards for public and private health care.”[219] The CRPD and the Women’s Protocol to the African Charter also require states to provide sexual and reproductive health care.[220]
Article 9 of the CRPD requires governments to take measures to ensure persons with disabilities have access, on an equal basis with others: to the physical environment, to transportation, to information and communications, including information and communications technologies and systems, and to other facilities and services open or provided to the public, both in urban and in rural areas. Under the CRPD, the physical environment includes buildings, roads, schools, housing, medical facilities, workplaces, and “other indoor and outdoor facilities.”[221]
Regional human rights instruments also support the right to health.[222] The African Charter obligates governments to take special measures to address the needs of persons with disabilities.[223] The Southern African Development Community (SADC) Protocol on Health calls on governments to ensure “a barrier free environment for the equalization of opportunities for people with disabilities.”[224] The Sexual and Reproductive Health Strategy for the SADC Region 2006-2015 includes in its guiding principles a priority for delivery of sexual and reproductive health and HIV services to vulnerable population groups including people living with disabilities.[225]
Underlying Determinants of Health
The right to health embraces a wide range of socio-economic factors that promote conditions in which people can lead a healthy life. States are obliged to ensure equal access for all to the underlying determinants of health including education and food and nutrition. The right to sexual and reproductive health is recognized as a fundamental part of the right to health.[226]
Education as a Determinant of Health
Under the Convention on the Rights of the Child, governments need to provide “youth-friendly and evidence-based comprehensive education to children and adolescents consistent with their evolving capacities, on human sexuality, sexual and reproductive health, human rights and gender equality” to ensure their right to sexual and reproductive health.[227]
The CRC Committee has recognized that “education plays a critical role in providing children with relevant and appropriate information on HIV/AIDS” by contributing to increased awareness, preventing negative attitudes towards victims of HIV and also by empowering children to protect themselves from the risk of HIV infection.[228]
Recognizing that children with disabilities, particularly during their adolescence, face “multiple challenges and risks in the area of establishing relationships with peers and reproductive health,” the CRC Committee recommends that governments provide adolescents with disabilities with adequate, and where appropriate, disability specific information, guidance and counseling.[229]
The CRPD obligates states to ensure that “persons with disabilities can access inclusive, quality and free primary education and secondary education on an equal basis with others in the communities in which they live.”[230] States are required to facilitate full and equal participation of persons with disabilities in education and as members of the community through appropriate measures including: the learning of sign language, braille alternative script, augmentative and alternative modes, means and formats of communication and orientation, and mobility skills, and by facilitating peer support and mentoring.[231]
Food and Nutrition as a Determinant of Health
Access to food and nutrition is recognized as an integral component of the right to health.[232] The right to food is also set out in the ICESCR. Governments are obligated to ensure access to the minimum essential food that is nutritionally adequate and safe and to ensure freedom from hunger to everyone.[233]The CRC Committee has also stated that comprehensive HIV treatment and care includes good nutrition.[234]Under the 2011 UN Nations Political Declaration on HIV and AIDS, UN member states have committed to integrate access to sufficient, safe and nutritious food as part of a comprehensive response to HIV/AIDS.[235]
Non–discrimination and Equal Recognition before the Law
The major international and regional human rights treaties expressly prohibit discrimination and require governments to take steps to eliminate all forms of discrimination against individuals, which include persons with disabilities.[236]
Non-discrimination is one of the cardinal principles upon which the CRPD is grounded.[237] The CRPD defines discrimination on the basis of disability as “any distinction, exclusion or restriction on the basis of disability which has the purpose or effect of impairing or nullifying the recognition, enjoyment or exercise, on an equal basis with others, of all human rights and fundamental freedoms in the political, economic, social, cultural, civil or any other field.”[238]
The CRPD sets minimum guiding standards for governments on how to realize equality and non-discrimination, including by recognizing that all persons are equal before and under the law and are entitled without discrimination to the equal protection and equal benefit of the law.[239] Article 12 of the CRPD obligates governments to recognize that persons with disabilities enjoy legal capacity on an equal basis with others in all aspects of life and to take appropriate measures to provide access by persons with disabilities to the support they may require in exercising their legal capacity.[240]
Article 8 of the CRPD requires governments to adopt immediate and effective measures to “raise awareness throughout society…to foster respect for the rights and dignity of persons with disabilities; to combat stereotypes, prejudices and harmful practices relating to persons with disabilities…in all areas of life; and to promote awareness of the capabilities and contributions of persons with disabilities.” [241]
According to the Committee on Economic, Social and Cultural Rights, access to health care (including the underlying determinants of health and to means and entitlements for their procurement) should be based on nondiscrimination, especially for “the most vulnerable or marginalized sections of the population, including individuals with disabilities.”[242] The CRPD further clarifies that the right to health must be upheld “without discrimination on the basis of disability.”[243]
Regional and international instruments on the provision of HIV services incorporate the requirement against discrimination on the basis of disability. The International Guidelines on HIV/AIDS and Human Rights recommend that states should “support the implementation of specially designed and targeted HIV prevention and care programmes for those who have less access to mainstream programmes due to language, poverty, social or legal or physical marginalization,” including persons with disabilities. [244] The Regional Minimum Standards for Harmonized Guidance on HIV Testing and Counselling in the SADC Region recommend that governments ensure access to HIV testing and counseling services for marginalized groups, with health staff trained in positive, non-judgmental attitudes. [245]
The CRPD also explicitly recognizes “that women and girls with disabilities are subject to multiple discrimination” and requires states to take all appropriate measures to ensure the full development, advancement and empowerment of women with disabilities.[246] According to the Committee on Economic, Social and Cultural Rights, the failure to protect women against violence amounts to violations of a government’s obligation to protect women’s right to health.[247]
Reasonable Accommodation
To realize the right of persons with disabilities to equal access to health care, the CRPD requires states to ensure “reasonable accommodation.” As defined by the CRPD, reasonable accommodation means “necessary and appropriate modification and adjustments not imposing a disproportionate or undue burden…to ensure to people with disabilities the enjoyment or exercise on an equal basis with others of all human rights and fundamental freedoms.”[248]
Measures to ensure access to health without discrimination include the promotion of “universal design” whereby “products, environments, programmes and services are designed to be usable by all people, to the greatest extent possible, without the need for adaptation or specialized design.”[249]
The CRPD also requires that governments facilitate “access by persons with disabilities to quality mobility aids, devices, assistive technologies and forms of live assistance and intermediaries, including by making them available at affordable cost.”[250]
Examples of reasonable accommodation in health care include changing the physical layout of clinics to provide access for people with mobility difficulties or communicating health information in accessible formats such as large print, braille, audio and picture format and through sign language interpretation.[251] Access to health care can also be facilitated by using equipment with universal design features (such as height adjustable examination tables, seated or platform scales and wheelchair accessible diagnostic equipment); making adjustments to appointment systems (by scheduling additional time for appointments or clustering appointments for disability needs); promoting peer support and using alternate forms of service delivery such as mobile and home outreach services.[252]
Right to Information, Participation and Confidentiality
The CRPD obligates governments to ensure that persons with disabilities can seek, receive and impart information and ideas on an equal basis with others and through all forms of communication of their choice, including by providing information intended for the general public in accessible formats and technologies appropriate to different kinds of disabilities in a timely manner and without additional cost.[253]
Article 26 of the CRPD guarantees that persons with disabilities should have access to habilitation and rehabilitation services including in the areas of health, education and social services with the purpose of ensuring their full inclusion and participation in all aspects of life.[254]
Article 22 requires governments to protect the privacy of personal, health and rehabilitation information of persons with disabilities on an equal basis with others.[255]
Zambian National Law and Policies
The 1991 Constitution of the Republic of Zambia contains one provision on persons with disabilities. In its Directive Principles of State Policy, the constitution provides that the “State shall endeavour to provide to persons with disabilities, the aged and other disadvantaged persons such social benefits and amenities as are suitable to their needs and are just and equitable.”[256] The constitution prohibits discrimination but disability is not specified as a prohibited basis.[257]
Zambia has been undertaking its recent constitutional review process since 2011. The 2012 draft constitution guarantees persons with disabilities enjoyment of all the rights and freedoms in the Bill of Rights and includes specific provisions on accessibility and equal access including in the areas of education and social security and protection. Disability is also explicitly included as a prohibited ground for discrimination.[258] The government should ensure that the new constitution guarantees persons with disabilities equality in all respects, including in relation to their right to health and education.
The Persons with Disabilities Act, 2012 (repealing the 1996 Persons with Disabilities Act) provides domestic legislation to incorporate the CRPD and mainstreaming of disability issues as an integral part of national policies.[259]
The act prohibits discrimination[260] and recognizes a series of rights including the right to family life,[261] legal protection and participation in judicial proceedings,[262] participation in political and public life,[263] as well as access to education,[264] health care,[265] habilitation and rehabilitation,[266] and employment and social protection.[267] It guarantees persons with disabilities the right to enjoy legal capacity on an equal basis with others in all aspects of life.[268] The act also addresses accessibility by persons with disabilities to the physical environment, transportation, information, communications and other facilities and services provided to the public, as well as prescribing measures to facilitate personal mobility.[269]
The 2012 act continues the existence of the National Trust Fund for Persons with Disabilities and the Zambia Agency for Persons with Disabilities established by the repealed 1996 act. It provides the agency with a comprehensive mandate to: plan, promote and administer services for persons with disabilities; ensure access to inclusive education at all levels, employment, community and social services; facilitate and coordinate rehabilitation services; promote public awareness and research on all aspects of disability; and take measures to eliminate discrimination and monitor and evaluate implementation of the act.[270]
In line with the CRPD, the 2012 act directs the government to provide persons with disabilities equal access to health care including in the area of sexual and reproductive health and population-based public health programs.[271] In addition to measures for early intervention, habilitation and rehabilitation, under the act the Ministry of Health is to include education on disability issues in healthcare programs and include the study of disability in the curriculum of training institutions for health professionals.[272]
The draft 2012 National Disability Policy recognizes that efforts aimed at responding to challenges faced by persons with disabilities have remained “fragmented, uncoordinated and ineffective due to lack of a policy framework.”[273] It aims to provide guidance to the government and non-state actors on the mainstreaming of disability in national development and sets out responsibilities for policy implementation across all line ministries, the judiciary, the Zambia Agency for Persons with Disabilities, DPOs, civil society and the private sector.[274]
Under the policy, the Ministry of Health is to ensure that persons with disabilities have access to primary health care; to enforce the code of conduct for public and private healthcare providers to address rights of persons with disabilities; to develop and strengthen specialized healthcare programs for persons with disabilities; and to ensure disability data is included in the health management information system.
V. Inclusion of People with Disabilities in Zambia’s National HIV Response
There is growing worldwide recognition that political and programmatic commitment to the provision of inclusive HIV services is necessary to overcome “the historic neglect of HIV prevention and support for people with disabilities.”[275] In the 2011 Political Declaration on HIV and AIDS, the UN General Assembly noted with concern that “prevention, treatment, care and support programmes adequately targeted or made accessible to persons with disabilities.”[276] Regionally, the African Union Sexual and Reproductive Health and Rights Continental Policy Framework calls on governments to develop preventive and curative HIV services for the most vulnerable groups including persons with disabilities.[277] In Zambia, the government is committed to ensuring that all “people have equal access and will utilise HIV services without stigmatisation or discrimination.”[278]
However, while the government recognized persons with disabilities as a vulnerable population within the 2011-2015 National AIDS Strategic Framework (NASF), it provided limited guidelines for inclusive or targeted services in its guidelines on specific interventions and strategies to strengthen and expand coverage of HIV services. It did not address the need for inclusive services in key areas such as condom promotion, male circumcision, HIV testing or ART delivery.[279] Guidelines on the provision of inclusive health care are also absent from the 2011-2015 National Health Strategic Plan (NHSP).[280]
In contrast to the 2006-2010 Fifth National Development Plan, which identified specific program objectives for people with disabilities within a development framework (including provisions for inclusive HIV and other health services), the 2011-2015 Sixth National Development Plan addresses the needs of people with disabilities within a social protection framework, and does not specify inclusive HIV and health strategies or programs.[281]
Role of National Agencies and Civil Society
One of the critical factors in the lack of adequate HIV services for persons with disabilities is the weak coordination between the agencies and ministries that address the needs of persons with disabilities and those responsible for the development and implementation of HIV programs. There is little sharing of data and collaboration on HIV program development between the Zambia Agency for Persons with Disabilities (ZAPD) established by the 1996 Persons with Disabilities Act and the National HIV/AIDS/STI/TB Council (NAC) established by the 2002 National HIV/AIDS/STI/TB Council Act. The ZAPD is currently undergoing re-structuring and has historically struggled with funding and resources, and data collection, administrative and technical capacity issues.[282]
At the ministry level, the Ministry of Community Development, Mother and Child Health undertakes responsibility for the delivery of primary healthcare services as well as overseeing the ZAPD (through its Social Welfare department). The Ministry of Health guides the NAC in its role as chair of the Cabinet Committee of Ministers on HIV/AIDS.[283]
Under the 2012 Persons with Disability Act, the Zambian government is required to provide inclusive education, employment, social protection and health services (including HIV prevention and treatment services) through the relevant line ministries. In response, the government has initiated a cross-cutting approach, and intends to appoint a focal person on disability in each ministry to ensure the mainstreaming of disability across multi-sectoral policies and programs.[284] To date, this approach has faced significant obstacles due to the lack of senior line ministry responsibility for mainstreaming disability, the lack of transparency and clarity in funding allocation for inclusive services, and the lack of data collection on persons with disabilities.[285] Representatives of DPOs and government officials told Human Rights Watch that implementation of the 2012 Act continues to be impeded by the lack of clarity on agency and ministry responsibilities and the delay in issuing statutory instruments to effect some provisions of the act.[286]
International and domestic organizations in Zambia also provide important services to persons with disabilities. ZAFOD is a key national umbrella organization, representing twelve Disabled Persons Organizations (DPOs). ZAFOD and numerous DPOs together with the Treatment Advocacy and Literacy Campaign (TALC) have increasingly advocated for the right of persons with disabilities to inclusive HIV services.[287] However, provision of HIV and health services is not supported by strong linkages across DPOs, HIV member organizations (such as networks of people living with HIV) and community-based healthcare organizations providing services to people with disabilities and people affected by HIV.
Role of Donors
International donors are uniquely placed to facilitate the full implementation of inclusive and targeted HIV services for persons with disabilities in Zambia. In addition to calling on the Zambian government to respect its human rights obligations to persons with disabilities, international donors should ensure that their own development assistance strategies and policies hold up to the principles of non-discrimination, inclusion and equality in health services as articulated in the Convention on the Rights of Persons with Disabilities and other treaties.
Donors have funded much of Zambia’s fight against HIV. More than eighty percent of Zambia’s HIV programmatic funding comes from external sources.[288] The US government via the President’s Emergency Plan for AIDS Relief (PEPFAR) is Zambia’s largest bilateral donor, providing more than US$1 billion between 2004 and 2009 for HIV programs.[289] In 2012 alone, Zambia received PEPFAR funding of $307 million.[290] The Global Fund for AIDS, Tuberculosis and Malaria (GFATM) is another important donor, having provided a total of $655 million for HIV programs since the launch of Round 1 funding in 2003.[291] In 2013, the Global Fund signed a three-year grant agreement (consolidating Rounds 8 and 10) for $156 million.[292] To date, relatively little of this assistance has been designated toward the provision of inclusive or targeted prevention, testing, treatment and care services for persons with disabilities, despite the existence of disability-inclusive programming guidelines.[293]
VI. Examples of Inclusive and Targeted HIV Services
Resource constraints, lack of prevalence data about persons with disabilities, and lack of technical capacity are the most widely cited reasons for not promoting inclusive and targeted HIV and sexual and reproductive health services. As the following examples show, an inclusive approach requires focused and strategic investment of existing resources and can be implemented through cost-effective approaches such as peer teaching, knowledge sharing, modified allocation of human resources and adaptation of core knowledge resources. An inclusive approach can result in improved HIV prevention, testing and treatment services for all people, through development of community-based health infrastructure including volunteer and mobile outreach services and health literacy. Importantly, both targeted and inclusive models of HIV services require the involvement and input of persons with disabilities to ensure they reach persons with disabilities through appropriate community linkages and are responsive to the various barriers faced by persons with disabilities.
Good Practices in Zambia
Peer-Based Deaf HIV Testing Services
Under a pilot program launched by Zambia Deaf Youth and Women (ZDYW) in 2012, 30 deaf persons in the Copperbelt province have been trained as VCT counselors.[294] With the support of provincial and district-level staff from the Ministry of Community Development and Mother and Child Health, deaf-friendly VCT services are currently being provided in primary care health facilities in six districts in the Copperbelt Province.[295] Deaf clients at these facilities are assured of confidentiality and access to full pre and post-HIV-test counseling information in sign language. These services have led to an uptake of VCT services by deaf persons at the pilot facilities and a demand for mobile peer-based VCT services by the deaf community.[296]
Provision of Home Care and Mobile Outreach to Persons with Psychosocial Disabilities Living with HIV
In collaboration with the Ministry of Health, the St. Francis Community Integrated Care Programme in Livingstone in the Southern Province supports a weekly mobile mental health clinic for persons with psychosocial disabilities and epilepsy, including persons living with HIV. The clinic is conducted on the premises of a primary care health facility providing ART services. Patients are provided with counseling, medical referrals and ongoing management of psychiatric and epilepsy medication by a psychiatric clinical officer from Livingstone General Hospital and healthcare workers from St. Francis.
Community care workers from St. Francis educate persons with psychosocial disabilities and their caregivers about HIV and psychosocial disability and ensure that persons with disabilities who are living with HIV (especially those living without any family support) attend their ART appointments and regularly access mental health services through the mobile clinic. They also provide persons with psychosocial disabilities with home-based care and support including nutritional support and counseling on medication adherence.[297]
Good Practices in Southern Africa
Zimbabwe – Development of a Sexual and Reproductive Health Sign-Language Dictionary
To address the lack of accessible information on HIV and sexual and reproductive health (SRH) services for persons with hearing disabilities in Zimbabwe, the HIV and AIDS Management and Support Organization (THAMASO-ZIMBABWE) and Disability HIV & AIDS Trust (DHAT) produced a sign-language dictionary for HIV and sexual and reproductive health and rights terms in 2013. It is designed for use within both educational and health institutions. The sign-language dictionary provides deaf persons with access to comprehensive information and clear communication in HIV and SRH services through a standardized sign-language vocabulary.The dictionary includes an illustrated guide to signing for individual letters as well as illustrations and descriptions for common HIV and SRH signs, and was developed in consultation with people with hearing disabilities from all provinces in Zimbabwe.[298]
South Africa – Ethical Guidelines for Healthcare Workers on HIV Counseling and Testing for People with Intellectual Disabilities
Recognizing that healthcare workers require specific skills to provide inclusive HIV services to persons with intellectual disabilities, the Western Cape Forum for Intellectual Disability developed ethical guidelines and training to support healthcare workers. These guidelines support the need to involve people with intellectual disabilities in their healthcare decision-making and include information about informed consent, tools to guide HIV risk assessment, HIV education and pre- and post-test counseling for persons with disabilities. [299]
Recommendations
To the Government of Zambia and the Zambia National Assembly
- Develop and promulgate regulations to ensure effective implementation of the 2012 Persons with Disabilities Act.
- Review all domestic legislation and amend laws and regulations as necessary to ensure harmonization with the 2012 Persons with Disabilities Act.
- Repeal the 1951 Mental Disorders Act and fully align the Mental Health Service Bill with the Convention on the Rights of Persons with Disabilities (CRPD).
- Ensure that the final version of the draft constitution retains provisions relating to persons with disabilities (including non-discrimination, accessibility and right to education).
- Submit Zambia’s first country progress report on implementation of the CRPD to the Committee on the Rights of Persons with Disabilities.
- Ratify the Optional Protocol to the CRPD.
To the National HIV/AIDS/STI/TB Council, Zambia Agency for Persons with Disabilities, Ministry of Community Development, Mother and Child Health, and the Ministry of Health
- Strengthen linkages between the National AIDS Council and the Zambia Agency for Persons with Disabilities, including data sharing and monitoring of HIV service delivery for persons with disabilities.
- Ensure input of persons with different disabilities across all HIV technical working groups providing guidance on HIV services and programs.
- Establish a national HIV and Disability unit
with representation of persons with different disabilities and responsibility
for development of a national database on:
- Human resources (such as deaf HIV testing counselors, HIV peer counselors in different districts);
- Best practice HIV service delivery models for persons with disabilities; and
- Technical resources for the development of HIV communication, education and information materials for persons with different disabilities.
- Strengthen integration of mental health and HIV and at all levels of healthcare delivery.
- Strengthen inclusive HIV services for adolescents at health facilities; develop accessible package of health services through the Adolescent Friendly Health Services program.
- Develop guidelines on reasonable accommodation in HIV testing, adherence monitoring and counseling; and provide training to ART and HIV testing counselors. Develop adherence monitoring guidelines that are responsive to the differentiated circumstances of persons with disabilities.
- Develop guidance on HIV disclosure counseling to children and adolescents with disabilities living with HIV, taking into account their emotional and cognitive maturity.
- Develop code of ethics for HIV testing, diagnosis and counseling services for persons with disabilities and provide training to health workers providing HIV services.
- Develop ethical guidance on HIV testing and disclosure for sign language interpreters working in health facilities.
- Provide reasonable accommodation to people with disabilities in patient management processes at health facilities, including within patient waiting areas.
- Develop HIV prevention and treatment campaigns depicting and involving persons with disabilities.
- Provide information, education, and communication (IEC) materials on HIV prevention, ART and positive living in large print, braille, easy to read, local language and sign language.
- Develop national accessibility standards including for hospitals, health facilities and schools.
- Make hospitals and health centers accessible for persons with disabilities. Ensure that health facilities have ramps, accessible examination and counseling rooms and toilets, and sign language interpreters. Train health workers in basic sign language.
- Monitor the provision of HIV prevention, testing and treatment services to determine they are reaching people with disabilities and collect disaggregate data on people with disabilities among HIV services clients. Incorporate data on disability within the SmartCare electronic health records system.
- Encourage persons with disabilities to apply for positions in the HIV services sector and make reasonable accommodations for them.
- Increase provision of testing and counseling services by DPOs.
- Strengthen peer-based prevention, testing and treatment support programs for persons with disabilities through recruitment and training of people with disabilities as HIV educators and counselors.
- Strengthen home-based care, outreach services and mobile clinics for HIV service delivery to persons with disabilities.
- Provide in-service training to HIV services health workers on differentiated needs of persons with different disabilities.
- Ensure there are functioning, accessible complaints mechanisms to report barriers to HIV and health services including discrimination in health facilities.
To the Ministry of Community Development, Mother and Child Health
- Implement a twin-track approach to mainstreaming disability within HIV services provision by ensuring accessible mainstream services and establishing targeted services for people with disabilities.
- Establish senior line ministry accountability for mainstreaming of disability issues across line ministries with a transparent reporting framework.
- Finalize and operationalize a comprehensive National Disability Policy with the input of persons with different disabilities.
- Expand community-based rehabilitation (CBR) programs and strengthen linkage with HIV services.
- Strengthen and expand income generation and social protection programs targeting people with disabilities.
- Disclose and monitor budget allocation of funds toward disability mainstreaming in each line ministry, including for HIV services.
- Ensure inclusive and targeted schemes for child protection and social protection (e.g. cash transfer programs) for children with disabilities.
To the Zambia Agency of Persons with Disabilities and DPOs
- Develop and implement public awareness programs in collaboration with DPOs and community leaders to combat stigma and discrimination based on stereotypes, prejudices and harmful practices relating to persons with disabilities.
- Implement monitoring and evaluation mechanisms for provision of health, education and social protection services including accessibility audits.
- Promote HIV prevention and positive living peer support groups for people with disabilities.
- Strengthen linkages between DPOs and HIV organizations including networks of people living with HIV.
- Develop a framework through which rights of persons with disabilities generally are monitored. This should be done in conjunction with ZAPD and the Zambia Human Rights Commission.
To the Ministry of Community Development, Mother and Child Health and the Ministry of Health and the Central Statistics Office
- Establish regular data collection on persons with disabilities, utilizing the Washington Group approach for capturing the full spectrum of functioning.
- Incorporate disaggregated data collection and reporting on persons with disabilities within national surveys including the Demographic and Health Survey, Sexual Behavior Survey and Antenatal Care Surveillance Survey.
To the Ministry of Home Affairs, the Zambian Police (Especially the Victim Support Unit), Ministry of Gender and Child Development
- Train Victim Support Unit officers on how to respect the rights of persons with disabilities and develop inclusive protocols on handling cases of gender-based and sexual violence, including techniques for interviewing survivors, maintaining their privacy, referring them to health services and providing protection for survivors.
- Provide sign language interpreters at police stations or identify volunteer sign language interpreters through local Disabled Persons Organizations.
- Expressly include and address the rights and challenges of women and girls with disabilities in community sensitization and other community-based interventions concerning gender-based violence.
- Develop accessible and inclusive child protection systems for children with disabilities.
To the Ministry of Education, Science, Vocational Training and Early Education
- Ensure inclusion of children with disabilities in HIV peer support programs conducted in school settings.
- Develop inclusive and targeted curriculum materials on HIV prevention and life skills for children and youth with disabilities in braille, large print, easy to read and sign language formats.
- Develop comprehensive policy on inclusive education including development of accessible curricula and learning materials and ongoing teacher education.
- Work with community leaders and DPOs to establish community-based right to education campaigns for children with disabilities.
To UN Agencies and the UN Special Rapporteurs
- Develop core indicators to monitor access to HIV services across the prevention and care continuum by persons with disabilities.
- Recognize persons with disabilities as a priority population and develop policy guidance on programming of inclusive HIV services.
- Expand programs supporting the right to sexual and reproductive information and services for people with disabilities.
- Develop inclusive programming and protocols for the implementation of the Anti-Gender-Based Violence Act under the UN Joint Programme on Gender Based Violence (2012-2016).
- Promote and develop life skills and HIV prevention materials for children with disabilities.
- UN Special Rapporteur on the Right to the Enjoyment of the Highest Attainable Standard of Physical and Mental Health should investigate barriers to access to HIV services faced by persons with disabilities.
To Donor Countries andDonor Agencies working on HIV/AIDS including the Global Fund and PEPFAR
- Assist the government through technical and financial support, with the design and implementation of inclusive HIV programming within each stage of the HIV continuum for persons with disabilities.
- Support design and implementation of inclusive condom promotion and distribution campaigns.
- Promote implementation of universally designed HIV programs and protocols in funded activities. Designate funds for targeted HIV programming for persons with different disabilities.
- Incorporate disability indicators for post-2015 development goals and targets on HIV.
Acknowledgments
This report is dedicated to the memory of Winstone Zulu, Zambia’s courageous HIV and TB activist and an important advocate for the rights of persons with disabilities.
This report was written by Rashmi Chopra, research fellow in the Disability Rights Division. The report is based on research conducted by Rashmi Chopra, Megan McLemore, senior researcher in the Health and Human Rights Division, and consultant Laura Thomas. The report was reviewed and edited by Shantha Rau Barriga, director of the Disability Rights Division; Joseph Amon, director of the Health and Human Rights Division; Tiseke Kasambala, Southern Africa Director in the Africa Division; Juliane Kippenberg, senior researcher in the Children’s Rights Division; Agnes Odhiambo, senior researcher in the Women’s Rights Division; James Ross, legal and policy director; Babatunde Olugboji, deputy program director; and Danielle Haas, senior program editor at Human Rights Watch.
Additional research support was provided by Jessica Harper, Jenny Nilsson, Betsy Krupar and Lea Labaki, interns in the Disability Rights Division. Jennifer Pierre, Fitzroy Hepkins, Jose Martinez, Grace Choi and Jessie Graham provided production and editorial assistance. Josh Lyons and Grace Choi designed the map in the report.
Human Rights Watch expresses its deep appreciation to the disabled peoples’ organizations, HIV and health services organizations, government agencies, nongovernmental organizations and individuals in Zambia who facilitated interviews and provided invaluable assistance in the research and preparation of this report.
Human Rights Watch thanks all of the persons with disabilities who agreed to be interviewed for this report. Their willingness to share their stories made this report possible.
[1] Collins English Dictionary: Complete & Unabridged 10th Edition, 2009, http://dictionary.reference.com/browse/Cerebral+Palsy (accessed April 6, 2014); The American Heritage Stedman’s Medical Dictionary, 2002, http://dictionary.reference.com/browse/Cerebral+Palsy (accessed June 2, 2014).
[2] American Association on Intellectual and Developmental Disabilities, “FAQ on Intellectual Disability,” 2011, http://aaidd.org/intellectual-disability/definition/faqs-on-intellectual-disability#.U5e2kC-QMXw (accessed June 2, 2014).
[3] Centers for Disease Control and Prevention, “Developmental Disabilities,” undated, http://www.cdc.gov/ncbddd/developmentaldisabilities/features/birthdefects-dd-keyfindings.html (accessed June 2, 2014).
[4] World Network of Users and Survivors of Psychiatry, “Manual on Implementation of the Convention on the Rights of Persons with Disabilities,” http://www.chrusp.org/home/resources (accessed June 2, 2014), p. 9.
[5] Human Rights Watch interview with Daniel L., Lusaka, February 14, 2014.
[6] We also held group discussions with 38 deaf children at two special education units for deaf and hearing-impaired children at a primary and secondary school in Kitwe and Lusaka.
[7] See Human Rights Watch, Unjust and Unhealthy: HIV,TB, and Abuse in Zambian Prisons, April 2010, http://www.hrw.org/sites/default/files/reports/zambia0410webwcover.pdf; Human Rights Watch, Hidden in the Mealie Meal: Gender-based Abuses and Women’s HIV Treatment in Zambia, December 2007, http://www.hrw.org/sites/default/files/reports/zambia1207web.pdf; Human Rights Watch, Suffering in Silence: The Links Between Human Rights Abuses and HIV Transmission to Girls in Zambia, November 2002, http://www.hrw.org/reports/2003/zambia/zambia1202.pdf.
[8] UNAIDS, “Global Report: UNAIDS Report on the Global AIDS Epidemic 2013,” 2013, http://www.unaids.org/en/media/unaids/contentassets/documents/epidemiology/2013/gr2013/UNAIDS_Global_Report_2013_en.pdf (accessed May 22, 2014), p.4.
[9] UNAIDS, “Getting to Zero: HIV in Eastern and Southern Africa: Regional Report 2013,” http://www.unaidsrstesa.org/sites/default/files/unaids_esa_report_july_2013.pdf (accessed May 22, 2014), p.9 (noting figures for 2011).
[10] UNAIDS, “UNAIDS HIV and AIDS Estimates 2012,” undated, http://www.unaids.org/en/regionscountries/countries/zambia/ (accessed May 22, 2014); See “The Global Fund TB and HIV Concept Note,” Draft Document, May 2014, p.3 (noting adult HIV prevalence of “just above 12.6%”), p.3 (noting 2013 data).
[11] The number of CD4 cells (T-helper lymphocytes with CD4 cell surface marker) used to assess immune status, susceptibility to opportunistic infections, and a patient’s need for ART; CD4 count is the most important lab result for untreated HIV patients. Joel E. Gallant and Christopher Hoffmann, Johns Hopkins Point-of-Care Information Technology, “HIV Guide: CD4 Cell Count,” March 18, 2009, http://www.hopkinsaids.edu/management/laboratory_testing/cd4_cell_count.html?contentInstanceId=8279 (accessed May 22 2014).
[12] World Health Organization, “Zambia: Summary Country Profile for HIV/AIDS Treatment Scale Up,” 2005, http://www.who.int/hiv/HIVCP_ZMB.pdf (accessed May 22, 2014), p.2.
[13] Ministry of Health and National HIV/AIDS/STI/TB Council, “National AIDS Strategic Framework 2011-2015: Joint Mid Term Review Report,” December 2013, p.2.
[14] Ministry of Health and National HIV/AIDS/STI/TB Council, “National AIDS Strategic Framework 2011-2015: Towards Improving the Quality of Life of the Zambian People,” November 2010, http://www.aidstar-one.com/sites/default/files/prevention/resources/national_strategic_plans/Zambia%20NASF%202011-2015.pdf (accessed May 22, 2014), p.15; “National AIDS Strategic Framework 2011-2015: Joint Mid Term Review Report,” December 2013, p.59.
[15] Republic of Zambia “Zambia Country Report: Monitoring the Declaration of Commitment on HIV and AIDS and the Universal Access, Biennial Report,” March 31, 2012, http://www.unaids.org/en/dataanalysis/knowyourresponse/countryprogressreports/2012countries/ce_ZM_Narrative_Report.pdf, (accessed May 22, 2014), p.36; See “The Global Fund TB and HIV Concept Note,” Draft Document, May 2014, p.20. The current ART treatment protocol in Zambia is based on 2013 World Health Organization (WHO) guidelines. See Ministry of Health and Ministry of Community Development, Mother and Child Health, “Zambia Consolidated Guidelines for Treatment and Prevention of Infection,” February 2014; WHO, “Consolidated Guidelines on The Use of Antiretroviral Drugs for Treating and Preventing HIV Infection,” June 2013, http://www.who.int/hiv/pub/guidelines/arv2013/download/en/ (accessed May 14, 2014).
[16] Ministry of Health and National HIV/AIDS/STI/TB Council, “National AIDS Strategic Framework 2011-2015: Towards Improving the Quality of Life of the Zambian People,” http://www.aidstar-one.com/sites/default/files/prevention/resources/national_strategic_plans/Zambia%20NASF%202011-2015.pdf, (accessed May 22, 2014), p. 11.
[17] Kampala Declaration on Disability and HIV & AIDS, 2008, http://www.dhatregional.org/docs/kampala_declaration_hivaids_disability[1].pdf (accessed May 22, 2014). The first African Decade of Persons with Disabilities (1999-2009) was established by the African Union to promote the full participation and equality of people with disabilities in Africa. The African Campaign on Disability and HIV & AIDS was launched during the first decade to ensure mainstreaming of persons with disabilities within the HIV response by governments within the region. See also: Waimar Tun et al, “Situation Analysis of Programs to Meet the Prevention, Care and Treatment Needs of Persons With Disabilities in Ghana, Uganda, and Zambia,” HIVCore Final Report, Washington, DC: USAID, 2013, http://www.hivcore.org/Pubs/HIVandPersonsWithDisabilities_Rprt.pdf (accessed May 18, 2014); Jill Hanass-Hancock, “Disability and HIV/AIDS – A Systematic Review of Literature on Africa,” Journal of the International AIDS Society, 12:24, 2009, http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2788347/ (accessed May 18, 2014); Stephanie A. Nixon et al, “The Sepo Study Report and Supplementary Appendices,” 2011 (shared by author); Stephanie A. Nixon et al., “Perceptions of HIV-related Health Services in Zambia for People With Disabilities Who Are HIV-positive,” Journal of International AIDS Society, 17(1), 2014, http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4000430/#S0001title (draft shared by author); Karen Yoshida, Stephanie A. Nixon et al., “Using Intersectionality to Explore Experiences of Disability and HIV Among Women and Men in Zambia,” Disability Rehabilitation, 2014 (draft shared by author).
[18] Republic of Zambia, The Persons with Disabilities Act, No. 6 of 2012, http://www.zambialii.org/files/zm/legislation/act/2012/6/The%20Persons%20with%20disabilities%20act,%202012%20(1).PDF, Part V, Sec. 27 (a).
[19] Ministry of Community Development, Mother and Child Health, “National Policy on Disability: Empowering Persons with Disabilities,” September 2012 Draft, p.13.
[20] Ministry of Health and National HIV/AIDS/STI/TB Council, “National AIDS Strategic Framework 2011-2015: Towards Improving the Quality of Life of the Zambian People,” http://www.aidstar-one.com/sites/default/files/prevention/resources/national_strategic_plans/Zambia%20NASF%202011-2015.pdf, (accessed June 27, 2014), p.11.
[21]World Bank and World Health Organization, “World Report on Disability,” 2011, http://whqlibdoc.who.int/publications/2011/9789240685215_eng.pdf, (accessed May 18, 2014), p.29, 44.
[22] Zambia Central Statistical Office, “2010 National Census of Population and Housing: National Analytical Report,” 2012, http://www.zamstats.gov.zm/report/Census/2010/2010%20Census%20of%20Population%20National%20Analytical%20Report%20-%202010%20Census.pdf (accessed May 20, 2014), p.71.
[23] SINTEF, “Living Conditions among People with Activity Limitations in Zambia: A National Representative Study,” 2006, http://www.sintef.no/upload/Helse/Levekår%20og%20tjenester/ZambiaLCweb.pdf (accessed May 20, 2014), p.74. The SINTEF survey applied the WHO framework for measuring health and disability at both individual and population levels, called the International Classification of Functioning, Disability and Health (ICF) and utilized the screening framework developed by the Washington Group on Disability Statistics. The ICF was officially endorsed by all 191 WHO Member States in the Fifty fourth World Health Assembly in May 2001 (resolution WHA 54.21). See World Health Organization, “International Classification of Functioning, Disability and Health,” May 22, 2001, http://www.who.int/classifications/icf/en/ (accessed May 18, 2014); Washington Group on Disability Statistics, http://unstats.un.org/unsd/methods/citygroup/washington.htm (accessed May 18, 2014); Mitchell Loeb et al., “Approaching the Measurement of Disability Prevalence: The Case of Zambia”, European Journal of Disability Research 2(2008):32-43, (accessed May 18), 2014, doi: 10.1016/j.alter.2007.06.001.
[24]World Bank and World Health Organization, “World Report on Disability,” http://whqlibdoc.who.int/publications/2011/9789240685215_eng.pdf, p.30; See also World Health Organization, “The Global Burden of Disease: 2004 Update,” 2008, http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf?ua=1 (accessed May 18, 2014) pp. 31-35.
[25] Zambia Central Statistical Office, “2010 National Census of Population and Housing: National Descriptive Tables,” http://www.zamstats.gov.zm/report/Census/2010/2010%20Census%20of%20Population%20National%20Descriptive%20Population%20Tables.pdf, (accessed June 1, 2014), p.260.
[26] Ministry of Education, “2010 Educational Statistical Bulletin,” p. 93; Basic schools include government and grant aided schools as well as community and private schools.
[27] Stigmatization of children and adults with disabilities, associated with witchcraft has been documented in a number of African countries. See Jill Hanass-Hancock, “Invisible - The Notion of Disability in the Context of HIV/AIDS in KwaZulu-Natal,” (PhD thesis, Humboldt University, Berlin, Germany, 2008); Emelie Secker, “Witchcraft Stigmatization in Nigeria: Challenges and Successes in the Implementation of Child Rights,” International Social Work 56(2013): 22-36, accessed May 18, 2014, doi: 10.1177/0020872812459065.
[28] Zambia Central Statistical Office, “2010 National Census of Population and Housing: National Analytical Report,” http://www.zamstats.gov.zm/report/Census/2010/2010%20Census%20of%20Population%20National%20Analytical%20Report%20-%202010%20Census.pdf, p. 70 (noting 12 categories: blind, partially sighted, deaf and dumb, deaf, hard of hearing, dumb, mentally ill, intellectual, speech impairment, physically disabled, mentally retarded, other).
[29] Ibid., p. 71.
[30] See World Bank “Zambia Country Data,”2014, http://data.worldbank.org/country/zambia (accessed June 27, 2014), noting 2013 population estimate of 14.54 million.
[31] CRPD, art. 1.
[32] Republic of Zambia, The Persons with Disabilities Act, No. 6 of 2012, http://www.zambialii.org/files/zm/legislation/act/2012/6/The%20Persons%20with%20disabilities%20act,%202012%20(1).PDF, (defining disability as: “a permanent physical, mental, intellectual or sensory impairment that alone, or in a combination with social or environmental barriers, hinders the ability of a person to fully or effectively participate in society on an equal basis with others”).
[33] Zambia Central Statistical Office, “2010 National Census of Population and Housing: National Analytical Report,” http://www.zamstats.gov.zm/report/Census/2010/2010%20Census%20of%20Population%20National%20Analytical%20Report%20-%202010%20Census.pdf, p.72.
[34] See World Bank, “HIV/AIDS & Disability: Capturing Hidden Voices, The World Bank/Yale Global Survey on HIV/AIDS and Disability,”2004, http://siteresources.worldbank.org/DISABILITY/Resources/Health-and-Wellness/HIVAIDS.pdf, (accessed June 1, 2014), p. 9-12; UNICEF, “The State of the World’s Children 2013 – Children with Disabilities,” May 2013, http://www.unicef.org/sowc2013/files/SWCR2013_ENG_Lo_res_24_Apr_2013.pdf (accessed June 1, 2014); WHO/UNFPA, “Guidance Note: Promoting Sexual and Reproductive Health for Persons with Disabilities,” 2009, http://www.unfpa.org/webdav/site/global/shared/documents/publications/2009/srh_for_disabilities.pdf, (accessed May 18, 2014), p.6; UNAIDS, WHO and OHCHR, “Disability and HIV Policy Brief,” April 2009, http://www.who.int/disabilities/jc1632_policy_brief_disability_en.pdf, (accessed June 1); Jill Hanass-Hancock, “Disability and HIV/AIDS – A Systematic Review of Literature in Africa,” Journal of the International AIDS Society, 12 (2009): accessed June 1, 2014, doi: 10.1186/1758-2652-12-34.
[35] Office of the United Nations High Commissioner for Human Rights and the Joint United Nations Programme on HIV/AIDS, “International Guidelines on HIV/AIDS and Human Rights,” 2006, http://data.unaids.org/publications/irc-pub07/jc1252-internguidelines_en.pdf (accessed June 1, 2014), para.97.
[36] There is no collection of disaggregated data about people with disabilities in Zambia’s national surveys such as the Demographic Health Survey and the Sexual Behaviour Survey and in reporting on HIV/ AIDS indicators.
[37] Zambia Central Statistical Office, “2010 National Census of Population and Housing: National Analytical Report,” http://www.zamstats.gov.zm/report/Census/2010/2010%20Census%20of%20Population%20National%20Analytical%20Report%20-%202010%20Census.pdf, p.73.
[38] Ibid.; See SINTEF, “Living Conditions among People with Activity Limitations in Zambia: A National Representative Study,” http://www.sintef.no/upload/Helse/Levekår%20og%20tjenester/ZambiaLCweb.pdf, p.74. (The SINTEF survey showed that of those children who acquired their disability before the age of 18: 33 percent of children with disabilities aged 5 years and over did not attend primary school; 66 percent of children with disabilities aged 15 years and over did not attend secondary school and over 90 percent of young people aged 18 years and over years did not attend tertiary or vocational training).
[39] Jean-Francois Trani, and Mitchelle Loeb, “Poverty and Disability: a Vicious Circle? Evidence from Afghanistan and Zambia,” Journal of International Development 24 (2010): S19-S52, accessed June 1, 2014, doi: 10.1002/jid.1709; Nora Groce et al., “Disability and Poverty: The Need for a More Nuanced Understanding of the Implications for Development Policy and Practice,” Third World Quarterly 32 (2011): 1493-1513, accessed June 1, 2014, doi: 10.1080/01436597.2011.604520; Nora Groce et al., “Poverty and Disability: A Critical Review of the Literature in Low and Middle-income Countries, September 2011, http://www.ucl.ac.uk/lc-ccr/centrepublications/workingpapers/WP16_Poverty_and_Disability_review.pdf (accessed May 14, 2014); The National HIV/AIDS/STI/TB Council indicated the pending release of an updated National AIDS Strategic Framework for the period 2014-2016, which will more explicitly recognize this link and address the need for the prioritization for access to HIV services and provide more comprehensive guidelines on inclusive interventions. Human Rights Watch interview with Dr. Witola, Director of Programmes, National HIV/AIDS/STI/TB Council, Lusaka, May 28, 2014.
[40] DFID, “Disability, Poverty and Development,” 2000, http://www.handicap-international.fr/bibliographie-handicap/4PolitiqueHandicap/hand_pauvrete/DFID_disability.pdf (accessed June 3, 2014), p.3; UN Enable, “Mainstreaming Disability in the Development Agenda,” undated, http://www.un.org/disabilities/default.asp?id=1569 (accessed June 3, 2014).
[41] World Bank, “Social Analysis and Disability: A Guidance Note,” March 2007, http://hpod.pmhclients.com/pdf/SAnalysisDis.pdf (accessed May 18, 2014), p. 9.
[42] Ibid.
[43] See United Nations Development Programme, “Millennium Development Goals, Zambia Progress Report 2013,”2013, http://www.zm.undp.org/content/dam/zambia/docs/mdgs/MDG%20Report%202013.pdf, noting 2010 data (accessed May 18, 2014), p.16; World Bank, “World Development Indicators,”2014, http://data.worldbank.org/country/zambia#cp_wdi, noting 2010 data (accessed May 18, 2014); Central Statistical Office, “Living Conditions Monitoring Survey Report 2006 & 2010,” undated, http://www.zamstats.gov.zm/report/Lcms/2006-2010%20LCMS%20Report%20Final%20Output.pdf (accessed May 18, 2014), p. 179-180 (noting that “the food poverty line, which corresponds to the cost of the food basket, has been designated by the CSO as the extreme poverty line, while the basic needs basket has been designated as the moderate poverty line. In the case of Zambia, households whose per adult equivalent expenditure is less than the extreme poverty line are classified as extremely poor, while households whose per adult equivalent expenditure is equal to the food poverty line (extreme line) but falls below the moderate line are said to be moderately poor”).
[44]SINTEF, “Living Conditions among People with Activity Limitations in Zambia: A National Representative Study,” http://www.sintef.no/upload/Helse/Levekår%20og%20tjenester/ZambiaLCweb.pdf,(accessed June 5, 2014) p.131.
[45] Central Statistical Office, “National Demographic and Health Survey 2007,” March 2009, http://dhsprogram.com/pubs/pdf/FR211/FR211%5Brevised-05-12-2009%5D.pdf (accessed May 18, 2014), p. 275 (indicating that almost half (47%) of all Zambian women have experienced physical violence since age 15); Central Statistical Office, “Zambia Sexual Behaviour Survey 2009,” 2009, http://www.zamstats.gov.zm/report/Demo/zambia_sexual_behaviour_2009.pdf (accessed May 18, 2014), Appendix: A88 (noting that 21.3 percent of females in urban areas and 17.8 percent of women in rural areas reported being ever forced to have sex.); Human Rights Watch, Hidden in the Mealie Meal: Gender-Based Abuses and Women's HIV Treatment in Zambia.
[46] See Marit Hoem Kvam, and Stine Hellum Braathen, “I Thought…Maybe This is My Chance: Sexual Abuse against Girls and Women with Disabilities in Malawi,” Sexual Abuse, 20 (2008): 5-27, accessed May 1, 2014, doi: 10.1177/1079063208314817; Soraya Maart and Jennifer Jelsma, “The Sexual Behaviour of Physically Disabled Adolescents,”
Disability and Rehabilitation 32 (2010): 438-43, accessed May 1, 2014, doi: 10.3109/09638280902846368; Sumaya Mall & Leslie Swartz, “Sexuality, Disability and Human Rights: Strengthening Health Care for Disabled People,” South African Medical Journal, 102 (2012):792-3, accessed May 1, 2014, doi: 10.7196/samj.6052; Karen Hughes et al., “Prevalence and Risk of Violence against Adults with Disabilities: a Systematic Review and Meta-analysis of Observational Studies,” Lancet 379 (2012):1621-9, accessed June 1, 2014, doi: 10.1016/S0140-6736(11)61851-5; Lisa Jones et al., “Prevalence and Risk of Violence against Children with Disabilities: a Systematic Review and Meta-analysis of Observational Studies,” Lancet 380(2012):899-907, accessed June 1, 2014, doi: 10.1016/S0140-6736(12)60692-8.
[47] World Bank, “HIV/AIDS & Disability: Capturing Hidden Voices, The World Bank/Yale Global Survey on HIV/AIDS and Disability,” http://siteresources.worldbank.org/DISABILITY/Resources/Health-and-Wellness/HIVAIDS.pdf, p. 10.
[48] The African Child Policy Forum, “Violence Against Children with Disabilities in Africa, A Compilation of the Main Findings of the Various Research Projects conducted by the African Child Policy Forum (ACPF) since 2006” March 2011, http://www.africanchildforum.org/site/images/stories/ACPF_violence_against_children.pdf (accessed June 1, 2014), p. 22, (noting that 52 % of survey respondents from Zambia reported incidents of forced sex).
[49] See Miriam Taegtmeyer et al., “A Peer-led HIV Counselling and Testing Programme for the Deaf in Kenya,” Disability and Rehabilitation, 31 (2009):508-514, accessed May 1, 2014, doi: 10.1080/09638280802133115; Olive Shisana et al., South African National HIV Prevalence, Incidence, Behaviour and Communication Survey 2008: A Turning Tide among Teenagers? (Cape Town: HSRC Press, 2010); See also Nora Groce et al., “HIV Issues and People with Disabilities: A Review and Agenda for Research,” Social Science & Medicine 77 (2013): 31-40, accessed June 1, 2014, doi: 10.1016/j.socscimed.2012.10.02; Patric Lunberg et al., “HIV Prevalence in Persons with Severe Mental Illness in Uganda: A Cross-Sectional Hospital-Based Study,” International Journal of Mental Health Systems, 2013 (7): accessed June 1, 2014, doi: 10.1186/1752-4458-7-20.
[50] USAID, AIR, World Vision, “Vulnerability for Households with Persons with Disabilities and HIV/AIDS in Chongwe, Zambia,” March 2010, http://www.air.org/sites/default/files/downloads/report/Vulnerability_for_Households_w_Disability_and_HIV_in_Chongwe_Zambia_Final_0.pdf (accessed June 10, 2014), p.11 (finding that disability was present in over 35.7 percent of HIV/AIDS vulnerable households in one district in Lusaka); F. Simende, “A Synopsis of Mental Health in Zambia,” 2013, Medical Journal of Zambia, http://www.mjz.co.zm/content/synopsis-mental-health-zambia (accessed June 1, 2014) (estimating a 20 percent HIV prevalence among mental health inpatients at Chainama Hills Hospital in Lusaka); N. Kankinza, “The Neglected Issue of HIV Infection in Psychiatric Patients in Zambia: A Case of Ndola Central Hospital,” draft paper shared by author (noting HIV prevalence of 32.2 percent among mental health patients at Ndola Central Hospital, based on a retrospective evaluation of data obtained from the Hospital’s psychiatric unit’s medical records on the patients that were admitted from the January 1 to June 30, 2011).
[51] Human Rights Watch interview with Carol A., Lusaka, November 14, 2013.
[52] Human Rights Watch interview with Mercy S., mother of a child with developmental disability, Lusaka, November 14, 2013; Human Rights Watch interview with Alice B., health care volunteer, Lusaka, November 13, 2013; Human Rights Watch interview with Theresa C., mother of a child with intellectual disability, Lusaka, November 15, 2013.
[53] Human Rights Watch interview with Franklyn C., January 21, 2014.
[54] Human Rights Watch interview with Samson B., Livingstone, January 24, 2014.
[55] Ibid.; Human Rights Watch interview with Paul C., who has a psychosocial disability, Lusaka, February 11, 2014; Human Rights Watch interview with Alice B., health care volunteer, Lusaka, November 13, 2013.
[56] Human Rights Watch interview with Sylvester Katontoka, Lusaka, January 30, 2014; Human Rights Watch interview with psychiatric clinical officer, Livingstone, February 7, 2014; Human Rights Watch interview with Friday Nsalamo, Senior Mental Health Officer, Ministry of Health, May 31, 2014; See also Augustus Kapungwe et al., “Mental Illness Stigma and Discrimination in Zambia, African Journal of Psychiatry, 13(2010):192-203, accessed June 1, 2014, http://www.ajol.info/index.php/ajpsy/article/viewFile/57913/46281 (noting that Chainama Hills Hospital is a source of widespread negative attitudes about people with psychosocial disability).
[57] Human Rights Watch interview with Patrick M., Livingstone, January 24, 2014.
[58] Human Rights Watch interview with Susan M., Lusaka, January 27, 2014.
[59] Human Rights Watch interview with Inocente T., Lusaka, November 14, 2013.
[60] Human Rights Watch interview with Leonard C., Lusaka, November 15, 2013.
[61] Human Rights Watch interview with Patrick M., Livingstone, January 24, 2014.
[62] Human Rights Watch interview with Grace M., mother of a child with disability, Lusaka, November 15, 2013.
[63] Human Rights Watch interview with Samson B., Livingstone, January 24, 2014.
[64] Human Rights Watch interview with Justin L., a man with hearing and physical disabilities, Lusaka, November 15, 2013; Human Rights Watch interview with Inocente T., Lusaka, November 14, 2013; Human Rights Watch interview with Chola M., Lusaka, November 12, 2013; Human Rights Watch interview with Doreen L., Livingstone, November 21, 2013.
[65] Human Rights Watch interview with Lusa Kabemba, Zambia National Federation of the Blind, Lusaka, November 14, 2013.
[66] Human Rights Watch interview with Yvone L., Lusaka, November 12, 2013; Human Rights Watch interview with Patrick M., Livingstone, January 24, 2014; Human Rights Watch interview with Jane Chalembwa, Lusaka, November 13, 2013; Human Rights Watch interview with Doreen L., Livingstone, November 21, 2013; Human Rights Watch interview with Dominic Vwalya, Lusaka, January 27, 2014.
[67] Human Rights Watch interview with Yvone L., Lusaka, November 12, 2013.
[68] Human Rights Watch interview with Philip M., Kitwe, January 22, 2014.
[69] Human Rights Watch interview with Michael C., Lusaka, January 29, 2014.
[70] Human Rights Watch interview with Yvone L., Lusaka, November 12, 2013.
[71] Human Rights Watch interview with Gordon K., Kitwe, January 21, 2014.
[72] Human Rights Watch interview with Candice L., Lusaka, November 12, 2014.
[73] Human Rights Watch interview with Bruce A., Livingstone, February 8, 2014.
[74] Human Rights Watch interview with Ruth L., Ndola, November 19, 2014.
[75] Human Rights Watch interview with Lucy B., Lusaka, February 12, 2014.
[76] Human Rights Watch interview with Jacob T., Lusaka,February 14, 2014.
[77] Human Rights Watch interview with Philip M., Kitwe, January 22, 2014; Human Rights Watch interview with Justin L., a man with hearing and physical disabilities, Lusaka, November 15, 2013; Human Rights Watch interview with Yvone L., Lusaka, November 12, 2013.
[78] Human Rights Watch interview with Matthew C., Lusaka, January 27, 2014.
[79] Republic of Zambia, Persons with Disabilities Act, No. 6 of 2012, sec. 17(4).
[80] Human Rights Watch interviews with Mr. Size Zulu, Special Education Officer, Ministry of Education, Science, Vocational Training and Early Education, Lusaka, February 3, 2014; Human Rights Watch interview with Emily B., Special Education Teacher, Livingstone, February 7, 2014. Human Rights Watch interview with special education teachers at Munali High School, January 31, 2014; Human Rights Watch interview with Munamuzunga Sikaulu, Education Specialist, UNICEF, February 14, 2014.
[81] SINTEF, “Living Conditions among People with Activity Limitations in Zambia: A National Representative Study,” http://www.sintef.no/upload/Helse/Levekår%20og%20tjenester/ZambiaLCweb.pdf, p.99.
[82] Human Rights Watch interview with Stephen M., Kitwe, January 21, 2014.
[83] Human Rights Watch interview with home care volunteer, Gertrude C., Lusaka, February 7, 2014.
[84] Human Rights Watch interview with Anita C., Ndola, January 21, 2014.
[85] Human Rights Watch interview with Mr. Nongola, Senior Curriculum Specialist, Peggy Sichone, Curriculum Development Specialist, (Intellectual Disability) and Pauline Luneta, Curriculum Development Specialist (Hearing Impairment) at the Ministry of Education, Science, Vocational Training and Early Education, Lusaka, February 4, 2014.
[86] Human Rights Watch interviews with: Special Education Teachers at Munali High School, Lusaka, January 31, 2014; Mrs. Nasama, Head Teacher, Valley View Primary School, Kitwe, January 21, 2014.
[87] Human Rights Watch interview with Frances L., Lusaka, January 31, 2014.
[88] Human Rights Watch group discussions with 38 deaf children at two special education units in Lusaka and Kitwe and in-depth interviews with six primary and secondary school students with visual and hearing disabilities.
[89]Ibid., Human Rights Watch interview with Mr. Nongola, Senior Curriculum Specialist, Peggy Sichone, Curriculum Development Specialist, (Intellectual Disability) and Pauline Luneta, Curriculum Development Specialist (Hearing Impairment) at the Ministry of Education, Science, Vocational Training and early Education,, Lusaka, February 4, 2014; Human Rights Watch interview with Frances L., Lusaka, January 31, 2014.
[90] Human Rights Watch interviews with staff of Zambia Health Education and Communication Trust (ZHECT), Lusaka, February, 11, 2014.
[91] Human Rights Watch interviews with staff of Zambia Health Education and Communication Trust (ZHECT), Lusaka, February, 11, 2014; Human Rights Watch interview with Mr. Mwiinga Donor-Coordinator and Public Relations Manager, National HIV/AIDS/STI/TB Council, February 29, 2014; Human Rights Watch interview with Dominic Vwalya from the Kanyama Disabled Persons Association, Lusaka, January 27, 2014.
[92] Human Rights Watch interviews with Frank Musukwa Jr, Zambia Deaf Youth and Women, Kitwe, November 19, 2013; James Kapembwa, Zambia National Association of the Deaf (ZNAD), Lusaka, November 14, 2013; Human Rights Watch interview with Julien Mwape, DISSUP, Kitwe, November 19, 2013; Human Rights Watch interview with George Mizinga, from Livingstone Network of Persons Living With Disabilities, November 20, 2013.
[93] Human Rights Watch interview with George Mizinga, from Livingstone Network of Persons Living with Disabilities, November 20, 2013.
[94] Ibid.; Lusa Kabemba, Zambia National Federation of the Blind, November 14, 2013; Mr. Manyando, Head of Special Education, Munali Secondary School, November 14, 2013.
[95] Human Rights Watch interviews with Frank Musukwa Jr, Zambia Deaf Youth and Women, Kitwe, January 21, 2014; Mr. Mbwe, Association of Sign Language Interpreters of Zambia, Lusaka, February 13, 2014; Human Rights Watch interview with Franklyn C., January 21, 2014.
[96] Human Rights Watch interviews with John L., Kitwe, January 21, 2014.
[97] Human Rights Watch interview with Jacob T., Lusaka, February 14, 2014; Human Rights Watch interview with Dominic Vwalya, Lusaka, January 27, 2014; Human Rights Watch interview with Gordon K., Kitwe, January 21, 2014.
[98] Human Rights Watch interview with Jacob T., Lusaka, February 14, 2014.
[99] Human Rights Watch interview with Sharon L., Kitwe, January 21, 2014.
[100] Human Rights Watch interview with nurse in ART department at health center, Lusaka, February 4, 2014; Human Rights Watch interview with Mackenzie Mbewe from Zambia National Association for the Deaf, Lusaka, November 14, 2013; Human Rights Watch interview with Susan M., who is also a VCT counselor, Lusaka, January 27, 2014.
[101] Human Rights Watch interview with Rosemary T., Kitwe, November 19, 2014.
[102] Human Rights Watch interview with Mary Zama, Senior Programme Officer, Population Council (noting the Population Council ‘s support of pilot initiative to provide access to post exposure prophylaxis at Victim Support Units in selected Lusaka districts); Human Rights Watch interview with Royter Choonga-Phiri, Programmes Manager, Raymond Havwala, Men’s Network Coordinator, Young Women’s Christian Association (YWCA), Lusaka, January 29, 2014; Human Rights Watch interview with Mr. T. Kasale, National Coordinator, Victim Support Units, Zambian Police Service, Lusaka, February 10, 2014.
[103] Human Rights Watch interviews with members of Anti-GBV clubs in Kanyama and Chawama compounds in Lusaka, February 10, 2014.
[104] Human Rights Watch interviews with members of Anti-GBV clubs in Kanyama and Chiwama compounds in Lusaka, February 10, 2014; Human Rights Watch interview with Royter Choonga-Phiri, Programmes Manager, Young Women’s Christian Association (YWCA), Lusaka, January 29, 2014; Human Rights Watch interview with Julien Mwape, DISSUP, Kitwe, January 22, 2013.
[105] Republic of Zambia, Anti-Gender Based Violence Act No. 1 of 2011; see Ministry of Gender and Child Development, “National Guidelines for the Multidisciplinary Management of Survivors of Gender-Based Violence,” 2011.
[106] Human Rights Watch interview with Sylvester Katontoka from Mental Health Users Network (MHUNZA), Lusaka, January 30, 2014.
[107] See Alister Munthali et al., “Effective HIV/AIDS and Reproductive Health Information to People with Disabilities,” 2004, http://www.aidsfreeworld.org/Our-Issues/Disability/~/media/04BE2528AA4A41DD9B344E7924397925.pdf (accessed May 18, 2014); Nora Groce et al., “Guidelines for Inclusion of Individuals with Disability in HIV/AIDS Outreach Efforts,” 2006, http://siteresources.worldbank.org/DISABILITY/Resources/280658-1161026944612/HIVGuidelinesENG.doc (accessed May 1, 2014).
[108] Human Rights Watch interviews with George Mizinga, Livingstone Network of Persons Living with Disabilities, November 20, 2013.
[109] Human Rights Watch interview with Dominic Vwalya from the Kanyama Disabled Persons Association, January 27, 2014.
[110] Human Rights Watch interview with Michael C., Lusaka, January 29, 2014.
[111] Human Rights Watch interview with Chola M., Lusaka, November 12, 2013; Human Rights Watch interview with Doreen L., Livingstone, November 21, 2013.
[112] Ministry of Health, “Zambia National Guidelines for HIV Counselling and Testing,” October 2006.
[113] Ministry of Health and National HIV/AIDS/STI/TB Council, “National AIDS Strategic Framework 2011-2015: Joint Mid Term Review Report,” December 2013, p.58 (noting data for 2011). See also Sara Gari et al., “HIV Testing and Tolerance to Gender Based Violence: A Cross-Sectional Study in Zambia,” (2013): accessed May 1, 2014, doi: 10.1371/journal.pone.0071922; Sara Gari et al., “The Critical Role of Social Cohesion on Uptake of HIV Testing and ART in Zambia,”19th International AIDS Conference: Abstract no. TUAC0105 .
[114] Human Rights Watch interview with Paul C., Lusaka, February 11, 2014.
[115] Human Rights Watch interview with Thomas L., Ndola, November 19, 2014.
[116] Human Rights Watch interview with Raymond L., Livingstone, January 24, 2014.
[117] Human Rights Watch interview with Felix B., Livingstone, January 24, 2014.
[118] Ministry of Health, “Zambia National Guidelines for HIV Counselling and Testing,” October 2006, pp. 17-20.
[119] Ibid.
[120] Human Rights Watch interview with Chipo Tembo, Livingstone, February 7, 2014.
[121] Human Rights Watch interview with Mackenzie Mbewe, Zambia National Association for the Deaf, November 14, 2013.
[122] Human Rights Watch interview with Lidia A., Kitwe, January 21, 2014.
[123] Human Rights Watch interview with Edwin B., Kitwe, November 19, 2014; Human Rights Watch interview with Kent M., Lusaka, January 31, 2014.
[124] Ministry of Health, “Zambia National Guidelines for HIV Counselling and Testing,” October 2006, p. 25.
[125] Human Rights Watch interview with Sylvester Katontoka and members [withheld at their request], Mental Health Users Network (MHUNZA), Lusaka, January 30, 2014. Human Rights Watch interview with Ada, Ndola, January 24, 2014.
[126] Human Rights Watch visited two psychiatric units in tertiary hospitals in two provinces and interviewed medical staff from a third psychiatric unit in a third province, at a mobile mental health clinic in a third province.
[127] Ministry of Health, “Adult and Adolescent Antiretroviral Therapy Protocols,” 2010, p.12-13 (noting that mandatory testing is essentially a compulsory test that cannot be refused and “is generally seen as an unsuitable way of combating HIV and AIDS in Zambia, because it restricts freedom of choice, and can result in stigmatization and discrimination for anyone who tests positive”).
[128] Ibid.
[129] Human Rights Watch interview with psychiatrist, February 5, 2014; Human Rights Watch interview with psychiatric clinical officer, February 7, 2014.
[130] Human Rights Watch interview with psychologist, January 21, 2014.
[131] Human Rights Watch interview with clinical psychiatric officer, November 18, 2013.
[132] Human Rights Watch interview with clinical psychiatric officer, January 21, 2014.
[133] Ministry of Health, “Adult and Adolescent Antiretroviral Therapy Protocols, 2010,” p. 13.
[134] See UN Committee on the Rights of Persons with Disabilities, General Comment No 1, Article 12: Equal Recognition Before the Law, CRPD/C/GC/1, 11 April 2014 (“States parties have an obligation to require all health and medical professionals (including psychiatric professionals) to obtain the free and informed consent of persons with disabilities prior to any treatment”; “Under article 12 of the Convention, perceived or actual deficits in mental capacity must not be used as justification for denying legal capacity”).
[135] Mental Health Bill, 2014, Part IX, sec. 31; Part XII, sec. 53 (provisions on consent and legal capacity), Draft Document on file with Human Rights Watch, January 2014); see also CRPD art. 12.
[136] CRPD, art. 25.
[137] World Health Organization, “Antiretroviral Therapy for HIV Infection in Adults and Adolescents: Recommendations for a Public Health Approach,” 2006, http://www.who.int/hiv/pub/guidelines/artadultguidelines.pdf (accessed May 1, 2014), p. 70; Also see WHO, “Consolidated Guidelines on The Use of Antiretroviral Drugs for Treating and Preventing HIV Infection,” http://www.who.int/hiv/pub/guidelines/arv2013/download/en/.
[138] Ibid.
[139] Human Rights Watch interview with Jacob T., Lusaka, February 14, 2014.
[140] Human Rights Watch interview with Chipo Tembo, Livingstone, February 7, 2014.
[141] Human Rights Watch interview with Humphrey L., Kitwe, January 21, 2014.
[142] Human Rights Watch interview with Noreen C., Kitwe, January 21, 2014.
[143] Human Rights Watch interview with Dominic Vwalya, Lusaka, January 27, 2014.
[144] Human Rights Watch interview with Gabriel L., Lusaka, February 13, 2014.
[145] Ibid.
[146] Human Rights Watch interview with Herbert B., Lusaka, February 13, 2014; Human Rights Watch interview with Paul C., Lusaka, February 11, 2014.
[147] Human Rights Watch interviews with psychiatric clinical officers and other health workers in Ndola, Livingstone, and Lusaka; Human Rights Watch interview with Friday Nsalamo, Senior Mental Health Officer, Ministry of Health, May 31, 2014.
[148] Republic of Zambia, Persons with Disabilities Act, 2012, Sec 27(d).
[149] Ibid., sec 28(d).
[150] Ibid., sec 29.
[151] Human Rights Watch interviews with Dominic Vwalya, Kanyama Disabled Persons Association, January 27, 2014; Human Rights Watch interview with Candice L., Lusaka, November 12, 2014; Human Rights Watch interview with Brenda T., Livingstone, February 6, 2014.
[152] Human Rights Watch interview with Dominic Vwalya, Lusaka, January 27, 2014.
[153] Ibid.
[154] Human Rights Watch interview with Candice L., Lusaka, November 12, 2014.
[155] Human Rights Watch interview with Annie who has a physical disability, Livingstone, February 7, 2014; Human Rights Watch interview with Margaret Malumo, Nurse and Counselor, St. Francis Community Integrated Care Programme in Livingstone February 7, 2014; Human Rights Watch interview with Brenda T., Livingstone, February 6, 2014.
[156] See Ministry of Health, “National Mobile HIV Services Guidelines: Reaching out to Remote Communities,” November 2013, (noting the expansion of mobile ART services, with a particular focus on rural and remote communities.) The Guidelines do not address the requirements for the provision of inclusive services for people with different disabilities.
[157] Human Rights Watch interview with Ruth L.,Ndola, January 24, 2014.
[158] Ministry of Health, “Adult and Antiretroviral Therapy Protocols,” 2010, p.41.
[159] Ibid.
[160] CRPD, art. 2.
[161] Human Rights Watch interview Dr. David M., Lusaka, November 11, 2014.
[162]WHO, “Consolidated Guidelines on The Use of Antiretroviral Drugs for Treating and Preventing HIV Infection,” http://www.who.int/hiv/pub/guidelines/arv2013/download/en/, p.178.
[163] Ibid.; Victor Musiime et al., “An Adolescent Peer Support Group Improves Adherence to Antiretroviral Therapy and Reduces Self Stigma among HIV Infected Adolescents at Joint Clinical Research Centre (JCRC), Kampala,” 4th IAS Conference on HIV Pathogenesis, Treatment and Prevention: Abstract no. CDB446.
[164] Human Rights Watch interview with Elizabeth, sister of Miriam who has an intellectual disability, Livingstone, January 24, 2014.
[166] Human Rights Watch interview with Candice L., Lusaka, November 12, 2014.
[167] Human Rights Watch interview with Lucy B., Lusaka, February 12, 2014; Human Rights Watch interview with Noreen C., Kitwe, January 21, 2014.; Human Rights Watch interview with Linda T., caregiver of child with visual disability, Lusaka, February 12, 2014.
[168] Human Rights Watch interview with Lucy B., Lusaka, February 12, 2014.
[169] Human Rights Watch interview with Pastor Tembo, Kitwe, January 22, 2014.
[170] Human Rights Watch interview with Noreen C., Kitwe, January 21, 2014.
[171] Ibid.
[172] See Human Rights Watch, A Question of Life or Death. Treatment Access for Children Living With HIV in Kenya, 2008, http://www.hrw.org/reports/2008/12/15/question-life-or-death-0; “Kenya: Support Disclosure of HIV Status to Children,” Human Rights Watch news release, December 1, 2010, http://www.hrw.org/news/2010/12/01/kenya-support-disclosure-hiv-status-children.
[173] Human Rights Watch interview with Noreen C., Kitwe, January 21, 2014; Human Rights Watch interview with Daniel L., a deaf boy who is on ART, Lusaka, February 14, 2014; Human Rights Watch interview with in-charge (name withheld) at orphanage for children from HIV affected households in Lusaka, November 11, 2013.
[174] See Ministry of Health, “Adolescent Health Strategic Plan 2011-2015,” undated, http://countryoffice.unfpa.org/zambia/drive/ZambiaAdolescentHealthStrategicPlan2011-2015.pdf, (accessed June 10, 2014), p.27.
[175] Ibid., p.19.
[176] Ibid., p.29.
[177] Central Statistical Office, “Living Conditions Monitoring Survey Report 2006 & 2010,” http://www.zamstats.gov.zm/report/Lcms/2006-2010%20LCMS%20Report%20Final%20Output.pdf, p. 180.
[178] Ibid.; SINTEF, “Living Conditions among People with Activity Limitations in Zambia: A National Representative Study,” http://www.sintef.no/upload/Helse/Levekår%20og%20tjenester/ZambiaLCweb.pdf. (accessed June 5, 2014).
[179] Human Rights Watch interview with Erica M., February 7, 2014.
[180] Human Rights Watch interview with Elizabeth, sister of Miriam who has an intellectual disability, Livingstone, January 24, 2014, Human Rights Watch interview with Chipo Tembo, Livingstone, February 7, 2014; Human Rights Watch interview with Mackenzie Mbewe, Zambia National Association for the Deaf, Lusaka, November 14, 2013.
[181] World Food Programme, WHO, UNAIDS, “Policy Brief: HIV, Food Security and Nutrition,” May 2008, http://data.unaids.org/pub/Manual/2008/JC1515_policy_brief_nutrition_en.pdf (accessed June 10, 2014).
[182] UNAIDS, “UNAIDS HIV and AIDS Estimates 2012,”http://www.unaids.org/en/regionscountries/countries/zambia/.
[183] See Human Rights Watch, A Question of Life or Death. Treatment Access for Children Living With HIV in Kenya; USAID AIDS Support and Technical Assistance Resources (AIDSTAR-One), “Protecting Children Affected By HIV Against, Abuse, Exploitation, And Neglect,” July 2011, http://www.aidstar-one.com/sites/default/files/AIDSTAR-One_Report_OVC_Child%20Protection.pdf (accessed June 10, 2014).
[184] Human Rights Watch interview with Angela L., Lusaka, November 13, 2013.
[185] Human Rights Watch interview with in-charge (name withheld) at orphanage for children from HIV affected households in Lusaka, November 11, 2013.
[186] Ibid.; Human Rights Watch interview with Emanuel B., Lusaka, November 16, 2013.
[187] Human Rights Watch interview with Pastor Michael, Lusaka, February 14, 2014; Human Rights Watch interview with Daniel L., Lusaka, February 14, 2014.
[188] Ibid.
[189] Human Rights Watch interview with Nandi Banda, Lusaka, January 31, 2014.
[190] Central Statistical Office, “National Demographic and Health Survey (DHS) 2007,” March 2009, http://countryoffice.unfpa.org/zambia/drive/2007_zdhs_final_report.pdf (accessed May 1, 2014), p. 283; See, D. Brown et al., “Exposure to Physical and Sexual Violence and Adverse Health Behaviours in African Children: Results From the Global School-Based Student Health Survey,” Bulletin of the World Health Organisation, 87 (2009):447-455, accessed May 18, 2014, doi: 10.2471/BLT.07.047423.
[191] Ibid., p. 286.
[192] Human Rights Watch interviews with: medical staff at Child Sexual Abuse (CSA) One Stop Centers at University Teaching Hospital, Lusaka, February 5, 2014 and Livingstone General Hospital, Livingstone, February 7, 2014; Human Rights Watch interview with Betty L., Police Officer at Victim Support Unit, Lusaka, February 10, 2014.
[193] Human Rights Watch interview with Janet K., Lusaka, February 5, 2014.
[194] Human Rights Watch interview with Margret M, Livingstone, January 24, 2014.
[195] Human Rights Watch interview with Malala C., Livingstone, February 6, 2014.
[196] Human Rights Watch interview with Elizabeth, sister of Miriam who has an intellectual disability, Livingstone, January 24, 2014; Human Rights Watch interview with Alice B., health care volunteer, Lusaka, November 13, 2013; Human Rights Watch interview with home care volunteer, Gertrude C., Lusaka, February 7, 2014.
[197] Human Rights Watch interview with Sarah L., Livingstone, January 24, 2014.
[198] Human Rights Watch interview with Brenda T., Livingstone, February 6, 2014.
[199] Human Rights Watch interview with Betty L., Police Officer at Victim Support Unit, Lusaka, February 10, 2014.
[200] Human Rights Watch interview with Erica M., February 7, 2014.
[201] Human Rights Watch interviews with Patience L., Livingstone, January 24, 2014.
[202] Human Rights Watch interviews with: medical staff at Child Sexual Abuse (CSA) One Stop Centers at University Teaching Hospital, Lusaka, February 5, 2014 and Livingstone General Hospital, Livingstone, February 7, 2014; Zambia is planning to expand the number of Stop Centers for survivors of gender based violence – these centers provide integrated health and psychosocial services and police and justice response in the one physical location. See Elwyn Chomba et al., “Integration of Services for Victims of Child Sexual Abuse at the University Teaching Hospital One-Stop Centre,” Journal Tropical Medicine, 2010 (2010): accessed May 1, 2014, doi: 10.1155/2010/864760.
[203] Human Rights Watch interview with Royter Choonga-Phiri, Programmes Manager, Young Women’s Christian Association (YWCA), Lusaka, January 29, 2014.
[204] Human Rights Watch interview with Margaret Malumo, Nurse and Counselor, St. Francis Community Integrated Care Programme in Livingstone, Livingstone, November 21, 2013; Human Rights Watch interview with Jennifer T., mother of 16-year-old daughter with intellectual disability, Lusaka, February 12, 2014; Human Rights Watch interview with Agnes C., mother of 13-year-old daughter with epilepsy and intellectual disability, Lusaka, February 12, 2014.
[205] International Covenant on Civil and Political Rights (ICCPR), adopted December 16, 1996, G.A. Res. 2200A (XXI), 21 U.N. GAOR Supp. (No. 16) at 52, U.N. Doc. A/6316 (1966), 999 U.N.T.S. 171, entered into force March 23, 1976, acceded to by Zambia on April 10, 1984.
[206] International Covenant on Economic, Social and Cultural Rights (ICESC), G.A. res. 2200A (XXI), U.N. Doc. A/6316 (1966), entered into force January 3, 1976, acceded to by Zambia on April 10, 1984.
[207] Convention on the Elimination of Discrimination against Women (CEDAW), adopted December 18, 1979 by G.A. resolution 34/180, entered into force on September 3, 1981, acceded to by Zambia on June 21, 1985.
[208] Convention on the Rights of the Child (CRC), G.A. res. 44/25, annex, 44 U.N. GAOR Supp. (No. 49) at 167, U.N. Doc. A/44/49 (1989), entered into force September 2, 1990, acceded to by Zambia on December 6, 1991.
[209] Convention on the Rights of Persons with Disabilities (CRPD), adopted December 13, 2006 by G.A. Res. 61/106, Annex I, U.N. GAOR, 61st Sess., Supp. No. 49 at 65, U.N. Doc A/61/49 (2006), entered into force May 3, 2008, U.N. Doc. A/61/61, ratified by Zambia on February 1, 2010. The optional protocol gives individuals the ability to submit complaints to the Convention’s monitoring body after they have exhausted all national redress mechanisms in their countries.
[210] African [Banjul] Charter on Human and Peoples’ Rights, adopted June 27, 1981, OAU Doc. CAB/LEG/67/3 rev. 5, 21 I.L.M. 58 (1982), entered into force October 21, 1986, ratified by Zambia on January 10, 1984.
[211] Protocol to the African Charter on Human and Peoples' Rights on the Rights of Women in Africa (the Maputo Protocol), adopted July 11, 2003, entered into force November 2005, ratified by Zambia on May 2, 2006.
[212] African Charter on the Rights and Welfare of the Child, OAU Doc. CAB/LEG/24.9/49 (1990), ratified by Zambia on December 2, 2008.
[213] Universal Declaration of Human Rights, adopted December 10, 1948, G.A. Res. 217A(III), U.N. Doc. A/810 at 71 (1948), art. 25(1); ICESCR, art. 12. The right to health is also protected under a number of other international human rights treaties and commitments that bind Zambia. The CRC obligates states to “recognize the right of the child to the enjoyment of the highest attainable standard of health and to facilities for the treatment of illness and rehabilitation of health. States Parties shall strive to ensure that no child is deprived of his or her right of access to such health care services.” CRC, art. 24. The right to the health is recognized by the International Convention on the Elimination of All Forms of Racial Discrimination and in CEDAW, arts. 11.1(f), 12 and 14(2)(b). The right to health has been proclaimed by the Commission on Human Rights, the Vienna Declaration and Programme of Action of 1993 and other international instruments. UN Committee on Economic, Social and Cultural Rights, “Substantive Issues Arising in the Implementation of the International Covenant on Economic, Social and Cultural Rights,” General Comment No. 14, the Right to the Highest Attainable Standard of Health, E/C.12/2000/4 (2000), http://www.unhchr.ch/tbs/doc.nsf/0/40d009901358b0e2c1256915005090be?Opendocument (accessed June 20, 2014), para. 2.
[214] ICESCR, art. 12.
[215] Committee on Economic, Social and Cultural Rights, General Comment No. 14: The Right to the Highest Attainable Standard of Health, E/C 12/2000/4, (2000), para. 12.
[216] Ibid.
[217] CRPD, art. 25.
[218] Ibid.
[219] Ibid.
[220] Women’s Protocol, art. 14; CRPD, art. 25.
[221] CRPD, art. 9.
[222] African Charter, art. 16., The African Charter on Human and Peoples’ Rights (African Charter) guarantees the right to health and requires governments to “take the necessary measures to protect the health of their people and to ensure that they receive medical attention when they are sick.”; See Southern African Development Community (SADC) Protocol on Gender and Development, art. 26.
[223] African Charter, art. 18.
[224] SADC Protocol on Health in the Southern African Development Community, 1999, art. 15.
[225] SADC Sexual and Reproductive Health Strategy for the SADC Region, 2006 – 2015, p. 15.
[226] Human Rights Council, Rights of the Child: the Right of the Child to the Enjoyment of the Highest Attainable Standard of Health, A/HRC/22/L.27, Para. 17.
[227]Ibid.
[228] Committee on the Rights of the Child, General Comment No. 3: HIV/AIDS and the Rights of the Child, para. 18.
[229] Committee on the Rights of the Child, General Comment No. 9: The Rights of Children with Disabilities, para. 59.
[230] CRPD art. 24 (b).
[231] CRPD art. 24 (3) (a).
[232] UN Committee on Economic, Social and Cultural Rights, General Comment No. 14: The Right to the Highest Attainable
Standard of Health, paras. 4, 11; CRC art. 24.
[233] UN Committee on Economic, Social and Cultural Rights, General Comment No. 14: The Right to the Highest Attainable
Standard of Health, para. 43b.
[234] Committee on the Rights of the Child, General Comment No. 3: HIV/AIDS and the Rights of the Child, para. 28; See Office of the United Nations High Commissioner for Human Rights and the Joint United Nations Programme on HIV/AIDS, “International Guidelines on HIV/AIDS and Human Rights,” http://data.unaids.org/publications/irc-pub07/jc1252-internguidelines_en.pdf, para.26.
[235] UN General Assembly Resolution, “2011 Political Declaration on HIV/AIDS: Intensifying Our Efforts to Eliminate HIV and AIDS,”A /RES/65/277, 8 July 2011, http://www.unaids.org/en/media/unaids/contentassets/documents/document/2011/06/20110610_un_a-res-65-277_en.pdf (accessed June 10, 2014), para. 20.
[236] ICESCR, art. 2 (1). ICCPR, art. 2(1). CEDAW, art. 5. CRC, art. 2 (1). ACHPR, art. 18 (4) and 28.
[237] CRPD, art. 3(b).
[238] CRPD, art. 2.
[239] CRPD. art. 5.
[240]CRPD. art. 12.
[241] CRPD. art. 8.
[242] CESCR, General Comment No. 14, para 12(b).
[243] CRPD, art. 25.
[244] Office of the United Nations High Commissioner for Human Rights and the Joint United Nations Programme on HIV/AIDS, “International Guidelines on HIV/AIDS and Human Rights,” http://data.unaids.org/publications/irc-pub07/jc1252-internguidelines_en.pdf, para.60(j).
[245] Southern African Development Community, “Regional Minimum Standards for Harmonised Guidance on HIV Testing and Counseling in the SADC Region,” November 2010, https://www.k4health.org/sites/default/files/HTC%20Minimum%20Standards%20reviewed%206%20JUNE%2011-1.pdf, (accessed July 2, 2014), Sec. 5.4.
[246] CRPD art. 6.
[247] CESCR, General Comment No. 14, para 14.
[248] CRPD, art. 2.
[249] Ibid.
[250] CRPD, art. 20.
[251] World Bank and World Health Organization, “World Report on Disability,” http://whqlibdoc.who.int/publications/2011/9789240685215_eng.pdf, p.74; World Health Organization, “Fact Sheet N°352: Disability and Health,” September 2013, http://www.who.int/mediacentre/factsheets/fs352/en/ (accessed July 2, 2014).
[252] Ibid.
[253] CRPD art. 21.
[254] CRPD art. 26.
[255] CRPD art. 22.
[256] Constitution of the Republic of Zambia (1991, amended 1996), The Laws of Zambia, 1996, http://www.parliament.gov.zm/downloads/VOLUME%201.pdf (accessed June 30, 2014) art. 112.
[257] Ibid., art. 23.
[258] See ‘First Draft Constitution’ released by the Technical Committee on Drafting the Zambian Constitution (TCDZC), April 30, 2010, http://zambianconstitution.org/downloads/First%20Draft%20Constitution.pdf, (accessed June 30, 2014).
[259]
The Persons with Disabilities Act, No. 6 of 2012, http://www.zambialii.org/files/zm/legislation/act/2012/6/The%20Persons%20with%20disabilities%20act,%202012%20(1).PDF
(accessed June 5, 2014).
[260] Ibid., art. 6.
[261] Ibid., art. 7.
[262] Ibid., art. 8.
[263] Ibid., arts. 20, 21.
[264] Ibid., arts. 22, 23.
[265] Ibid., art. 27-31.
[266] Ibid., art. 32.
[267] Ibid., arts. 35,36.
[268] Ibid., art. 8(1).
[269] Ibid., art. 40.
[270] Ibid., arts. 11-19.
[271] Ibid. art. 27 (a).
[272] Ibid. arts. 28, 29.
[273] Ministry of Community Development, Mother and Child Health, “National Policy on Disability: Empowering Persons with Disabilities,” 2012 Draft, p.14.
[274] Ibid.
[275] UNAIDS, “2011-2015 Strategy: Getting to Zero,” 2010, http://www.unaids.org/en/media/unaids/contentassets/documents/unaidspublication/2010/jc2034_unaids_strategy_en.pdf (accessed May 18, 2014), p.34.
[276] 2011 Political Declaration on HIV/AIDS: Intensifying Our Efforts to Eliminate HIV and AIDS, UN General Assembly Resolution, A /RES/65/277, 8 July 2011, http://www.unaids.org/en/media/unaids/contentassets/documents/document/2011/06/20110610_un_a-res-65-277_en.pdf (accessed June 10, 2014) para. 31.
[277] African Union, “Continental Policy Framework on Sexual and Reproductive Health and Rights,” 2006, http://pages.au.int/carmma/documents/continental-policy-framework-sexual-and-reproductive-health-and-rights (accessed May 18, 2014), pp.28.
[278] National HIV/AIDS/STI/TB Council, “National AIDS Strategic Framework 2011-2015: Towards Improving the Quality of Life of the Zambian People,” http://www.aidstar-one.com/sites/default/files/prevention/resources/national_strategic_plans/Zambia%20NASF%202011-2015.pdf, p.48.
[279] Ibid.
[280] Ministry of Health, “National Health Strategic Plan: Towards Attainment of Health Related Millennium Development Goals and Other National Health Priorities in a Clean, Caring and Competent Environment, 2011-2015,” http://www.nationalplanningcycles.org/sites/default/files/country_docs/Zambia/zambia_nhsp_2011-2015_.pdf (accessed June 5, 2014).
[281] Republic of Zambia, “Fifth National Development Plan 2006-2010: Broad Based Wealth and Job Creation Through Citizenry Participation and Technological Advancement,” (requiring the government to: “increase access to HIV and AIDS counselling and testing, in health facilities and at community level including special groups such as the disabled”; “define appropriate sizes and types of health facilities for the different levels of care which can also cater for the needs of the physically disabled”; and stating: “deliberate and effective interventions will be put in place to accelerate progress during the FNDP towards the attainment of the rights and needs of persons with disabilities.”) http://www.thegef.org/gef/sites/thegef.org/files/documents/ZAMBIA-FNDP.pdf (accessed June 5, 2014), pp. 167, 169, 204; Republic of Zambia, “Sixth National Development Plan 2011-2015: Sustained Economic Growth and Poverty Reduction, http://www.mofnp.gov.zm/jdownloads/National%20Development%20Plans/Sixth%20National%20Development%20Plan/sixth_national_development_plan_-_full_volume.pdf (accessed June 5, 2014), pp.33-35; 87-88; The government has developed a revised Sixth National Development Plan (2013-2016), with a greater focus on social protection.
[282] Human Rights Watch interview with Dr. Felix Silwimba, Director General, Zambia Agency for Persons with Disabilities, Lusaka November 8, 2013; Human Rights Watch interview with Mr. Michelo, Social Welfare Director, Ministry of Community Development, Mother and Child Health, Lusaka, February 4., 2014.
[283] See “The Global Fund TB and HIV Concept Note,” Draft Document, May 2014, p.27 (noting that “The role of the Ministry of Health in the realigned health care system is to provide overall health sector policy development, research and development, disease surveillance, oversight of training institutions, the setting of standards and performance audits, as well as level II to level IV health services” and “The first level health facilities such as health centres, health posts, community health services, and District Hospitals and District Medical Offices fall under the MCDMCH”).
[284] Human Rights Watch interview with Mr. S.Michelo, Social Welfare Director, Ministry of Community Development, Mother and Child Health, Lusaka, February 4, 2014; See Ministry of Community Development, Mother and Child Health, “National Policy on Disability: Empowering Persons with Disabilities,” September 2012 Draft.
[285] Human Rights Watch interview with Gizepe Chakulunta, Focal Point for HIV and AIDS, Ministry of Home Affairs, February 7, 2014; Human Rights Watch interview with Dr. Witola, Director of Programmes,, National HIV/AIDS/STI/TB Council, January 29, 2014.
[286] Human Rights Watch interviews with Serah Brotherton, Director, ZAFOD, January 27, 2014; Human Rights Watch interview with Julien Mwape, DISSUP, Kitwe, November 19, 2013; Human Rights Watch interview with Dr. Felix Silwimba, Director General, Zambia Agency for Persons with Disabilities, Lusaka November 8, 2013.
[287] Human Rights Watch interviews with Serah Brotherton, Director, ZAFOD, January 27, 2014; Human Rights Watch interview with Felix Mwanza, Clever Chilende, Treatment Advocacy and Literacy Campaign (TALC), February 4, 2014.
[288] See “The Global Fund TB and HIV Concept Note,” Draft May 2014 (noting that “GRZ contribution towards funding the national strategies … stands at 8%.”), p.12; See UNAIDS Programme Coordinating Board Field Visit to Zambia, November 2013, http://www.unaids.org/en/media/unaids/contentassets/documents/pcb/2013/20131106_PCB-field-visit-Zambia_en.pdf (accessed June 5, 2014), p.6; According to the National HIV/AIDS/STI/TB Council, this representation of the government’s expenditure does not take into account its expenditure on operational, infrastructure and capital costs associated with the HIV response. Human Rights Watch interview with Dr. Witola, Director of Programmes, National HIV/AIDS/STI/TB Council, Lusaka, May 28, 2014.
[289] See Partnership Framework Between the Government of the Republic of Zambia, Ministry of Finance and National Planning and Ministry of Health and the Government of the United States of America, “To Support Implementation of the Zambian National HIV and AIDS Response 2011-2015,” http://www.pepfar.gov/documents/organization/153133.pdf (accessed June 5, 2014) p.5.
[290] PEPFAR, “Zambia Operational Plan Report FY 2012,” undated, http://www.pepfar.gov/countries/cop/2012/ (accessed July 2, 2014), p. 5.
[291] UNAIDS, “UNAIDS Programme Coordinating Board Field Visit to Zambia,” November 2013, http://www.unaids.org/en/media/unaids/contentassets/documents/pcb/2013/20131106_PCB-field-visit-Zambia_en.pdf (accessed June 30, 2014), p.6.
[292] Ibid.
[293] See PEPFAR, “Zambia Operational Plan Report FY 2012,” http://www.pepfar.gov/documents/organization/212853.pdf; See PEPFAR, “Technical Considerations: Provided by Technical PEPFAR Working Groups for FY 2014 COPS and ROPS,” http://www.pepfar.gov/documents/organization/217761.pdf (noting that “Where possible it is envisioned that wider PEPFAR programming be inclusive of disabled people and disability issues, so that HIV/AIDS prevention and treatment outcomes can be improved for all people, including disabled people. However, this should not preclude disability-specific interventions where appropriate (for example, to reach disabled people who might not otherwise be included in HIV/AIDS prevention, treatment, care and support activities.”); see Global Fund Grant Portfolio: Zambia, 2013, http://portfolio.theglobalfund.org/en/Country/Index/ZMB (accessed June 5, 2014).
[294] Human Rights Watch interview with Frank Musukwa, Zambia Deaf Youth and Women, on November 19, 2013 and follow-up discussions in February and June 2014.
[295] Ibid. VCT training for the deaf counselors was provided by staff from the Society for Family Health, University Teaching Hospital in Lusaka and the Buchi Clinic in Kitwe. The Open Society Foundation Initiative for Southern Africa (OSISA) is the major donor for the program. The program is also supported by the Kitwe District Medical office and the District AIDS Task Force.
[296] Ibid. The program has been supported by awareness-raising through mobile VCT and community based initiatives including drama performances in community and healthcare settings by a deaf drama troupe on the difficulties faced by deaf persons in accessing sexual and reproductive health and HIV services.
[297] Human Rights Watch discussions with Sister Mary Courtney, Project Coordinator, and Margaret Malumo, Nurse and Counselor, St. Francis Community Integrated Care Programme in Livingstone in November 2013 and in February and May 2014. Human Rights Watch interviews with clinical psychiatric officers from Livingstone General Hospital at mobile clinics in November 2013 and May 2014.
[298] See Zimbabwe Sexual and Reproductive Health Sign Language Dictionary, http://catalogue.safaids.net/sites/default/files/publications/ZimbabweHIVSignLanguageDictionary_2013.pdf (accessed 12 June, 2014); Open Society Initiative for Southern Arica website, Rights Boost for Zimbabwe’s Deaf, at http://www.osisa.org/hiv-and-aids/zimbabwe/rights-boost-zimbabwes-deaf (accessed 12 June, 2014). Development of the dictionary was supported by the European Union, the Open Society for Southern Africa (OSISA) and the Southern Africa HIV and AIDS Information Dissemination Service (SAFAIDS).
[299] See Rebecca Johns and Ray Lazarus, “Taking the Test: HIV Counselling and Testing for People with Intellectual Disability. Practical and Ethical Guidelines for Healthcare and Support Workers,” undated, http://wcfid.co.za/resources-3/ (accessed July, 2, 2014); The Western Cape Forum for Intellectual Disability is a network of over 150 organizations providing services for people with intellectual disabilities in the Western Cape province of South Africa.