Hidden in the Mealie Meal
Gender-Based Abuses and Women's HIV Treatment in Zambia
I. Summary
I started [HIV] medication in 2006.[My husband] does not know.I take the medicine out of a bottle and put it in a plastic [bag] or in a paracetamol box . Sometimes I would miss a dose; he comes back at 18:00 hrs, drunk, closes the door and says, "Today you are going to freak out."He locks [me] in, he beats me up and locks me out of the house . I go to the neighbors, if they have mercy they will let [me] in, if not, [I] sleep under a tree until tomorrow.As a result of that I miss doses sometimes.I feel very bad. I don't even feel like taking the medicine.
-Berta K., Lusaka, February 3, 2007
Zambia is one of many countries setting ambitious targets for rapidly scaling up antiretroviral treatment for HIV/AIDS and is making impressive progress. It is addressing a range of obstacles to treatment and receiving substantial donor support to overcome them. However, women's unequal status in Zambian society gravely undermines their ability to access and adhere to antiretroviral treatment (ART), and the government is paying little if any attention to the gender dimension of treatment, especially the impact of entrenched discrimination and gender-based violence and abuse.
Women in Zambia report that gender-based human rights abuses are, in fact, very real barriers to accessing and adhering to treatment.HIV programs, activists, and policy makers are increasingly recognizing that discrimination and violence against women must be addressed if the world is to combat the AIDS pandemic.But treatment policies and programs still tend to ignore the connection between domestic violence or women's insecure property rights and their ability to seek, access, and adhere to HIV treatment.Although the Zambian government has taken some steps to address violence and discrimination against women generally, major gaps remain in legislation, HIV treatment programs, and support services to address poverty among women living with HIV/AIDS. This must change if HIV treatment is to be provided equitably and to succeed in saving women's lives.
Human Rights Watch investigated the negative impact of gender-based human rights abuses on women's access and adherence to HIV treatment in two provinces in Zambia, Lusaka and the Copperbelt, in 2006 and 2007. Women there told Human Rights Watch how beatings and rapes by their intimate partners, emotional and verbal abuse, loss of property upon divorce or death of a spouse, and fear of such abuses affected their access and adherence to HIV treatment. The abuses thwarted their ability to seek HIV information and testing, discouraged them from disclosing their HIV status to partners, delayed their pursuit of treatment, and hampered their ability to adhere to HIV treatment regimens. Many women, fearing abuse or abandonment, fabricated excuses for their absence from home during clinic visits or support group sessions and hid their medication in flower pots, holes in the ground, food containers, and elsewhere. Many struggled to find money for food, transport to clinics, and diagnostic tests, especially those whose property was taken when divorced, abandoned, or widowed. Some missed doses as a result. The strain took a toll on many, like Berta K., who told us that due to repeated abuse by her partner, "I miss doses sometimes. I feel very bad. I don't even feel like taking the medicine. I say, 'Ha, let me die.'"
Though gender-based abuses have seriously undermined their ability to get HIV treatment, most of the women Human Rights Watch interviewed said their difficulties are simply not discussed in the clinics where they go for HIV counseling or medicine. With few exceptions, health care providers did not raise the issue.Some of the institutions that train HIV counselors in Zambia told us "gender is integrated" into their training. Yet most of the dozens of HIV counselors Human Rights Watch interviewed said they do not screen for gender-based abuses, offer referrals for services, discuss safety strategies with patients, assess how this impacts treatment, or otherwise address the abuses. Treatment adherence counselors said they count women's remaining pills and discuss certain other obstacles to adherence, but not gender-based abuses. Almost all, however, expressed willingness to start dealing with these abuses with proper training and support.
There is perhaps no better place than Zambia to create a model approach to responding to gender-based human rights abuses within HIV treatment programs as part of an overall strategy to prevent and address these abuses. Situated in Southern Africa, the region most affected by the pandemic, 17 percent of Zambia's adult population is living with HIV/AIDS, and of these, 57 percent are women. Zambia also has high rates of gender-based violence.Recent surveys have found that more than half of women surveyed reported beatings or physical mistreatment since age 15, and one in six women reported having been raped.
On the positive side the government has enacted laws to protect women's property rights, has established specialized police units to address gender-based abuses, and in 2006 appointed a cabinet minister for gender and development. Civil society organizations provide services for women survivors of abuse and adults and children living with HIV/AIDS. The country has high-level governmental and multi-sectoral bodies working on HIV/AIDS, and is commended globally for its fight against the epidemic. It has pledged to make HIV treatment and related tests free in the public health system and has increased the number of people on treatment over 30-fold in five years. However, almost half of all individuals in need of treatment are still not getting it. Increasing donor support for its HIV/AIDS response puts Zambia in the spotlight, including as one of 15 focus countries for the United States President's Emergency Plan for AIDS Relief.
Zambia has also ratified major regional and international treaties that require the government to eliminate violence and discrimination against women and to guarantee their rights to health, physical security, non-discrimination, and life. It has also committed to fulfill the United Nations (UN) Millennium Development Goals, which include promoting gender equality, empowering women, and combating HIV/AIDS. To safeguard women's rights and dignity, and to ensure the success of HIV treatment programs, Zambia must turn these commitments into concrete action.
Human Rights Watch calls on the Zambian government to strengthen its response to HIV/AIDS by safeguarding women's human rights, ensuring equitable access to antiretroviral therapy (ART), and providing women on ART access to healthcare services designed to help them deal with gender-based abuses as part of their treatment.In this effort the Zambian government should act urgently to enact and enforce legislation on sexual and gender-based violence.The government should ensure that the new constitution currently under debate guarantees women's equality in all respects, including matters relating to personal and customary laws.And the government should ensure that health care providers working in the areas of HIV/AIDS and ART receive adequate training, clear guidelines, and support to detect and address gender-based abuses. It should improve health care infrastructure, including by ensuring that HIV counseling occurs in a private setting, where women and their healthcare providers can discuss the existence or risk of gender-based abuses.
Donor agencies should support these reforms as a priority, endorsing them as a necessary component of effective treatment for women with HIV/AIDS.
This is a dynamic moment of opportunity and risk in the global fight against HIV/AIDS. Governments and international agencies are pressing to achieve universal access to HIV prevention, treatment, care, and support by 2010. Donors are spending tens of billions of dollars to support HIV treatment.The number of individuals on HIV treatment worldwide jumped from 400,000 in 2003 to more than two million in 2006, and millions more will seek testing for HIV infection and start treatment in the next few years. Without urgent attention to gender-based abuses, Zambia will not realize the potential for these efforts, and the lives of many women will be at risk.
II. Key Recommendations to the Government of Zambia and Zambia National Assembly
To the President of the Republic of Zambia
- Publicly denounce gender-based abuses, including gender-based violence, property grabbing, and unequal distribution of marital property upon divorce, and emphasize the harmful effect of these abuses on HIV treatment.
- Publicly express support for initiatives to redress gender-based abuses.
To the Zambia National Assembly
- Ensure that as the draft constitution is finalized, provisions on equality before the law regardless of sex, and provisions prohibiting any law, culture, custom, or tradition that undermine the dignity, welfare, interest or status of women or men are retained in the final version.
- Adopt specific legislation to prevent and remedy sexual and domestic violence. This should include civil and criminal judicial remedies, and the provision of services to survivors.
To the Ministry of Justice and the Gender in Development Division
- Support efforts to review and transform discriminatory aspects of customary law.
To the Cabinet Committee on AIDS, the National AIDS Council, the Ministry of Health, and the Gender in Development Division
Facilitate the establishment and implementation of programs in the healthcare system to address gender-based abuses, as follows:
Establish a multi-sectoral taskforce that would study different models for addressing gender-based abuses in health settings (see Appendix II), devise a model that is effective and appropriate for Zambia, pilot it, and implement it in the nine provinces.
Integrate initiatives addressing gender-based abuses, especially gender-based violence, into ART and HIV programs.
Ensure that HIV treatment adherence counselors integrate screening for and handling of gender-based violence in counseling, establish protocols on detecting and addressing gender-based violence, and provide continuous supervision and support for counselors to assist them in doing so.
To the Ministry of Health and the Zambia Counseling Council
- Ensure that institutions providing training for HIV counselors cover the issues of gender-based violence, lack of legal protection for women's property rights, and other gender-based abuses and their effect on treatment in training courses.
To the Ministry of Health
- Monitor and document the impact of gender-based abuses on ART in on-going research on ART in Zambia.
To the Gender in Development Division
- Lead on the development of a campaign that emphasizes women's right to decide when, where, and how to seek health services, including access to HIV testing and treatment programs.
To the Ministry of Home Affairs
- Ensure the provision of adequate resources and training for the Victim Support Unit (VSU) including vehicles, sexual crime kits, stationery, and appropriate training and supervision for all VSU officers.
To The Ministry of Community Development and Social Services
- Establish shelters and other relevant services for survivors of gender-based violence in all provinces, and provide additional funding for existing Young Women's Christian Association shelters.
III. Methodology
This report is based on field research conducted in January and February 2007 and in May 2006 by a Human Rights Watch researcher and a consultant.
Human Rights Watch conducted one-on-one interviews with 83 women living with HIV/AIDS, most of whom were survivors of domestic violence or have experienced property grabbing or loss of marital property upon divorce. Many of the women were on antiretroviral therapy (ART). Their ages ranged from 17 to 74, with the majority between 25 and 55 years. One interviewee testified on behalf of her bed-ridden sister. We also conducted two mixed-gender focus group discussions and one women-only focus group discussion with members of HIV support groups in Lusaka and Chongwe. We identified and contacted informants through women's groups and HIV support groups and organizations, and also used the snowball technique where women we interviewed introduced us to other women in their social networks or support groups whose experiences were relevant to our research.The interviews took place in private rooms at NGOs premises, informants' houses, support groups meeting rooms, and in a meeting room at a hotel.
Interviews were conducted in English, Bemba, and Nyanja with the help of two female professional translators and a female coordinator of a support group. Prior to each interview we informed participants of the purpose of the interview, its voluntary nature, and the way in which the data would be collected and used. Researchers assured participants of confidentiality and obtained informed verbal consent from them. Care was taken with survivors to ensure that recounting their experience did not further traumatize them or put them at physical risk. We provided each interviewee with a list of local nongovernmental organizations and clinics that provided relevant services.
Human Rights Watch also interviewed over 25 HIV/AIDS counselors and nurses, in addition to representatives of nongovernmental organizations specializing in women's rights, HIV/AIDS or development, faith-based groups, and traditional health practitioners. At the governmental level we interviewed representatives from the Ministry of Health, the National AIDS Council, the Gender in Development Division, the Ministry of Finance, the Ministry of Justice, the Zambia Permanent Human Rights Commission, and the Victim Support Unit of the police. We also interviewed the First Lady of Zambia, bilateral donors, the World Bank, and UN agencies. Researchers conducted several follow-up phone interviews with government officials and healthcare professionals.
The research focused on the Lusaka and Copperbelt provinces, which have the largest number of adults and children living with HIV/AIDS and the most HIV treatment sites in Zambia. Apart from Kafue and Chongwe rural areas, our interviews took place mainly in the urban districts of Lusaka, Kitwe, and Ndola. Zambia is highly urbanized; the urban population has twice the infection rate of the rural population, and the most established treatment programs are in urban areas. Future research on HIV treatment barriers for rural women would be valuable.
A limitation to this research is that we mainly interviewed women connected to women's organizations and HIV support groups, or who attended adherence counseling. The experiences of women who are unable to access these services are likely to be more severe. Moreover, in terms of adherence, support group leaders and adherence counselors often emphasize that patients should take ART on time as prescribed by clinic staff. Women who have missed appointments to renew their prescriptions for ART reported that they were "told off" by clinic staff. Consequently, some of the women interviewed might have decided not to admit missing ART doses as they associated Human Rights Watch researchers with support group leaders or adherence counselors.
Another limitation is that we did not interview perpetrators, including husbands, intimate partners, and family members involved in property grabbing.
Unless stated otherwise, the names of women living with HIV/AIDS cited in this report have been disguised with names and initials (which do not reflect real names), in the interest of the privacy of the individuals concerned.
IV. Background
Gender and HIV/AIDS in Africa
More than twenty-five years after the first HIV cases were detected, Africa remains in the grip of a terrible epidemic.Millions of children have been orphaned and are at risk of abuse and exploitation, thousands of adults in their most productive years are dying every day, millions of others are sick, and countless others fear abandonment and even violence if they disclose their HIV status to family and friends.
Globally, 33.2 million people are living with HIV/AIDS.Of these approximately 15.4 million are women.[1]Sub-Saharan Africa remains the epicenter of the pandemic, with 22.5 million of all those with HIV living in this region, representing 68 percent of all infections.[2]
In Africa women with HIV outnumber men, constituting between 59 and 61 percent of all adults with HIV above age 15.[3]There is now a well established body of international and regional research that illustrates how gender inequalities fuel the epidemic and hamper efforts to prevent new infections among women.[4]Women's subordinate status within intimate relationships and their economic dependence on male partners make it difficult for them to negotiate safer sex and to use condoms consistently, for fear of being abandoned or assaulted.Concurrent relationships (or suspicion of concurrent relationships) in the age of HIV/AIDS often give rise to tensions that can result in domestic violence.[5]
The World Health Organization (WHO) has identified violence, including violence against women, as "a major public health problem in Africa."[6] Gender-based violence creates conditions conducive to the transmission of HIV to women, since women in violent relationships often experience coercive, violent sex and are unable to negotiate HIV prevention. Furthermore, some women may be unable to leave violent relationships because of their economic and psychological dependence on their abusers.Women's unequal property rights also contribute to the HIV/AIDS epidemic in the region.Under the laws and customs of many sub-Saharan African countries, women neither inherit nor keep property upon divorce on an equal basis with men.This reinforces their dependence on men, sometimes locking them in abusive relationships.This may also render women and their children destitute upon divorce or the death of their husbands.
Access and Adherence to Treatment
In 2003 2.1 million adults and children died of AIDS-related causes worldwide, the vast majority unable to pay for life-saving medication. At that time only 400,000 people in low- and middle-income countries were receiving antiretroviral therapy.[7]By December 2006 the reach of treatment had increased five-fold, to over two million, but even this figure represents only 28 percent of those who needed treatment.[8]Many adults and children still cannot access life-saving ART.Leaders of the Group of Eight (G8) and the United Nations General Assembly made commitments in 2005 and 2006 to work with the WHO, Joint United Nations Program on AIDS (UNAIDS), and other international institutions to move as close as possible to universal access to treatment by the year 2010.[9]This political commitment led to increased resources for HIV treatment programs, and in sub-Saharan Africa the scale-up of treatment has been dramatic.[10]
Despite these advances, governments and international health agencies point to several constraints in the delivery of and adherence to ART.These include the procurement and supply of drugs and equipment for diagnostic testing, limited human resources, limited capacity of healthcare systems, and lack of proper program management and monitoring systems.[11]These and other factors, such as food insecurity, poverty, lack of money for transport, stigma and discrimination, and direct and indirect user fees, are all factors that hold back the expansion of treatment programs. As Chapter V below shows, gender-based abuses substantially curtail women's ability to benefit fully from ART.In some cases women's enrollment in ART programs exposed them to domestic violence, and to abandonment and divorce, which coupled with insecure property rights, often exposed women to further impoverishment and even homelessness.If ART programs are not strengthened so that they take into account and help to address the impact of gender-based violence, lack of protection for women in family and property rights issues, and unequal relations between men and women in general, women will continue to miss out on life-saving treatment.
A high level of adherence is critical for the success of ART.According to the WHO, "adherence to ART is well recognized as an essential component of individual and programmatic treatment success."[12]Research on drug adherence has shown that "higher levels of drug adherence are associated with improved virological, immunological and clinical outcomes and that adherence rates exceeding 95 percent are necessary in order to maximize the benefits of ART."[13]Lack of adherence can lead to the development of drug resistance, which can lead to treatment failure among individuals and drug resistant strains of HIV can be transmitted to others during unprotected sex and other high-risk activity.[14]
Obstacles to Accessing HIV/AIDS Treatment in Zambia
In 2006 the prevalence of HIV in Zambia was about 17 percent (approximately 1.1 million people) among the 15 to 49 age group.[15] Women account for 57 percent of Zambians infected with HIV.[16]Girls and young women between ages 15 and 24 are four times more likely to be infected with HIV than their male counterparts.[17]
Despite increased knowledge of the importance of HIV counseling and testing, few Zambian women and men know their HIV status.[18]According to the most recent Zambia Sexual Behavior Survey (2005), although 80 percent of Zambian women and 83 percent of Zambian men stated that they knew a place where they could have an HIV test,[19] the percentage of Zambians who had ever been tested remained low.In 2005 the percentage of Zambian women and men who had ever been tested was 15.3 percent and 11.4 percent respectively.[20]Fear of learning the result, fear of stigma and discrimination, and lack of adequate health facilities are all factors contributing to the low percentage of people aware of their HIV status in Zambia.[21]Gender-based abuses and the fear of such abuses also determine women's decisions to access HIV testing.
In 2004 the Zambian government introduced free access to ART in the public health sector for those who need it, and in June 2005 the government declared that the whole ART service package would be available free of charge in the public health sector.[22]It appears, however, that this policy is not being uniformly applied in the two provinces studied for this report.Interviewees in Ndola, in the Copperbelt province, indicated that they only receive antiretroviral medicine free of charge, and must pay for CD4 countsand other diagnostic tests.[23]As the testimonies in Chapter V indicate, the cost of these tests is prohibitive for women with insecure property rights and also severely impacts women in abusive relationships.
In January 2004 only 1,483 people were accessing HIV treatment in Zambia. By November 2005 an estimated 43,964 people living with HIV were accessing antiretroviral drugs through 53 public health facilities throughout the country.[24] At the end of 2006 the number had increased to 75,000 and the number of sites to 110.[25]According to PEPFAR, by September 2007 the number of people receiving HIV treatment in Zambia had increased to 122,700.[26]
In 2006 61 percent of those accessing treatment were women.[27]Women are more likely to know their HIV status through antenatal healthcare services, Prevention of Mother to Child Transmission of HIV (PMTCT) programs, and through seeking pediatric medical assistance when a child is ill.However, the slightly higher percentage of women accessing HIV treatment raises the risk of complacency where healthcare providers and other stakeholders may overlook the serious hindrances to women's access and adherence to HIV treatment such as those discussed in this report.
The US President's Emergency Plan for AIDS Relief (PEPFAR) and the Global Fund to Fight AIDS, Tuberculosis and Malaria (the Global Fund) are the largest funders of HIV treatment in the country.Zambia is one of PEPFAR's 15 focus countries, and received support from the Global Fund in rounds one and four (see Chapter VIII).
HIV has placed enormous pressure on a public health system that was already struggling to serve Zambians while only committing approximately US$51 per capita per year for health services.[28]The Zambian government has identified a number of barriers to improving the healthcare system.These include a "human resource crisis," the poor state of health facilities, inadequate drugs and medical supplies, long distances to and between health facilities, poor transportation infrastructure, and high-levels of poverty.[29]Similarly, PEPFAR has identified several limitations within the health system that are hindering ART scale-up, such as inadequate staff and gaps in supply of drugs in the public sector.[30]Other barriers, such as stigma and food insecurity, compound the effects of these obstacles in the health system.
Staff shortages hinder the government's efforts to expand access to ART and ensure that access is equitable via addressing the specific needs of women who experience gender-based abuses.A 2006 Ministry of Health evaluation of the ART program in Zambia identified severe shortage and high turnover of trained staff as "the most significant constraint in ART service delivery."[31]The report identified "inadequate recruitment, insufficient re-training of the few staff in position, inadequate monetary and non-monetary retention incentives, long working hours in ART sites, and increased workload due to rapid increase in numbers of enrollments due to the free ARV policy"[32] as major causes of staff shortages.The latest available data on the number of healthcare workers in Zambia indicates that in 2004 there were only 1,264 physicians-0.12 physicians per 1,000 people-and 16,990 nurses-that is 1.56 nurses per 1,000 people.[33]
Dr. James Banda, director of the District Health Management Team for Kitwe, a large town in the Copperbelt, stated that staff shortage was "the most fundamental challenge that we face every day."[34]According to Banda, Kitwe's population of 460,000 is serviced by just 483 health care workers.[35]Staff shortages in Zambia are discussed further in Chapter VI.
Women in Zambia
Zambian women face multiple forms of discrimination and abuses, including gender-based violence and insecure property rights.Women's relatively low socioeconomic and political status is reflected in a number of indicators that are discussed below.
Domestic and Sexual Violence
In 2001-2002 more than half of ever-married women surveyed reported being beaten or abused by their husbands.[36]In November 2006 the Zambia chapter of Young Women's Christian Association (YWCA) reported that their shelter recorded ten cases of rape of adult women in Lusaka every week.[37]There is no specific law against domestic violence, so cases must be prosecuted under the general assault statutes, which typically do not provide effective protection for women because of the need to provide evidence of gross bodily harm, or of the fact that the perpetrator was carrying a weapon.Moreover, the penal code does not specifically prohibit marital rape, and the provisions on rape in the code do not in practice apply to spousal rape.
Property Rights
Zambian statutory law partially protects women's inheritance and property rights, but failure to prevent discriminatory customary law taking precedence over statutory law undermines such protection.Moreover, the laws are poorly enforced.The Intestate Succession Act (1996 amendment) provides that a widow should receive 20 percent of her deceased husband's estate, and that it is illegal to evict a surviving spouse from a matrimonial home.[38]However, under the customs of some ethnic groups, which are more widely used by Zambians than statutory law, the right to inherit property often rests with the deceased man's family.The inability to enforce their property rights in the area of inheritance is compounded for HIV-positive widows since in-laws sometimes threaten to punish them if they insist on keeping their property by not caring for their childrenwere they to fall sick or die.A lawyer at the International Justice Initiative, an organization that focuses on cases of property grabbing, told Human Rights Watch, "We had one case when a woman was [HIV] positive, [her in-laws] said, 'It is just a matter of time, you are sick [and will die soon] and then see what we are going to do to the children.'"[39]
In-laws may also insist that a widow undergoes sexual "cleansing" (through sexual intercourse with a hired male of lower social status), and as a result, widows sometimes give up their property to avoid this practice.As Yoram Siame, HIV/AIDS program officer at the Church Health Association of Zambia, a PEPFAR partner, put it, "If a widow is not willing to share property with in-laws, they will say, 'Take everything, but we want cleansing.'"[40]
The Matrimonial Causes Act, which address division of marital property upon divorce, was passed by the National Assembly passed in 2007 and is awaiting presidential signature.[41]When it comes into force, the Matrimonial Causes Act will be applicable to civil marriagesunder the Marriage Act.[42]It enables courts to determine settlement of property upon divorce, but is silent in terms of equal distribution of property upon divorce.However, most people in Zambia marry according to customary law rather than the civil marriage statute, and thus the protections of the Matrimonial Causes Act will not apply to them.[43]Although customary law is continuously evolving and heterogeneous, reflecting the norms of Zambia's 73 ethnic groups, it generally continues to discriminate against women in marriage and divorce.Customary practices tend to grant men all rights to marital property.
Zambia's constitution prohibits the enactment of any law that is discriminatory on the basis of sex or has such discriminatory effect.But it also recognizes a "dual legal system," which allows local courts to administer customary laws, some of which discriminate against women.
One promising property rights development is Zambia's land policy, which requires that 30 percent of all land advertised for lease be allocated to women.However, to qualify for the land acquisition it is necessary to prove the capacity to develop the land, as evidenced by bank statements, and this is often an impossible hurdle for women.[44]
Social, Economic, and Political Indicators of the Status of Women
A range of indicators show that women are at a distinct social and economic disadvantage in Zambia.Statistics on literacy show that only 59.7 percent of women are literate compared to 76.1 percent of men.[45]Poverty affects women disproportionately.Many women are in low-paid and low-skilled jobs with little job security.Seventy-six percent of women in Zambia are engaged in agriculture, fisheries, and forestry.[46]Sixty-three percent of women engaged in agricultural work receive no payment for their work, compared to 56 percent of males working in the same sector who do not get paid for their work.[47]
Women's Political Participation
In Zambia women's representation in government falls below the 30 percent target set by the Southern African Development Community and the 50 percent target set by the African Union.[48]In 2006 only 100 women stood for election to the National Assembly, compared to 605 men.Of these 100 female candidates, only 21 were elected to the National Assembly, representing 14.19 percent of the Assembly.[49]There are currently only 22 women MPs out of a total of 150 elected and nominated members of the National Assembly.Only six out of 23 cabinet members are women, although after the 2006 elections the President of Zambia appointed a Minister of Gender and Development.[50]
Decision-Making within the Household and Negotiation of Safer Sex
In Zambia women's ability to make informed decisions about their health and lives, including their ability to obtain information on HIV/AIDS, counseling, and testing, and their ability to negotiate safer sex, is seriously impaired by the perceived and real control of men (particularly intimate partners) over their lives.At the household level, statistics from the Zambia Demographic Health Survey (ZDHS) indicate that the majority of husbands have the final say in making decisions on wives' healthcare.[51]As the interviews for this report indicate, this meant that women felt unable to receive HIV testing or treatment without their husbands' permission.The ZDHS also indicates a strong correlation between a woman's financial position and her decision-making power: of wives who indicated that they had no say in household decision-making, 36 percent were unemployed, 30 percent were employed but not for cash, and only 18 percent were in formal, paid employment.[52]
Women in some of Zambia's ethnic communities are socialized to be submissive, not to challenge male authority, and to respect and please men.[53]As one activist told Human Rights Watch, "Women can't speak in public. They shouldn't discuss their domestic affairs. They must keep quiet as a wife."[54]Over half of the women interviewed for this research indicated that married women in many Zambian communities are taught to submit to demands for sex from their husbands and have little power to negotiate safer sex.They said it was considered inappropriate for women to initiate discussions about sex with their intimate partners.
Many of the women interviewed for this report described the difficulties they experienced in attempting to negotiate condom use.Isabel H. told Human Rights Watch that healthcare workers told her that she must refrain from having unprotected sex with her husband as both were living with HIV.Isabel H.'s husband refused to use condoms: "Every time we had sex, there was a quarrel.He didn't want to use condoms."[55]
Cultural beliefs about the roles of women and men also inform how women themselves think about, and respond to, gender-based violence.The ZDHS found that a large majority of women (85 percent) and men (69 percent) believed that a husband is justified in beating his wife for at least one reason.[56]As one activist put it, "our culture means that women must accept certain extremes, for example, violence. They are constrained by culture when [a woman] gets married, she is told, 'take things as they come.' She must accept a certain level of abuse, it's a way of life."[57]
V. The Impact of Gender-Based Abuses on Women's HIV Treatment
We have seen domestic violence interfere with ARVs [antiretroviral drugs] many times.There are several examples of such cases among women in [YWCA's] shelter.One [of the women in the shelter] had a partner who threw away her pills.[He] said to her, "If you have to drink medicine you're out of this house."
-Yeta Mekazu, shelter manager, Young Women's Christian Association, Lusaka, February 1, 2007
Human Rights Watch identified gender-specific barriers that impede Zambian women's ability to seek HIV information or start and continue using ART.These include violence and the fear of violence by intimate partners, the fear of abandonment and divorce in an environment where women suffer insecure property rights, and property grabbing upon the death of a spouse.These abuses occur in the context of poverty and of a culture that condones male authority and control over women.The final result can be severe.Some of the women in need of ART either do not access ART in the first place, with dreadful impact on their health and their lives, or they hide their HIV status and their ART, which sometimes results in missing vital ART doses or appointments to collect their medication.
Gender-Based Violence
Women reported to Human Rights Watch that domestic violence at the hands of their husbands and intimate partners, and the fear of such violence, had a direct, harmful impact on their ability to start and continue using ART.Women said that they were beaten, slapped, shouted at, verbally abused, and raped upon discussing HIV testing and treatment with their husbands, after disclosing their HIV status to their husbands, and as a result of visiting health facilities to collect their ART.
Some of the women interviewed for this report said that they could not be tested for HIV infection or get access to ART because of the kinds of abuses described in this chapter, or fear of such abuses.Some women only accessed HIV services and started ART after their husbands died.Others said that they received HIV tests through antenatal services while pregnant, but because of violence and the fear of violence they did not go back to the health facility to collect their test results.Other women started taking ART without informing their husbands.
HIV Testing and Disclosure
To access treatment women need to receive an HIV test, and if the test results are positive, they usually take further tests before they can start ART.Married women interviewed for this report stated that their husbands and other intimate partners beat, kicked, or emotionally abused them when discussing HIV testing and treatment, and when they disclosed their positive HIV status.This caused critical delay in their ability to start ART.Mercy Z., 29, told Human Rights Watch,
I got married in 2004 and my husband started giving me STDs [sexually transmitted diseases]. He goes out with women.When I ask for a condom, or go to the clinic to get treatment, he starts beating me. In January 2006 I went for VCT [voluntary counseling and testing].He was refusing [to receive an HIV test].The results came positive. From the time I got the results, he started beating me up.After two months he chased me away. He beat me everywhere.When I was four months pregnant he beat me until the placenta came out.I had to go to the Victim Support Unit [a special unit of the Zambian police that addresses abuses against women and children].[58]
Some of the women interviewed for this report described the psychological abuse they experienced as a result of discussing HIV testing with their husbands and when their husbands found out about their HIV status.Unique Z., who lived with her Zambian husband in a neighboring country where he worked, told Human Rights Watch that when she discussed HIV testing and counseling, "[My husband] just ignores me, he does not even eat in the house.He just comes home and takes a bath and goes out again."[59]Unique Z. said that this delayed her decision to receive an HIV test until she became very sick:
When I became very sick, I said that I needed to be near my mother and came back to Zambia. [That was when] my brother took me to take an HIV test.[At the time], my CD4 countwas 21.[60]When I tested positive, I went into depression for three weeks I am on ARVs [antiretroviral therapy] and on Monday my CD4 count was 725.When I [first] met [my former husband] he was very good.Two months after we met he said to me "I want you as a parent [mother for his children]." I said to him okay, let us have [an HIV] test.I [later] discovered that he was just a womanizer.We fought when I asked him about women.He hit me on the mouth.He tore half of my hair.I spoke to his brother but he told me that this was a domestic affair and there is no need to involve the police.I just went to his elders and discussed it."He is not a criminal." That is what they said.[61]
Numerous other women said that their husbands described them as "prostitutes," suggesting that the women had extramarital affairs and as a result they suspected that they had sexually transmitted infections.As such, several women interviewed for this report told Human Rights Watch that they decided not to discuss the matter with their husbands or take HIV tests.
Women who access routine HIV testing as part of antenatal services sometimes fear domestic violence should they raise the issue with their partner or husband and as a result some may never return to the clinic to receive their HIV diagnosis or to be assessed for readiness for ART. Others simply decide not to start ART.Monica Mwachande, a senior nurse at the government's Kalingalinga Clinic, said that when she asks women why they did not return to the clinic for further tests, "At times they say, 'Suppose I find my results positive, this may cause problems at home.'"[62]
The impact of the delay in HIV testing and in commencing ART as a result of violence is reflected in the testimony of Precious C., 43, who was only able to receive an HIV test and later enroll on ART after her husband abandoned and then divorced her.She told Human Rights Watch, "My CD4 count was only 4 . I went down to 27 kilograms from 68 kilograms.[I looked like] a skeleton.There were buds [bumps/blisters associated with AIDS related skin conditions] coming from my body and I was impaired whenever I came into contact with sunlight I realized that I was killing myself."[63]Precious said that had she still been with her husband, she never would have been able to start ART, and that she could have died as a result:"If I was still with him I am sure I would have died [by now] because he'd never have allowed me to test or go on medicationHe used to beat me a lot."[64]
Another factor that delays women's access to HIV testing and ART is that women sometimes feel that they must obtain their husbands' or partners' permission to receive an HIV test.Many of the women interviewed for this report said they were counseled upon reaching puberty to be submissive and obey their future husbands.Women also repeatedly told Human Rights Watch that they received pre-marital counseling from elderly female relatives who emphasized women's subordinate role within the household and their obligation to obey their husbands.Violence against women within the household, they were told, was normal and acceptable, and a woman should remain in her marriage regardless of her husband's behavior.In some traditions, according to Women in Law and Development in Africa (WiLDAF), "domestic violence is misconstrued as a sign of love, 'rather than divorce her, he is willing to mould her into the kind of woman that he wants.'"[65]Like gender-based violence, these gender norms and socialization often shape women's attitudes toward seeking healthcare, including HIV testing and counseling, with devastating results.
A number of women said that until their husbands died, they felt unable to take an HIV test or access treatment.When Ruth M., a 52-year-old farmer from Chongwe, and her husband started getting sick, she tried in vain to convince her husband to allow her to receive an HIV test, and for him to test as well:
I used to tell my husband, we should both [receive] HIV test[s].He refused.He didn't want me to go for a test.He said, "This is not AIDS but people just [be]witched us."We used to go to witch doctors, but there was no help.We just wasted a lot of money I went for [an HIV] test and the results were positive.I am on ARVs now If it was not for my husband, I would have gone for VCT long ago.I didn't know what was wrong [with me] and sold a lot of things at the farm to pay the [witch] doctors.Now there is hunger at home and a lot of poverty.[66]
A growing body of research addressing women in sub-Saharan Africa shows that despite incidents of gender-based violence and abandonment upon disclosure,[67] where there is acceptance of a woman's HIV-positive serostatus by her partner, being able to disclose HIV test results to sexual partners resulted in less anxiety, increased social support, and improved access to care and support programs.[68]Still, the difficulties that women in sub-Saharan Africa face in disclosing their HIV-positive status are reflected in the fact that the lowest rates of disclosure in the studies conducted among women receiving antenatal services were in sub-Saharan Africa.[69] Many of the women interviewed for this research said they felt unable to disclose their HIV status to their husbands, and as a result had to take HIV medicine secretly (see below).
The Impact of Violence and Abuse on Access and Use of ART
Women interviewed for this report who were enrolled in ART programs told Human Rights Watch that, as a result of physical and psychological abuse and the fear of such abuse, they sometimes missed ART doses and clinic appointments, including appointments to collect their medicine.Some women felt compelled to hide their HIV status and medicine because of fear of violence, or because they feared that their husbands might dispose of the medicine.Berta K., whose husband beat her routinely, told Human Rights Watch, "I started medication in 2006. [My husband] does not know."[70]Beatrice S. told Human Rights Watch that she was not planning to inform her husband about her HIV status: "My husband is not good to me.Once I asked him to go for VCT but he refused.He does not want me to drink any medicine or go anywhere.Even these scratches on my face are because I was in the market to buy vegetables.He said, 'You are late, why?' and he started beating me.He beats me up about every two weeks."[71]
Commencing ART without informing their husbands, many women told Human Rights Watch that they had to grapple even with where to keep their medication. Some of the women testified that they dug holes in the ground or in flower pots to hide ARVs.These women then retrieved the medicine-which they must take for the rest of their lives-twice every day and then hid it again.Others told Human Rights Watch that they hid the medication in the dish or bag for the family's mealie meal (maize-based traditional staple). Others said they hid the medicine in suitcases under their beds, or in aspirin and panadol containers.Some pretended they were taking family planning pills.Some of the women said they missed ART doses as a result of all this subterfuge.One woman told Human Rights Watch that because she fears domestic violence, "I take the medicine out of the bottle and put it in a plastic [bag] or in a paracetamolbox [container] . Sometimes I would miss a dose."[72] Marrietta M., who said that her husband often beat and insulted her, hides ART in her clothes: "I hide my treatment in my clothes.My husband will not look for it in my clothes.My husband and I fight a lot. He insults me and he says very bad things to me. He is a very difficult person and I do not want to upset him."[73]
Having started ART secretly, some of the women interviewed by Human Rights Watch said that when they experienced side effects of treatment, they had to make up explanations so as to avoid violence and other abuses.Marietta M. told Human Rights Watch, "When I started the medication, I had bad side effects.I had to tell my husband that it was malaria."[74]
Regardless of whether husbands knew about their HIV status or treatment, women whose husbands continually beat them or otherwise abused them sometimes missed ART doses.Berta K., stated,
[Sometimes, my husband] comes back at 18:00 hrs, drunk, closes the door and says, "Today you are going to freak out."He locks [me] in, he beats me up and then he locks me out.[On another day I would say], "Here is Nshima" (traditional Zambian food), and he would say, "You think I am not wise enough to know this is Nshima?"He beats me up and locks me out of the house.I go to the neighbors.If they have mercy they will let [me] in, if not, [I] sleep under a tree until tomorrow.As a result of that I miss doses sometimes.I feel very bad. I don't even feel like taking the medicine.I say, "Ha, let me die."[75]
Other women told Human Rights Watch that their husbands beat them or threatened to beat them if they saw them taking ART.Charity T. said, "I do not take my medicine in front of my husband.He told me that he would beat me if he saw me taking the pills.He did slap me when he saw me take them.I did miss taking some of the pills because I was scared of my husband.It was very difficult for me to take the medication in the beginning because of him."[76]
Most of the women interviewed for this report testified to the impact of verbal abuse on their health in general and on their adherence to ART.Rooted in dominant beliefs about women, verbal abuse described by women interviewed also reveals how stigma is entrenched in society.Verbal abuse often takes place alongside other forms of abuse. Efforts to avoid such abuse have caused over 30 of the women we interviewed to miss ART doses.The testimony of Maria T., 45, whose husband only knows that she has tuberculosis, is telling:
I did not tell anybody about my [HIV] status apart from [members of] the support group.I fear to tell my husband because I fear that he can shout [at me] and divorce me.He uses bad language with me every time, especially when he is drunk.[He says], "The vagina of your mother," "the anus of your mother, move away from me you are a patient of TB, you could die in my hands." I hide the medicine, I put it on a plate, add mealie meal, so when he takes the lid off he [does not find the ART medicine].I take the medicine at 8:00 hrs [when he is] at home and at 20:00 hrs when he is still at work.I have to make sure that he is outside.That is why I forgot to take medicine four times since I started treatment [in June 2006].Last year he hit me around the back with his fist. I got the cooking stick and hit him back.[77]
In addition to the direct, dire impact of physical and verbal abuse on women's ability to access and continue using ART, at least five women told Human Rights Watch that their husbands threw away their antiretroviral medicine.Charity T., whose husband abused her physically, stated,
Once [my husband] threw away my medication into the pit latrine. He said that he did not want to see these medicines in his house.I used to hide the medicines with my neighbor; I left them there for six months.After he threw the medicines away, I had to go back to the clinic the next day to get more medicine.I did explain to the nurse what had happened.She got me more medicines.[78]
Several support group leaders, activists in women's groups, and HIV treatment- adherence counselors told Human Rights Watch similar stories.Ida Mukuka, an AIDS activist and former support groups coordinator, said that in some of the groups she ran "Women would come and say, 'My husband rapes me every night. He would throw the ARVs in the toilet.'It is a very sad situation."[79]An adherence counselor in Lusaka also relayed the experience of a former patient who passed away: "She took her drugs at the same time as her husband.Every time they quarreled her husband would beat her up and take her drugs and throw them away."[80]The manager of the shelter that the Young Women's Christian Association (YWCA) established in Lusaka also recounted the stories of two women survivors of domestic violence who used the services of the YWCA shelter, "The partners of two women who are on ARVs refused [to let] the women drink [HIV] medicine.One woman [said that] her husband threw away her medicine and told her, 'If you drink that medicine, you are out of this house.'"[81]
The experiences of women interviewed for this research show that gender-based violence thwarts the ability of many of them to continue HIV treatment.The majority of the women interviewed told Human Rights Watch that they attended adherence counseling sessions at ART clinics.When asked whether they discussed their experiences of verbal, psychological, and physical abuse, they said that counselors did not usually ask about these issues, unless they notice visible marks of assault (see Chapter VI).[82]
Some of the women interviewed by Human Rights Watch stated that despite continuous beating and verbal abuse, they made sure to take their ART on time.This could be because the majority of the informants started treatment when they were already extremely ill with full-blown AIDS and so have seen the difference ART made in improving their health over time. Or another reason, as noted in Chapter III, could be that Human Rights Watch researchers mainly interviewed women who were connected to support groups, attended adherence counseling, or both.Support group leaders and adherence counselors often emphasize that patients should take ART on time as prescribed by clinic staff.Women who have missed appointments to renew their prescriptions for ART reported that they were "told off" by clinic staff.Consequently, some of the women interviewed might have decided not to admit missing ART doses as they associated Human Rights Watch researchers with clinic staff.
The testimonies in this chapter show that women are very resilient and often use creative means to ensure that they take ART on time and attend clinic appointments, while at the same time undertaking key care responsibilities. Some even use gender-based violence as an excuse to attend clinic appointments.The story of Lucia G. is indicative:
I tested [for HIV] in 2005.I was ill [and] a nurse asked me to go for VCT.I asked my husband who refused and said "if you go for VCT and test positive I will divorce you."I went secretly [to the clinic] and tested positive.This way I knew what was wrong with me.After three months my CD4 [count] went down so I was put on ARVs.I am still on ARVs but my husband does not know.I am only managing because I hide medicine.I dig in the ground, put medicine in a tin, and put it in a hole then put the water bucket over it, so no one would know that there is medicine buried underneath.I am always thinking about my life.I do not want to lose my marriage and I do not want to lose my life, so I have to do this to keep my marriage and my life.If I am divorced I cannot look after the children.My husband is very arrogant.This scar on my face is because he hit me.He beats me because he suspects I am ill and because I go to the clinic a lot when I am ill or [to collect] ARVs.He beats me, insults me, and asks me why I go to the clinic every time.I tell him I need to go to the clinic because of the beating.If I do not get beaten for a whole week that is too long.He hits me almost everyday, which is good for me because I can [find an excuse to] go to the clinic.I never reported him [to the police].I once told the headman [village chief].[83]
Lucia G., and other women interviewed for this research described how they raise funds specifically to cover transportation costs to attend clinic appointments."When my appointment [at the HIV clinic] gets nearer, I sell pumpkin leaves to raise money [for transportation].Sometimes I manage [and] sometimes I don't, so I borrow money from friends."[84]Similarly, Angela R., a market vendor who sells fruits, who said she hid ARVs between two flower pots, told Human Rights Watch: "I go [to the clinic] by bus and have to pay [Kw10,000 (about US$2.50) for a round trip].I do not [usually] get profit from my business, so when there are a few days left for my appointment at the clinic, I do some piece work, like washing other people's clothes.Once I missed a clinic appointment last December because I had no transport money.At the clinic they shouted at me and warned me not to miss [appointments or ART doses] because this is very dangerous."[85]
Insecure Property Rights
Women interviewed for this report identified unequal property rights, and their inability to protect their property rights, as a major factor impeding their access to ART and their ability to adhere to treatment.For women who married under discriminatory customary laws, their lack of property rights often mean having to remain in abusive marriages, which in turn can impede treatment.Fear of divorce in a context where women are economically dependent on men forces some women to hide ART. Women who seek divorce and lose property they accumulated during their marriage suffer constraints that restrict their ability to afford transportation costs to attend clinic appointments, collect ARVs, or attend treatment-adherence counseling.Similarly, widows told Human Rights Watch about property grabbing by in-laws when their husbands died, which made it harder for them to start and continue taking ART, due to economic constraints.Property grabbing also led some women to enter new, abusive marriages just to sustain themselves and their children.
Unequal Property Rights upon Divorce
Right now, [we have about] seventy clients for [each] legal officer.The most common issue is divorce in local courts.If married under customary law, nothing is given to the woman.[Not] even her clothes!
-Rumbidzai Mutasa, legal officer at the Women's Legal Aid Clinic, Lusaka, February 23, 2007
As noted above, among some ethnic groups in Zambia, to which over 50 percent of the women interviewed for this report belong, women who marry under customary law often lose the property accumulated during their marriages upon divorce.[86]The resulting economic hardship often affects their HIV treatment.Women who divorced under customary law told Human Rights Watch that they suffered abject poverty and were not able to afford transportation to health facilities to collect ARVs or even to afford food.As a result, they had to take medicine on an empty stomach.This is problematic as some ARVs must be taken with food and good diet can help with recovery.Moreover, the appetite of people recovering from AIDS related illnesses may increase.[87]
Human Rights Watch documented the experiences of women abandoned by their husbands and other intimate partners, chased from their homes, and divorced by their husbands as a direct result of disclosing their HIV status.Women told Human Rights Watch that fear of abandonment and divorce, and the consequent loss of property, sometimes forced them to hide their HIV status and their ARVs.Caroline M., 31, whose first husband divorced her upon finding out that she had HIV, eventually married another man to whom she did not disclose her HIV status, so she hid ARVs."If I disclose my status to my husband," said Caroline M.
I fear two things: [being] divorced again or that my husband would just say, "Stop taking ARVs, you are okay".So when I get the ARVs from the clinic, I throw away the box [container] and keep the plastic [bag].I place the medicine underneath clothes in the wardrobe.My husband does not even touch clothes.He asks me to bring clothes to him from the wardrobe. I take the medicine at 8:00 hrs and 20:00 hrs.We only have two rooms so when my husband brings friends home I prepare themedicine and put it in the kitchen in advance.My new husband is bossy.He always says "You can't be positive, and these ARVs you hear about are not good."He thinks he cannot be HIV-positive.When he's drunk he is a problem.He hits me and shouts at me.[88]
Ann K., 27, whose husband divorced her, received her HIV-positive test result one day prior to her interview with Human Rights Watch.Married according to customary law, she told Human Rights Watch that upon divorcing her, her husband appropriated all her belongings, including plates, cupboards, mattresses and sheets.Ann K. said she complained to the "headman" of the farm where she lived with her husband, but her husband ran away to Lusaka to avoid confrontation with the headman, and her former husband's new wife claimed that these items were presents from her parents.Ann K. said that she gave up trying to reclaim her badly needed belongings due to ill-health."I am sick but I have no sheets or mattresses.I have to sleep on a mat on the floor.I have one blanket that my niece gave to me.I share it with the children."[89]She was due to return to the HIV clinic on the next day for further tests.Ann K. said that although the doctors might enroll her on ART, she might not be able to tolerate the medication with no food to eat.
Property Grabbing
Widows living with HIV/AIDS interviewed by Human Rights Watch described the daunting impact of property grabbing-the unlawful appropriation of property by relatives of the deceased (usually a man)-on their HIV treatment.Property grabbed by in-laws, said these widows, could have helped them start small businesses, feed themselves and their children, and pay for transport to attend clinic appointments.Some of the widows who needed HIV treatment before it was available for free also said that property grabbed by in-laws could have helped them generate income to cover ART costs.
When Mina P.'s husband died in 1999, she had already told him that she was living with HIV/AIDS.Along with his relatives, he accused her of "bringing HIV to the house."Upon her husband's death, his relatives took the couple's property:
I was not working when my husband died.His relatives blamed me They said that I had brought illness into his house.His relatives took all the property and they sold our land.I didn't get any money from the land.I did not [report this to the Victim Support Unit].My relatives said that I must not fight over the land ...You do not fight over land as we all come from the soil.When I had the land, [my family] always had something to eat.After they took the land, I really struggled and we often did not have food.This was not good for my health and I got sick. I could not afford [HIV] treatment at this time. If I had had the land, I could have sold it to pay for [HIV] treatment or I could have sold some of the things that we grew.[90]
Even after the Zambian government made ARVs available for free, property grabbing by in-laws has at times forced widows receiving ART to miss vital clinic appointments because they were unable to afford transportation costs.The experience of Hilda M. is illustrative:
All the property was taken by [my late husband's] relatives. They took a motor vehicle, TV, radio, DVD player, dining room suite and sitting room chairs.They told me that I was going to die so I would not need these things. I did not try to get this property back-it is the way things are-I have no power.My problem is that I do not have enough food now.These drugs are very strong.I need to have food to take them.If I had the minibus I would use it for business and I would get money for food and transport. I have to catch a bus to the hospital to get my medication every month.My sister has to give me money for this, and when she can't, I have to walk. It is too far when I am feeling weak.I have missed some appointments when I do not have money for transport.Once I did not collect my medication for three days.[91]
Not only does property grabbing intensify poverty among women, it also prompts them to enter into new relationships for economic security, in some cases with abusive partners.When June S.'s husband passed away in 1991, his relatives "grabbed everything."[92]June S. never got her property back.Having received an HIV-positive diagnosis the same year, she went to live with her father and stepmother, where she was mistreated.After four years June S. remarried.She told Human Rights Watch that her current husband beats her up, rapes her, and refuses to use protection during sexual intercourse, even though she disclosed her HIV status to him.Whenever she refused to have unprotected sex with her husband, said June S., her husband would just grab her.[93]June S. reported her husband to the government's Victim Support Unit (VSU) when he beat her badly, and VSU officers offered to refer her to the YWCA shelter.June S. told Human Rights Watch that she wanted to know her CD4 count to see if she needed HIV treatment, but that her husband "does not want to hear about HIV treatment."[94]She explained to Human Rights Watch that had her property not been grabbed when her first husband died, she could have sold the property to keep going, and that she could have left her current abusive husband.
When the husband of Beatrice S., 35, died, his relatives grabbed all their belongings."The family got these things because [my] husband worked: TV, fridge, stove, sofa, and iron.I got nothing, just my clothes."[95] Beatrice, who has been receiving ART since 2004, had to find accommodation with a friend who later married her.Beatrice S. said that she will not inform her current (similarly abusive) husband about her HIV status or about the fact that she is on ART.
Lack of Access to Food
Many of the women interviewed for this report, especially those who lost their property upon divorce or upon the death of their partners, spoke of hunger as a major problem marking their experiences of taking ART.[96]Lack of adequate food is a general problem in Zambia, where, in 2004, 68 percent of the population was classified as poor, and 53 percent of the population could not afford the cost of a basic food basket of Kw78,223 (about US$18.50) per month.[97]Poverty in Zambia affects women disproportionately, given their already low economic status and dependency on male partners.For example, in 2002/2003 poverty stood at 58 percent in female-headed households, compared to male-headed households where poverty stood at 43 percent.[98]
For adults and children living with HIV/AIDS, adequate food and nutrition are essential for the health of their immune systems and for the success of ART.According to the Joint United Nations Programme on HIV/AIDS (UNAIDS), "Adequate nutrition is essential to maintain a person's immune system, to sustain healthy levels of physical activity, and for quality of life. Adequate nutrition is also necessary for optimal benefits from antiretroviral therapy."[99] Similarly, Pathfinder International explains that,
Many people who are diagnosed with AIDS have lost weight through chronic ill health. They may have decreased appetite, be unable to eat much because of candidiasis in the mouth or esophagus, have poor absorption, or have chronic diarrhea. Co-infection with TB is common in HIV infection, and widespread TB infection may also cause weight loss. Weight gain may be rapid for persons commencing ART and after treatment of TB. Some ARVs must be taken with food and recovery may be assisted by a good diet. Many people recovering from AIDS-related infections have increased appetite, and this can be a problem in poor households that are not food secure.[100]
Payment of Related Costs
Women who do not enjoy secure property rights may also lack the resources needed for tests related to ART where these are not consistently available for free, as is the case in the Copperbelt province.As discussed earlier, in June 2005 the Ministry of Health announced that it would provide a full package of HIV/AIDS care, including ART, free of charge to Zambians. It appears, however, that this policy is not being uniformly applied in the two provinces studied for this report.Interviewees in Ndola, in the Copperbelt province, indicated that they only receive antiretroviral medicine free of charge, and must pay for CD4 countsand other diagnostic tests.
For all the reasons explained above, the cost of these tests also severely impacts women in abusive relationships.For example, Dorothy M., who said that healthcare workers advised her to have a CD4 count every six months, said that she was four months late on taking the test because she could not afford the cost.Her husband-who assaulted and abandoned her along with her two children when he found out that she had HIV-refused to pay for it.[101]Another woman told Human Rights Watch that she was unable to commence treatment because she could not afford the cost of the CD4 count. Her doctor recommended that she take the test as soon as possible since she had suffered from a number of opportunistic infections, but her husband refused to pay.[102]
VI. Zambia's Response to Gender-Based Abuses Impeding Women's HIV Treatment
I have always felt that [the government is] not doing anything.If the president says, "declare free drugs," do they know what is happening to women?When ministers talk about achievements [in terms of treatment rollout], the biggest beneficiaries of ARV [programs] are women.[But] What have they [really] done for them?They need to put appropriate laws and policies in place.[There is a need] for provisions for women [so] if they are beaten because they are [HIV] positive, men should be jailed.
-Ida Mukuka, AIDS activist and former support groups' coordinator in Lusaka, January 31, 2007
The Zambian government's rollout of free ART is commendable as is the establishment of a gender ministry in 2006.However, the government has not done nearly enough to prevent or respond to gender-based violence and inadequate protection of women's property rights, and the impact that these abuses have on women's ability to access and adhere to ART.Healthcare facilities providing ART-which are overburdened and under-staffed-have no systems in place to detect or address gender-based abuses such as domestic violence.The training that counselors receive does not cover gender-based abuses in a systematic manner, nor does the understanding of gender-based abuses factor into official counselor certification.There are no government protocols on how to address gender-based abuses, including domestic violence, within ART programs, and monitoring systems do not track the effects of such abuse. Our research found no arrangement or partnership between the government and nongovernmental service providers that could provide such services at healthcare facilities.
Similarly, the country's legal framework fails to address these issues adequately.Zambia has no specific law that criminalizes gender-based violence.The penal code does not cover marital rape or psychological abuse.Prevalent customary laws discriminate against women in terms of property allocation upon divorce or the death of a spouse.The 1989 Intestate Succession Act regulates inheritance where the deceased did not leave a will, by providing for the surviving spouse in such cases, but it is ill-enforced.
This chapter examines the response-or lack thereof-of the health system and the legal, justice, and policy frameworks in Zambia to the violations described in the previous chapter.
The Health System
Health Policies
The Zambian government is responsible for devising health policies, delivering healthcare services, regulating private providers of healthcare services, and regulating healthcare workers, including HIV and ART adherence counselors.[103]In 2005 the Zambian government launched the National HIV/AIDS/STI/TB Policy (hereafter National HIV Policy).The policy identifies "[g]ender issues that perpetuate the dominance of male interests and lack of self assertiveness on the part of women in sexual relations" as a major factor contributing to the spread of HIV.The policy also lists women's poor socioeconomic status and unequal distribution of household resources as determinants of the disproportionate effects of AIDS on women.The policy, however, does not mention gender-based violence and its effects on treatment.
In May 2006 the government launched the National HIV and AIDS Strategic Framework, which stated that AIDS was inter-linked with poverty, social and economic inequality between women and men, and dominant cultural beliefs, and acknowledged the disproportionate effect of AIDS on women.[104]This framework, however, does not suggest ways to address gender-based abuses.The Fifth National Development Plan (2006-2010) (FNDP) further articulates the national policy response to HIV/AIDS.It has a specific chapter on gender and recognizes the role of gender-based violence in the spread of HIV/AIDS.[105]The FNDP recommends strengthening the penal code with respect to gender-based violence and facilitating the enactment of a gender-based violence bill as strategies for the gender sector during the period (2006-2010).[106]
Healthcare Facilities and Gender-Based Violence
In the past decade an international consensus has gathered around the importance of recognizing gender-based violence as a critical public health issue,[107] and as a barrier to women's use of health services.[108]As a result, the WHO and UNAIDS issued a policy statement in 2004, calling for interventions that take into account the different needs of women and men who access HIV services.[109]And the UN Commission on Human Rights in 2005 encouraged states "to ensure the availability towomen and girls of comprehensive and accessible health-care services and programmes and to health‑care providers who are knowledgeable and trained to recognize signs of violence against women and girls and to meet the needs of patients who have been subjected to violence, in order to minimize the adverse physical and psychological consequences of violence."[110]
In 1999 the Committee on the Elimination of Discrimination against Women (CEDAW Committee) identified gender-based violence as a critical health issue for women, and called upon states parties to guarantee "(a) The enactment and effective enforcement of laws and the formulation of policies, including health care protocols and hospital procedures to address violence against women and the provision of appropriate health services; (b) Gender-sensitive training to enable health care workers to detect and manage the health consequences of gender-based violence."[111]
In Zambia our investigation revealed that healthcare facilities providing ART have not adequately responded to gender-based abuses, including violence against women, in a way that would enhance women's access and adherence to ART.Although relevant policies generally highlight the importance of gender in addressing health needs in Zambia, they seldom address gender-based violence.Healthcare workers responsible for monitoring adherence to ART are not required to probe for gender-based violence or other abuses as potential hindrances to successful treatment, nor are they adequately trained to do so.Existing health protocols do not cover gender-based violence.
HIV adherence counselors, other health professionals, and policy-makers, however, told Human Rights Watch that they would welcome programs through which they could probe for and address gender-based violence in ART clinics, if adequately trained and equipped to do so.This should be part of an overall strategy to address gender-based violence and other abuses that affect Zambian women.
Monitoring Adherence to ART and Gender-Based Abuses
Chapter V discusses the extent to which violence against women and inadequate protection of property rights for women affect women's access and adherence to HIV treatment.Health facilities disseminating ART, including clinics, could play an important role in detecting and responding to these abuses, especially during adherence counseling sessions.In Zambia clinical follow up for all patients living with HIV/AIDS takes place at least every three months.Patients receiving ART typically present every month at clinics to collect their drugs.[112]At these monthly visits they also generally attend adherence counseling sessions.These are one-on-one sessions where a trained counselor determines the capacity of a patient to take his or her prescribed ART, monitors adherence to ART, and helps patients develop ways to cope with their illness and with ART.
Human Rights Watch's interviews with women receiving ART and with healthcare staff, including adherence counselors, indicated that healthcare facilities providing and monitoring adherence to ART seldom address gender-based violence or other abuses.This is left to the discretion of individual healthcare workers,[113] several of whom said they only discuss gender-based violence when women have visible signs of physical abuse.[114]In such cases some counselors advise women to contact the VSU or the YWCA,[115] or offer them couple counseling.[116] Staff at the YWCA said that at times hospitals refer women who were injured as a result of domestic violence-and who were receiving treatment for these injuries-to YWCA.[117]
Counselors commonly monitor patients' adherence by counting the pills remaining from the last visit and asking questions if the patient has missed ART doses.Most counselors complete a form, devised by the Centre for Infectious Disease Research in Zambia[118] (see Appendix I), that assists counselors in discussing adherence-related issues with patients.[119]It probes a wide range of reasons why a patient may not have taken their ART, including that the patient forgot, felt too ill, experienced side effects, ran out of medication, was uncomfortable taking the pills in front of others, was disorganized, or had problems swallowing.However, the form does not include questions about violence, including violence against women.Thus, some of the critical barriers to women's adherence to ART remain undetected and unaddressed by healthcare workers.This undermines these facilities' ability to provide appropriate support to women who experience violence.[120]
Probing whether female patients have experienced or fear gender-based violence or other forms of abuse or discrimination including violations of their property rights, in adherence counseling sessions can help women overcome the dehumanizing effects of the abuses described earlier in this report, and would improve women's ability to cope with ART, HIV/AIDS, and violence.[121]Human Rights Watch asked policy-makers, counselors, and other healthcare workers about the feasibility of detecting and responding to gender-based violence by healthcare staff in facilities providing ART.The majority of healthcare professionals and policy-makers interviewed said that, with proper support, it would generally be desirable and feasible to address gender-based violence in their work.Dr. Kamoto Mbewe, reproductive health specialist at the Ministry of Health in Zambia, supported the idea of integrating questions about gender-based violence "because women may hide the abuses, so it is important that [health workers] help those [women]."[122]Elizabeth Serlemitsos, chief advisor at the Zambia National AIDS Council (NAC), said that it would be "realistic" to recommend that adherence counselors ask about domestic violence, but that in rural areas, where there are less community resources, this requires HIV counselors to have basic skills on how to counsel women about gender-based violence.[123]
The manager of planning and development at the Kafue District Health Management Team stated that it "will help us a lot to have these interventions [to address gender-based violence]."[124] Theresa Chidothi, a nurse and counselor in Nangongwe clinic in Kafue, rural Lusaka, said that screening for and addressing gender-based violence was "a welcome idea.We require skills to handle [survivors of gender-based violence]."[125]In terms of time limitations, Theresa Chidothi said, "I think we can manage [in Kafue] because we have set aside a day to [see patients in need of ART]."[126]
In Chongwe, Idah Mthetwa, an ART nurse and adherence counselor, said that it is a "good idea"to probe for and address gender-based violence, but stressed the need for more community-based services, to which counselors could refer women living with HIV/AIDS who are experiencing gender-based violence.[127]
Counselors in Lusaka expressed similar enthusiasm for handling gender-based violence in their clinics, provided that adequate training is secured and adequate space is provided for counseling.[128]Monica Mwachande, senior nurse at Kalingalinga clinic, said that screening for and addressing gender-based violence "could easily be fitted" into adherence monitoring and counseling sessions.[129]Some women will not reveal their experience of domestic violence right away, she said, "but I will at least handle those women, advise them that there are people who can help, for example, the YWCA, the Human Rights Commission, and the VSU."[130]
Vital as it is, this enthusiasm for handling gender-based violence needs to be supported by several practical steps and should be part of an overall strategy to combat gender-based abuses.The practical steps include, but are not limited to, proper training at different levels of health facilities that covers gender-based violence, the availability of protocols that outline ways to address such violence, improving clinic infrastructure, and establishing clear referral channels with existing support organizations.This should be done in partnership with local and international stakeholders given that healthcare facilities in Zambia are already overburdened.The existence of guidelines and models of good practice devised by agencies such as the United States Agency for International Development (USAID), United Nations Population Fund (UNFPA), and the Pan American Health Organization (PAHO) on how to address gender-based violence in health settings can be helpful in guiding this response (see Appendix II).
Training for ART Counselors
Currently, HIV counselors in Zambia must complete eight weeks of training in psycho-social counseling as a prerequisite for certification.[131]Some counselors take additional specialist training in eclectic counseling (diverse areas of counseling), pediatric counseling, adherence counseling, etc.These courses are usually paid for by the counselors themselves or by the institutions they work for.[132]
There are a variety of providers of training for counselors who use training guidelines developed by the Ministry of Health.Some of these providers cover gender relations in their training curricula, but to our knowledge, they seldom cover, systematically, ways to screen for and/or address gender-based violence.The training manager at Kara Counseling told Human Rights Watch that Kara has integrated gender into their courses.[133]The head of the department of counseling studies at Chainama College (which trains counselors and trainers, including those delivering courses at Kara Counseling) also told Human Rights Watch that their curriculum included gender modules, covering the definition of gender, gender awareness, gender as a cross-cutting issue, how to counsel on "gender-conflict," and violence.[134]
The Zambia Counseling Council, a quasi-governmental organization responsible for counselor certification and for monitoring the performance of adherence counselors, has the mandate to de-register counselors who engage in unethical behavior.The Council does not require gender training for counselor accreditation.[135]
Health System Limitations and the Response to Gender-Based Abuses
The availability of ART has contributed substantially to the quality of life for people living with HIV/AIDS in Zambia, especially women.But there are a number of health system constraints that the government has not yet overcome, including a lack of confidential space for counseling; a shortage of human resources; a lack of response to women's inability to afford transportation costs to attend clinic appointments; and inadequate appointment systems, which lead to long waiting hours in clinics.These constraints hinder HIV treatment substantially, as they intersect with women's experiences of domestic violence and other kinds of abuse.
Shortage of Human Resources
One of the main limitations in the health system in relation to ART rollout is the shortage of healthcare workers,[136] especially medical doctors,[137] in Zambia. Shortages of trained healthcare workers, according to the government's Gender in Development Division, reduce "access to health services for the victims of violence."[138]
To address human resource limitations and facilitate treatment rollout, the government has trained clinical officers, nurses, and midwives, and accorded them the additional responsibility of providing HIV treatment and care, following standard care protocols.[139]However, HIV counselors currently are not on the government's payroll and are also poorly paid: a counselor typically earns between Kw25,000 and Kw35,000 (between $6 and $9) per day.[140]To increase the number of nurses and midwives, the government is opening a number of nursing schools and they have reduced the number of years required for midwifery training.The reproductive health specialist at the Ministry of Health told Human Rights Watch that in addition to these steps, the government has a human resources plan and has taken measures to increase the number of health professionals in rural areas.[141]
Inadequate Infrastructure
Sufficient clinics with space for counseling, at a reasonable distance from patients' homes, are important factors in the delivery of quality HIV services.Unfortunately, many of the women and counselors interviewed for this report complained about long distances to clinics and the lack of adequate space for counseling.Women who were impoverished, often as a result of property grabbing or unequal distribution of marital property upon divorce, said that as a result of high transportation costs to far-away clinics, they miss clinic appointments.
Without sufficient private and confidential space for counseling, women may not be comfortable disclosing and discussing gender-based violence.[142]Some clinics lack the space necessary to ensure privacy and confidentiality for HIV patients.For example, the Lusaka-based Kalingalinga and Kamwala clinics, run by the government with support from CIDRZ, where a counselor sees between 70 and 110 patients per day, have one adherence-counseling room each.Counselors must either wait for their colleagues to complete their adherence sessions before seeing their clients, or use the same room for more than one session simultaneously, thus compromising patient confidentiality, privacy, and the general quality of service.As one supervisor in an HIV clinic in Lusaka put it,
The complaints that counselors come with [include the problem that] the clinics are congested. The space is so squeezed and used to be a ward.At least if we had three rooms in the clinic for adherence counseling, we would not have to wait outside until the room is free.[143]
A counselor in Lusaka told us,
Space is the biggest issue.Because of lack of infrastructure, you see in one side[of a counseling room], someone is getting blood, maybe CD4 count, and another counselor is giving adherence counseling in the same room.[144]
The number and location of clinics determine how easy they are to reach.Chapter V discusses the drastic effects that property grabbing and insecure property rights upon divorce have on women's ability to afford transport to far-away clinics.This is particularly problematic in rural areas.A woman who lives in Chongwe, rural Lusaka, said that she had to pay Kw20,000 (about $4.80) for transportation every time she visited the clinic and that "the government should bring clinics nearer to people."[145]
Recognizing the transport challenge, clinics budget for emergencies that might prevent patients from renewing their prescriptions on time: two to three days' worth of extra pills are provided with each dispensation of ART and clinics also allow pre-registered family members or "buddies" to collect the medicine on behalf of patients if needed.[146] However, this is not always effective for women affected by gender-based violence who are hiding their status from their husbands and other family members.When asked about the steps taken to improve patients' access to care, the district commissioner of Chongwe, a district that has 300 trained counselors,[147] said that the government provided thirty bicycles and motorbikes for the district's 28 clinics, including clinics providing ART, so healthcare staff can reach patients who are unable to attend clinics due to distance or poor road networks.[148]
The director of Lusaka's District Health Management Team also said that that the Zambian government has increased the number of clinics delivering ART-related services in Lusaka and a number of other provinces, and expanded some of the clinics to provide more space for ART services.[149] As of October 2006 there were thirty-one sites in Lusaka supported by CIDRZ, one of the largest agencies supporting ART service delivery in Zambia.[150]
Lack of Appointment Systems
Most healthcare facilities that provide ART lack of appointment systems, which allow patients to make appointments in advance.This compounds the problems that women affected by gender-based abuses encounter in their daily lives and impacts their adherence to ART.The only clinic that has an appointment system that Human Rights watch identified in its research was the Kara Clinic.The director of the Lusaka DHMT said that introducing an appointment system in Zambia will be difficult given that patients might not be able to arrive on time.[151]
As discussed earlier in this report, the violence and other abuses that women experience in Zambia sometimes compel women to hide their HIV status from their husbands, partners, and other family members.In such circumstances women have to make up explanations for their trips to attend clinic appointments, such as telling their husbands that they are visiting relatives or attending a funeral.In the absence of an appointment system, women end up waiting long hours at clinics.A number of women testified that they experienced violence at the hands of their husbands for arriving home late from clinics and for failing to prepare the food on time.Then women must also wait at clinics without food.One woman who told Human Rights Watch that her husband beats her up for the slightest delay, even if she was buying vegetables in the market, said, "The problem is when I go to the clinic to get ARVs.I go there six in the morning and come back at 20:00 hrs.They don't give you food, so when it is time I drink my medicine without food."[152]
The Role of Women's Organizations in AIDS Programs and Community-Based Support
Community-based support is an important element of a successful AIDS response, including in terms of receiving and responding to referrals from healthcare facilities addressing gender-based abuses.In Zambia, particularly in urban settings in Lusaka and the Copperbelt provinces, there is a wide range of women's organizations and other nongovernmental organizations and community-based organizations that provide services to women affected by gender-based abuses, including domestic violence and lack of enjoyment of property rights.Yet currently there are almost no formal referral paths between health facilities providing ART and these organizations.Counselors often refer patients on ART to support groups associated with the health facility or run by nongovernmental or faith-based organizations that address the needs of adults and children living with HIV/AIDS.But Human Rights Watch knows of no specialized support groups dealing with gender-based violence that are associated with healthcare facilities providing ART.
In terms of addressing the financial vulnerability of women living with HIV/AIDS, including food security, there are a number of international organizations, such as CARE International and Oxfam, that are implementing programs that provide income support and food security for people living with HIV/AIDS.Some of these organizations are linked to ART providers.[153]
Addressing the gender-specific problems that arise from health system policy and infrastructural problems discussed above may materialize through better representation of women and women's organizations in health and HIV policy and coordination bodies.The essential role of women in decision-making and as full partners in relation to the national and international fight against AIDS has become evident and increasingly recognized globally.[154]
NAC, the organization that coordinates Zambia's national response to HIV/AIDS, works in partnership with a wide range of stakeholders, including civil society representatives.These stakeholders influence the HIV/AIDS response in Zambia through participation in thematic groups.While the NAC includes youth groups, faith-based groups, traditional healers, and other stakeholders in its thematic groups, there is no thematic group specific to women.NAC officials told Human Rights Watch that they were planning to contact the Non Governmental Organizations' Coordinating Council for Gender and Development (NGOCC), a network of women's organizations in Zambia with over eighty member organizations, to form a women's specific thematic group.[155] Developing a women's thematic group within the NAC would improve its ability to identify and address the needs of women living with HIV/AIDS or accessing treatment.
Legal Framework and Access to Justice
Despite several positive reforms, the legal framework and justice system in Zambia fall short in providing the necessary respect for and protection of women's rights, as required by Zambia's human rights obligations.
The Constitution
Zambia's constitution is currently undergoing a review process, which is likely to conclude in 2009.Although the existing constitution contains language that forbids discrimination on the basis of sex (article 23), this provision specifically excludes from its application key areas of personal and customary law.[156]Given that customary law has traditionally been a source of discrimination against women in Zambia, this exclusion undercuts the ability of women married according to customary law to seek redress for violations of their rights.
The draft constitution, published for discussion in 2006, contains new language that would remedy this and other shortcomings in the current constitution.Articles 38-40 of the draft provide that every person is equal before the law and has the right not to be discriminated against on any ground, including on the ground of sex; that women and men have equal rights to property and inheritance; and that "any law, culture, custom or tradition that undermines the dignity, welfare, interest or status of women or men is prohibited."[157]
Legislation on Gender-Based Violence
Zambia has no specific legislation to address domestic violence, so women must resort to the general penal code provisions on assault occasioning bodily harm.[158]Penalties vary depending on the gravity of injury and on whether the assailant used a weapon.Weak criminal provisions and the lack of other sufficient civil enforcement mechanisms mean that many women, particularly poor women, may be forced to choose between having their husbands arrested and incarcerated or keeping an abusive breadwinner in the family home.Officers in the VSU, officials at the Zambia Human Rights Commission, and staff members of Women in Law and Development in Africa (WiLDAF) and Women and Law in Southern Africa (WLSA) told Human Rights Watch that complainants often withdraw charges against abusive husbands who have been arrested and imprisoned.[159] In their experience this is because women lack access to financial resources and depend on their spouses for food and shelter.It is also due to social pressure.Women have withdrawn charges against abusive partners even where they received free legal services, for example, through the Centre for Coordinated Response to Sexual and Gender-Based Violence known as the "one-stop center" where women survivors of domestic violence receive free legal support.According to the director of the center, 50 percent of the cases that the center addresses, especially in the area of domestic violence, are withdrawn.[160]
The Penal Code does not specifically criminalize marital rape.Chapter XV, Section 132, of the penal code defines a rapist as: "[a]ny person who has unlawful carnal knowledge of a woman or girl, without her consent, or with her consent, if the consent is obtained by force or by means of threat or intimidation of any kind, or by fear of bodily harm, or by means of false representations as to the nature of the act, or, in the case of a married woman, by personating [sic] her husband."[161]
It has been suggested that one problem is that the definition of rape and the law do not foresee the possibility of "unlawful" carnal knowledge of one's wife.[162] This would be consistent with the customary social understanding that the payment of "lobola" [dowry] creates an obligation on a woman to be sexually available when her husband so demands.[163]
A new proposed bill, the Sexual Offences and Gender Violence Bill (2006), which WiLDAF drafted in consultation with other nongovernmental organizations, addresses sexual offenses and violence against women and girls in and outside the home.It also introduces new provisions relating to domestic violence.The draft bill contains a definition of domestic violence which incorporates physical, sexual, and psychological violence.[164]It introduces a system of remedies in the form of protection orders for victims of domestic violence and criminalizes marital rape.[165]The bill also proposes the establishment of a specialized court for sexual offenses and gender violence, with trials and procedures that are less intrusive into the lives of survivors of sexual abuse.[166]Human Rights Watch understands that the draft Sexual Offences and Gender Violence Bill was presented to Parliament in 2006 but was then withdrawn for further consultation.[167]
In its 2006 report on compliance with the Southern African Development Community's Declaration on Gender and Development and its addendum on the prevention of violence against women and children, the Zambian government reported, "On the issue of gender violence, Government has demonstrated its resolved commitment to reduce and/or eradicate gender based violence by amending the Penal Code which has domesticated in part the provisions of the Convention on the Elimination of All Forms of Discrimination against Women (CEDAW) as they relate to violence against women Act no. 15 of 2005 has stiffened the penalties for perpetrators of sexual violence."[168]
Property Rights in Statutory and Customary Law
Women's rights to acquire, administer, enjoy and inherit property, including upon divorce, are inadequately protected under Zambian law.The protections that do exist are poorly enforced.In terms of property rights upon divorce, the Matrimonial Causes Act, which is awaiting presidential approval as of October 2007[169] and applies to marriages covered by article 3 of the Marriage Act,[170] provides for property-related settlements in court upon divorce, instead of current practices where it is often assumed that the matrimonial property belongs to the husband. The Act is silent in relation to equal division of property upon divorce.
Since many people in Zambia prefer to marry according to customary law rather than according to the civil marriage statute, the protections of the Matrimonial Causes Act, once in force, will not apply to them.[171]As mentioned earlier in this report, customary law generally discriminates against women in divorce.The Zambian government describes customary law as "unwritten, patriarchal," and administered by "non-professional justices who are predominantly male."[172]
Inheritance is another area where customary laws discriminate against women.Under the customary laws that most Zambian ethnic groups practice, couples do not own property jointly, and traditions in most ethnic groups stipulate that the deceased husband's family retains all inheritance rights.The World Bank's report, Engendering Sustainable Growth in Zambia, states that compared to men, "women [in Zambia] have much lower prospects of inheriting marital assets, land, or money even when the deceased party is their spouse.In matrilineal communities only persons related to the deceased through the deceased's mother or more remote female ancestor are eligible to share in the estate.In patrilineal communities eligibility is limited to those related to the deceased through a common male ancestor."[173]
The Intestate Succession Act of 1989 was intended to "make adequate financial and other provisions for the surviving spouse, children, dependents and other relatives" of people who die without leaving a will.[174]The Act allocates 20 percent of the property to the widower or widow, 50 percent to the children, 20 percent to parents of the deceased, and 10 percent to other dependents.[175]Where local courts have jurisdiction, they often do not enforce the Intestate Succession Act.Instead, they use the Local Courts Act to distribute inheritance without reference to the percentages specified by the Intestate Succession Act, and often mandate low fines for property grabbing.Thus, in many cases, widows receive little inheritance.[176]
The Zambian government has responded to women's insecure property rights under customary law by initiating consultations with traditional chiefs on the need to change practices that discriminate against women in terms of access to land.[177]Some women's organizations, such as Women for Change and WLSA, are also working closely with traditional leaders and chiefs in a number of provinces to bring change in the way they handle women's access to land and property.[178]Moreover, government representatives and women's rights activists told Human Rights Watch of government's preliminary efforts to revise and codify customary law so that it is consistent with statutory law and does not discriminate against women.[179]
The Victim Support Unit
In 1994 the Zambian government established the Victim Support Unit of the police department (VSU) in response to gender-based abuses.The VSU has officers in police stations in Zambia's nine provinces.
Although the existence of the VSU is an indication of political will to address gender-based abuses, there are serious problems that undermine its ability to carry out its functions effectively. Like other government institutions in Zambia, the unit lacks resources.[180]The head of the Community Service Department of the Zambian police (of which the VSU is part) and Zambian activists[181] told Human Rights Watch that the unit lacks paper and sexual crime forensic kits.The head of the Community Service Department told Human Rights Watch that the one vehicle that the VSU had was out of service.A nurse counselor in Kafue told Human Rights Watch that she tried to help women patients who had visible signs of physical violence to report their husbands to the VSU, but that VSU officers said they had no transport or were short staffed, and unable to help the women.[182]
The head of Community Services Department also said that staffing levels were inadequate compared to the responsibilities of the VSU.In Lusaka province, which has the highest number of VSU officers, there are 120 VSU officers based in 21 stations who are also deployed as "foot officers" in unplanned settlements.[183]Given that the total population of Lusaka province is 1.39 million[184] of which females constitute 685,551,[185] this means that there is one VSU officer for every 5,713 women and girls in Lusaka province.
Due to high staff turnover,[186] and the lack of a system of ensuring that officers are trained regularly,[187] fewer than half of the VSU officers are properly trained to handle victims of violence.[188]YWCA staff members also raised the problem of high staff turnover at the VSU.The YWCA held several training workshops on gender-based violence, only to have the officers who received the training move to other departments.[189]According to the head of the Community Services Department, about 40 percent of the staff members are trained in psychosocial counseling.By February 2007 only six VSU officers had completed training on HIV and on dealing with survivors of sexual violence.With the exception of the Center for Coordinated Response to Sexual and Gender-Based Violence, the rooms allocated for VSUs are often not adequate to ensure privacy for victims and survivors of sexual violence.[190]
Although many of the women living with HIV/AIDS and activists in women's rights organizations we interviewed praised the attitudes of VSU personnel, there were concerns about the behavior of some individual VSU officers and of the police in general, which at times deter women from accessing VSU services.For example, in some cases, the police encouraged reconciliation rather than pursuing reports on domestic violence.[191]A legal advisor at WilDAF told Human Rights Watch that officers at the VSU asked a 17-year-old girl whose father had raped her repeatedly since she was 11, "In [your area] there are no boys of your age? ... For you to have an affair with your father you must like him."[192] The same legal advisor also told Human Rights Watch that VSU officers said to a widow who reported a case of property grabbing, "You should be mourning your husband, and you are worried about a fridge?"[193]
A number of women interviewed by Human Rights Watch reported cases of corruption among police officers.One woman said that she believes her former husband bribed VSU officers, and as a result, they stopped pursuing him to pay maintenance as per a court's decision.[194]Another woman said that her bedridden sister's former partner-who appropriated Kw4.5 million (US$1,084) from her inheritance-bribed the VSU and as a result they delayed her sister's case.[195]
Legal Aid
One of the major problems that women who experience gender-based abuses-especially property grabbing and unequal distribution of their marital property upon divorce-is obtaining information on their legal rights and representation in court cases.The Zambian government established a legal aid department that provides free legal aid for those who cannot afford to cover legal costs.However, a number of those interviewed said that this department failed to have a meaningful impact due to its limited capacity and resources.Lawyers at nongovernmental organizations said that there were only four legal aid lawyers who cover Lusaka, Ndola, Kitwe and Livingstone districts.Denial of women's property rights is apparently not a priority, as the focus is often on crimes such as murder or aggravated robbery.[196]
WLSA reported that because of the lack of financial and human resources, the Legal Aid Department was "a myth in the lives of many Zambians, particularly women."[197]In its initial report on the implementation of the African Charter on Human and Peoples' Rights, the Zambian government stated, "Though the Legal Aid Department is set up for the benefit of the entire population, it is restricted in its operation by serious financial constraints, which limit its ability to reach out to a wider section of the population" and that "[v]ery few people are aware of the functions of the Legal Aid Department."[198]
As such, property rights violations and other abuses in the domestic sphere are often taken up by civil society organizations such as WLSA, WILDAF, the International Justice Mission, and the Women's Legal Aid Clinic of the Zambia Law Society.
Shelters and Social Support Services
Zambia's government has not provided shelters for women and girls who are survivors of violence and other forms of abuse.The only two shelters in the country are run by the Young Women's Christian Association.YWCA staff told Human Rights Watch, "We only have one shelter in Lusaka and it is constantly full, as it can only accommodate up to 13 women and their children.We are advocating with the government [for the establishment of] a social housing unit for women who need it."[199]YWCA is in the process of establishing another shelter outside Lusaka. YWCA's shelter in Lusaka is supported through funds generated by YWCA's small businesses, and through funds from Scandinavian countries.The Ministry of Youth and Sports provides YWCA with monthly funding toward the organization's food support programs for children in crisis.The organization also receives small grants from the Gender and Development Division.[200]
One positive development is the establishment of the multi-agency Centre for Coordinated Response to Sexual and Gender-Based Violence, the one-stop center mentioned earlier, a partnership between the government (Zambia's police and judiciary) and civil society organizations (YWCA, Zambia Society for Prevention of Child Abuse and Neglect, WLSA, and Care Zambia).[201]The center provides integrated police, legal, counseling and health services to women.It works closely with the University Teaching Hospital, to which it refers victims of sexual abuse who need medical treatment.The center also receives general referrals from the University Teaching Hospital.
Gender Policies
Zambia has a number of policies and governmental bodies that specifically address gender-based abuses.The National Gender Policy (2000) outlined concrete measures for the government to address gender-based violence.The government made a commitment to:
(a) promote awareness through campaigns to change harmful and negative cultural practices of society especially by health and media personnel, the police and other security and defense agencies toward gender issues; (b) encourage victims, through appropriate mechanisms, to report cases of all forms of violence and sexual abuse to the relevant law enforcement agencies; (c) establish a mechanism to co-ordinate the effort of the police, social welfare workers and legal personnel in dealing with cases of gender violence; (d) expand and strengthen the operations of the police victim support unit to effectively cover the entire country; (e) build capacity among law enforcement agencies to handle cases of gender violence by increasing their skills in counseling, psychology, social work, gender and human rights; (f) establish and encourage institutions dealing with rehabilitation of victims of gender violence; (g) promote and conduct awareness campaigns targeted at women and men on the existence of legal provisions in the Penal Code, Intestate Succession Act and other laws protecting women and those with disabilities against violence, sexual harassment and abuse; and (h) improve women's participation in law enforcement and crime prevention.[202]
The Strategic Plan of Action for the National Gender Policy (2004-2008)lists as government priorities the establishment of mechanisms to coordinate efforts to address gender-based violence, to "strengthen, enact and/or amend gender discriminatory laws and procedures," to "facilitate reporting of all forms of gender violence," and to build the capacity of the law enforcement agencies to handle cases of violence.As discussed above, the Fifth National Development Plan also lists gender-based violence as a major problem.
Zambia has a Gender in Development Division (GIDD), which still operates under the Cabinet Office, although the president of Zambia has appointed a cabinet-level minister of gender and development in 2006.[203]The GIDD is responsible for coordinating the implementation of the Gender Policy, and has a very limited capacity in terms of financial and human resources.[204]The budget allocated to GIDD in 2007 was Kw3.43billion (about US$902,656) out of a total budget of Kw12.04trillion (about US$3.17billion).[205]The Minister of Finance told Human Rights Watch that GIDD received relatively fewer resources because resources earmarked for gender-related projects are also allocated to other ministries such as the Ministry of Education, to cover girls' education, for example.[206]Still, the mere .04 percent of the total national budget allocated specifically for gender is unacceptably low.
In 2000 the Zambian government drafted the National Plan to End Gender-Based Violence, in line with the SADC Addendum on the Prevention and Eradication of Violence against Women and Children.The plan outlined legal, socioeconomic, cultural, and political factors, as well as education, awareness, and training as key areas for action.However, this plan remained in draft form until 2007,[207] when GIDD revisited it.In August 2007 a number of nongovernmental organizations including YWCA, NGOCC, and the Zambia Media Women's Association submitted the Zambia 365 Day Action Plan to End Gender-Based Violence[208] to the Gender and Development Division for government endorsement[209] and incorporation in the National Plan to End Gender-Based Violence.[210]
The Role of NGOs
NGOs in Zambia play an important role in filling gaps created by the shortfall in the government's response to gender-based abuses in the context of HIV/AIDS.In addition to the roles of organizations that provide diverse services for women affected by gender-based abuses discussed in this chapter, some organizations also build the skills of women living with HIV/AIDS so they can cope better with HIV/AIDS and generate income.Hope House, which is part of Kara Counseling, trains women living with HIV/AIDS on "positive living" and income generation.Participants in this program receive funds for transportation.Another program, the Circles of Hope, consists of more than 30 Lusaka-based support groups for people living with HIV/AIDS (particularly women and girls).Affiliated with the Council of Churches in Zambia, the Circles of Hope program provides peer support on coping with HIV, violence against women, and property grabbing.It also supports women to establish income-generating projects.[211]
A number of organizations are also delivering training and gender-sensitization to judges.These include Zambia Aids Law Research and Advocacy Network (ZARAN), WiLDAF, and WLSA, all of which either receive little or no government funding.
VII. Zambia's International Legal Obligations
Although the Zambian government has taken impressive steps to address some of the gender-based abuses covered in this report and to address the need for free ART by adults and children living with HIV/AIDS, it is falling short of many of its human rights obligations to women, including women living with HIV, under international law.[212]
Violence against women, including domestic violence, raises a range of human rights abuses that governments have a direct responsibility to address.For example, domestic violence violates a woman's rights to dignity, personal freedom, and physical integrity, as well as their right to freedom from cruel and inhuman treatment.Governments have positive obligations to protect against violations of these rights, even if the perpetrator is a non-state actor, such as a spouse or partner.
International human rights law makes clear that violence against women is a form of gender-based discrimination that governments must eliminate.Zambia is a party to the Convention on the Elimination of All Forms of Discrimination against Women (CEDAW).[213] The CEDAW Committee has on several occasions made clear that the definition of discrimination under the treaty includes gender-based violence as it is "violence that is directed against a woman because she is a woman or that affects women disproportionately.It includes acts that inflict physical, mental or sexual harm or suffering, threats of such acts, coercion and other deprivations of liberty.Gender-based violence may breach specific provisions of the Convention, regardless of whether those provisions expressly mention violence."[214]
Regional treaties to which Zambia is also bound, namely the African Charter on Human and Peoples' Rights, also enshrine the principle of non-discrimination on several grounds, including sex.[215]The Charter calls on all states to eliminate "discrimination against women" and to ensure the protection of the rights of women, as specified in international human rights conventions.[216]
The Protocol to the African Charter on Human and Peoples' Rights on the Rights of Women in Africa (the African Women's Rights Protocol), which Zambia ratified in May 2006, clearly states that "every woman shall have the right to dignity inherent in a human being and to the recognition and protection of her legal and human rights."[217] The protocol further protects women's rights to life, integrity, and security of the person.[218]It prohibits all forms of cruel, inhuman, or degrading treatment and calls upon states parties to take appropriate and effective measures to:
a) enact and enforce laws to prohibit all forms of violence
against women including unwanted or forced sex whether
the violence takes place in private or public;
b) adopt such other legislative, administrative, social and economic measures as may be necessary to ensure the prevention, punishment and eradication of all forms of violence against women;
c) identify the causes and consequences of violence against women and take appropriate measures to prevent and eliminate such violence; .
f) establish mechanisms and accessible services for effective information, rehabilitation and reparation for victims of violence against women.[219]
Zambia also made political commitments to "take urgent measures to prevent and deal with violence against women" by signing the SADC Declaration on Gender and Development and its addendum on the Prevention of Violence Against Women and Children.
The accounts of women affected by gender-based violence documented in this report, and the government's lack of adequate response documented in Chapter VI above indicate that the Zambian government must do more to protect women from gender-based violence and to meet its obligations under international human rights law.The inadequacy in addressing violence against women has placed tremendous constraints on women's HIV treatment and is generally reflected in the high-levels of gender-based violence in the country in the absence of effective deterrence.The lack of adequate government response to gender-based violence is also reflected in the wide range of services that nongovernmental organizations provide.
The International Covenant on Economic, Social and Cultural Rights (ICESCR), to which Zambia is also a party, specifically requires states to take steps to achieve progressively the full realization of the right to "the enjoyment of the highest attainable standard of physical and mental health."[220]General Comment 14 of the Committee on Economic, Social and Cultural Rights (the Committee), the independent panel of experts that monitors the implementation of the ICESCR, recommends that states "integrate a gender perspective in their health-related policies, planning, programs, and research in order to promote better health for both women and men."[221]The Committee further recommended that states remove all barriers interfering with women's access to healthcare services.[222]
The Committee stressed the importance of developing national strategies to eliminate discrimination against women, including the protection of women from domestic violence to reduce their health risks.[223] According to the Committee, "the failure to protect women against violence or to prosecute perpetrators; [and] the failure to discourage continued observance of harmful traditional practices,"[224] amount to violations of the states' obligation to protect women's right to health.The Committee further stipulates that "the failure to take measures to reduce the inequitable distribution of health facilities, goods and services, [and] the failure to adopt a gender-sensitive approach to health,"[225] amount to violations of the states parties' obligations to fulfill the realization of the right to health.[226]
Ensuring that health facilities that provide ART are capable of detecting and responding to gender-based violence would remove a significant barrier that women with HIV experience when accessing appropriate health services, including ART.This would also help to address domestic violence and the needs of women whose rights have been violated by it.In order to meet its obligations to protect and fulfill women's right to health, Zambia must take measures that will help protect against domestic violence and facilitate access to health services for women living with HIV/AIDS who have been abused.
International human rights law also safeguards women's right to equal enjoyment of property rights, including in areas of inheritance and allocation of property upon divorce.CEDAW specifically obliges state parties to "accord to women, in civil matters, a legal capacity identical to that of men. In particular, [states] shall give women equal rights to conclude contracts and to administer property and shall treat them equally in all stages of procedure in courts and tribunals."[227] CEDAW also requires states to take appropriate measures to ensure equal rights and responsibilities in marriage and divorce.[228]It accords the same rights to both spouses "in respect of the ownership, acquisition, management, administration, enjoyment and disposition of property."[229]
Zambia's obligations concerning women's equal property rights are further defined in General Recommendation 21 by the CEDAW Committee,[230] which states, "The right to own, manage, enjoy and dispose of property is central to a woman's right to enjoy financial independence, and in many countries will be critical to her ability to earn a livelihood and to provide adequate housing and nutrition for herself and for her family."[231]The CEDAW Committee further affirms that "any law or custom that grants men a right to a greater share of property at the end of a marriage or de facto relationship, or on the death of a relative, is discriminatory and will have a serious impact on a woman's practical ability to divorce her husband, to support herself or her family and to live in dignity as an independent person."[232]
Like CEDAW, the African Women's Rights Protocol requires states to enact legislation to guarantee equality between women and men in marriage,[233] and in cases of separation, divorce, or annulment of marriage.[234]The protocol stipulates married women's right to own and manage their own property freely.[235] The protocol further affirms that upon separation or dissolution of marriage, "women and men shall have the right to an equitable sharing of the joint property deriving from the marriage."[236]
International law also affirms women's equal rights under laws relating to inheritance.General Recommendation 21 of the CEDAW Committee states: "There are many countries where the law and practice concerning inheritance and property result in serious discrimination against women. As a result of this uneven treatment, women may receive a smaller share of the husband's or father's property at his death than would widowers and sons .Often inheritance rights for widows do not reflect the principles of equal ownership of property acquired during marriage. Such provisions contravene the Convention and should be abolished."[237]
The experiences of women documented in this report indicate that the property rights of women who marry under customary law are often violated with impunity, and that despite the existence of the Intestate Succession Act, property grabbing is still practiced.By failing to ensure that women enjoy and can enforce their property rights, the Zambian government is failing to meet its legal obligations discussed above.
International human rights instruments also set out what protections should exist against abuses linked to individuals' HIV status.The Office of the High Commissioner for Human Rights' and UNAIDS's international guidelines on HIV/AIDS and human rights provide a road map for governments to enable them to effectively incorporate human rights protections linked to HIV/AIDS into national law.The guidelines cover the elimination of violence against women (including harmful traditional practices, sexual abuse, and exploitation), protection against discrimination, the need for legislation to address public health issues related to HIV/AIDS, and reform of criminal law to ensure consistency with international obligations.[238]Zambia still does not have specific laws that address discrimination against people living with HIV/AIDS, although a process to develop an HIV/AIDS human rights charter has started.[239]
VIII. Response of the International Community
Since the start of 2000 the global response to HIV/AIDS pandemic has seen much-needed improvement.In 2000 the G8 countries acknowledged the need for resources to combat HIV/AIDS, and African leaders confirmed this need for resources in Abuja in 2001.The United Nations General Assembly Special Session (UNGASS) on HIV/AIDS in 2001 concluded with a firm commitment to create a global fund to fight HIV/AIDS.World leaders made commitments in the Millennium Development Goals (MDGs) to promote gender equality and empower women (MDG 3) and to combat HIV/AIDS, malaria, and other diseases (MDG 6) by halting and beginning to reverse the spread of HIV by the year 2015.Significant initiatives have been launched and significant resources mobilized to fight the pandemic and rollout treatment.
In September 2003 the World Health Organization (WHO) and UNAIDS launched the "3 by 5" initiative, aiming to have three million people in need of HIV treatment on ARVs by the end of 2005.This included two million people in the African continent, and 1,297 million people in East and Southern Africa.[240]In 2003 the US government created the President's Emergency Plan for AIDS Relief (PEPFAR).All these initiatives and political commitments enabled countries in the global South with sufficient political will to roll-out HIV treatment.
In 2005 leaders of the G8 pledged to "work with WHO, UNAIDS, and other international bodies to develop and implement a package for HIV prevention, treatment, and care for all those who need it by 2010."Member States of the UN endorsed this goal at the High-Level Plenary Meeting of the UNGASS in September 2005.At the UNGASS High-Level Meeting on AIDS in 2006, the states agreed to work toward the goal of "universal access to comprehensive prevention programs, treatment, care, and support" by the year 2010.[241]
The gender dimensions of HIV/AIDS in Southern Africa, the sub-region most affected by the pandemic, received relatively better attention, thanks, among other factors, to advocacy by women's NGOs and concerned UN personnel: the former UN special envoy for HIV/AIDS in Africa, Stephen Lewis, and the executive director of the World Food Program, James Morris,[242] recommended "urgent action in addressing the gender dimensions of HIV/AIDS in Southern Africa."[243] In response the former UN Secretary-General established a task force on women, girls and AIDS in Southern Africa to focus on improving the response to HIV/AIDS in nine countries of the sub-region, including Zambia.The task force focused on six areas, including property and inheritance rights, and violence against women and girls.[244]
The global political commitments to address HIV/AIDS translated into increased-although not sufficient-financial resources.In turn, the number of people receiving ART in Africa grew from just 100,000 in 2003, to over one million by December 2006.[245]Resources from the Global Fund to Fight HIV/AIDS, Tuberculosis and Malaria (Global Fund), PEPFAR, and other bilateral, multilateral, and private donor resources, played a major role in this increase in the number of people receiving treatment.
The rest of this chapter outlines the role of the two largest contributors to Zambia's HIV treatment programs, namely the United States (US) government and the Global Fund in responding to some of the abuses described in this report.
The United States
The US government is one of the major donors in Zambia, particularly in the area of HIV/AIDS, including support for HIV treatment programs through PEPFAR.[246] Under PEPFAR Zambia received more than US$81.6 million in 2004, about $130.1 million in 2005, and approximately $149 million in 2006 to support HIV/AIDS prevention, treatment and care programs.[247]PEPFAR is providing $216 million in fiscal year 2007.[248] Funds are disbursed to "partner organizations" and "sub-partners" and are used to cover a wide range of HIV services and activities.
In its various documents, the Office of the US Global AIDS Coordinator (OGAC), which coordinates PEPFAR, recognizes the importance of adopting service delivery models that potentially reduce client risk of gender-based violence, and also of supporting interventions that enhance women's decision-making power in the private and public spheres.[249] However, a number of international AIDS advocacy organizations have criticized PEPFAR's response to gender-based violence.[250]
In terms of addressing gender-based violence and other abuses in Zambia, officials in the major US agencies tend to link their program interventions to the White House Women's Justice and Empowerment Initiative (WJEI).Announced by the US president in June 2005, WJEI is a $55 million initiative that aims to support ongoing activities to promote women's empowerment and their access to justice in four African countries, including Zambia.[251]The initiative is supposed to strengthen the capacity of the legal system so it can protect women through training of the police, prosecutors, and judges in areas of gender-based abuses, including sexual violence.The initiative also aims to strengthen laws that protect women, such as the Sexual Offences and Gender Violence Bill in Zambia, improve the capacity of shelters, and address women's health needs.[252]According to the US State Department, "WJEI funds will help raise awareness about gender-based violence, protect and assist victims of rape and domestic violence, and bring justice to perpetrators of violence."[253]
The implementation of WJEI has unfortunately been substantially delayed.As of November 2007-that is, over two years since the start of the program-no WJEI funds had actually been disbursed for projects in Zambia.According to the officer in charge of WJEI at the US Department of State, the process of disbursing the funds involved planning, identification of needs on the ground, and ways to complement existing programs.[254]
In terms of specific programs addressing gender-based violence and unequal property rights, the second secretary at the US Embassy in Lusaka told Human Rights Watch, "We tend to integrate gender into all of our programs [including in the areas] of justice and legal reform."[255]Potential future areas of support indicated by diplomats at the US Embassy in Lusaka include the establishment of shelters (mainly for victims of trafficking), and establishing additional one-stop centers.[256]The US Embassy in Lusaka also has a small grants program.
PEPFAR Reauthorization and Debates on Prevention and Treatment Approaches
The law that created PEPFAR is up for reauthorization in 2008.One of the main areas of contention around reauthorization is the allocation of resources in the area of HIV/AIDS prevention.In 2003 Congress required that 55 percent of PEPFAR money be allocated toward HIV treatment, 15 percent toward palliative care for individuals with HIV/AIDS, 10 percent toward helping orphans and vulnerable children, and 20 percent toward HIV prevention.[257]However, at least 33 percent of the prevention funds were earmarked to be spent on abstinence-until-marriage programs, which attracted tremendous criticism from local, regional, and international organizations, including Human Rights Watch.[258]PEPFAR's policies on prevention have been described as "ill informed and ideologically driven."[259]
The frustration of Zambian AIDS activists with the US prevention strategies was evident during the visit of US First Lady Laura Bush to Zambia and a number of other African countries in June 2007.The founder of Health Triangle Trust, which addresses HIV/AIDS, tuberculosis, and malaria, stated that "the good work that the US is doing in providing treatment and care [in Zambia] will come to nothing as long as new infections are not prevented. We are therefore, demanding that the US reconsider its policy on HIV prevention and other reproductive rights issues in order to stop new infections."[260] Abstinence-until-marriage and fidelity programs, stated the Health Triangle Trust, "do not take into consideration the social, cultural and economic contexts that people live in. To simply promote faithfulness without taking into consideration the power play that exist between women and men in [Zambia] is not only ineffective but also puts the women at risk of contracting HIV from their spouses."[261]
Similarly, the Treatment Advocacy Literacy Campaign (TALC) issued a press statement on the visit of First Lady Laura Bush to Zambia, stating that the conditionalities attached to US government funding for HIV prevention programs were likely to undo the impressive gains made in the area of HIV treatment in Zambia.
The Protection against Transmission of HIV for Women and Youth Act (PATHWAY) bill proposed by Congresswoman Barbara Lee would abolish the requirement to allocate 33 percent of prevention money to abstinence-until-marriage HIV prevention programs.It also requires the president and OGAC to establish a comprehensive HIV prevention strategy that addresses the vulnerabilities of women and girls to HIV infection in all countries that receive US HIV assistance.[262]
Another proposed law, the African Health Capacity Investment Act of 2007, is particularly important in addressing the disastrous lack of capacity in the healthcare system in Zambia and other countries affected by HIV/AIDS in sub-Saharan Africa.The bill aims to enhance the efforts to achieve internationally recognized goals in the treatment and prevention of HIV/AIDS and other major diseases and the reduction of maternal and child mortality by improving human health care capacity and improving retention of medical health professionals in sub-Saharan Africa.[263]The bill would amend the Foreign Assistance Act of 1961 and authorize the US president to provide assistance for programs to improve health infrastructure and retain healthcare workers in sub-Saharan Africa.The Act would also direct the US president to develop a strategy to coordinate, implement, and evaluate assistance programs to build the healthcare capacity in Africa.The Act proposes appropriations of $150 million, $200 million, and $250 million for the fiscal years 2008, 2009, and 2010, respectively.[264]
The Global Fund to Fight HIV/AIDS, Tuberculosis and Malaria
The Global Fund is one of the main resource providers in Zambia's HIV sector, including in the area of HIV treatment rollout.In funding rounds one (2003) and four (2005), the Global Fund approved a total of $322.22 million toward HIV programs in Zambia.By January 2007 the Global Fund had disbursed $93.10 million of these funds.However, little of this money covers gender-based violence or gender-specific projects.[265]
The Global Fund has four main recipients in Zambia: the Ministry of Finance and National Planning, the Ministry of Health, Church Health Organizations in Zambia, and Zambia National AIDS Network.The Global Fund works through a country coordinating mechanism (CCM) in Zambia.The CCM is responsible for developing national priorities and for overseeing the development and implementation of proposals.There is no representation of women's organizations in Zambia's CCM.
IX. Conclusion
Before ARVs became freely available to all in Zambia, receiving an HIV-positive diagnosis was the equivalent of a death sentence.By introducing a policy of universal access to free ART, the Zambian government proved its seriousness in attempting to combat the HIV pandemic and save the lives of many Zambians living with HIV/AIDS, including women.But there are still life-threatening barriers to the success of ART programs and some of these, such as domestic violence and insecure property rights, affect women disproportionately.The government of Zambia should urgently address and remove these barriers.
Zambian women living with HIV/AIDS suffer persistent constraints to accessing HIV information, testing, and treatment, and to adhering to ART.The accounts of women interviewed for this report reveal the excruciating effects of gender-based violence and insecure property rights, not only as abuses in their own right, but as major factors that delay women's access to lifesaving ART, compel them to hide their HIV status and medicine, and eventually impede adherence to ART.The consequences are potentially disastrous since adherence to ART must be close to perfect (95 percent) to achieve proper suppression of HIV.Lack of adherence can also lead to the emergence of new, resistant strains of HIV that can both be transmitted to others and lead to drug failure.
Zambia's health system and legal frameworks are ill-equipped to respond to gender-based abuses and their effects.In healthcare facilities HIV treatment adherence counselors and other healthcare providers do not generally probe for, discuss, or respond to gender-based violence and other abuses, thus missing vital opportunities to support women's treatment.HIV treatment counselors also do not receive specialized training to help them detect or respond to gender-based violence.There is no government protocol that instructs counselors on the practical steps to detect or address gender-based violence.Although Zambia has expanded its clinics substantially to accommodate the increasing need for and supply of ART, in most clinics there is inadequate private, confidential space for counseling.Most of healthcare facilities also lack appropriate settings for women to be able to disclose their experiences of violence or other abuses.
With respect to legal protections, there is currently no specific law to address gender-based violence, and the Penal Code has limited application in cases of domestic violence.It also does not appear to cover psychological abuse or marital rape.
Widowed and divorced women who are living with HIV/AIDS suffer impoverishment as a result of their inability to exercise and enforce their property rights, and this affects their ability to access and adhere to ART.The Intestate Succession Act is not properly enforced, and property grabbing still occurs.Widows who experience property grabbing and many women divorced under discriminatory customary law often sink into deep poverty and fail to start or adhere to treatment as a result of their inability to afford food or the transportation necessary to attend clinic appointments to collect their ART.
Zambia still has a long way to go to fulfill its international and regional obligations in relation to women's human rights, including the right to the highest attainable standard of health.As a priority the Zambian government should immediately take the necessary steps to integrate detecting and responding to gender-based violence into the work of healthcare facilities providing ART.As a prerequisite the government should build the capacity of healthcare facilities and providers so they can respond to the gender-based abuses described in this report, particularly violence against women.There are several useful guidelines developed by international and regional organizations that could help the healthcare sector in its response to gender-based violence.
The Zambian government should act immediately to introduce constitutional and legal reform as a critical measure to eliminate discrimination against women, including under customary law.The government should make sure that the new constitution affirms equal rights for all Zambians, including women.It should enact a law that addresses gender-based violence without delay, and as a necessary step towards the prevention of gender-based violence and effective prosecution of perpetrators.The Zambian government should also enforce the Intestate Succession Act.It should further ensure that the Matrimonial Causes Act provides for equal property rights for women upon divorce.
In the long run it is essential that the Zambian government, UN agencies, and donors work in collaboration with women's rights organizations to transform the unequal power relations between women and men, and the social, economic, political, and cultural factors that maintain gender-based abuses and inequality in Zambia.
In 2000 the Zambian government, along with other world leaders, made firm commitments, in the Millennium Development Goals, to promote gender equality and combat HIV/AIDS.This political commitment and the availability of resources-inadequate as they may be-could help Zambia set an example in the Southern Africa region by removing the overwhelming barriers to HIV treatment and support that some women face.Otherwise, gender-based abuses will continue to shatter the lives of countless Zambian women in acute need of ART and contribute to avoidable losses of health and lives.
X. Detailed Recommendations
To the Government of Zambia and the Zambia National Assembly
To the President of the Republic of Zambia
- Publicly denounce gender-based abuses, including gender-based violence and lack of enjoyment of property tights, and emphasize the harmful effect of these abuses on HIV treatment.
To the Zambia National Assembly
- Ensure that as the draft constitution is finalized, provisions on equality before the law regardless of sex, and provisions prohibiting any law, culture, custom, or tradition that undermine the dignity, welfare, interest or status of women or men are retained in the final version.
- Adopt specific legislation to prevent and remedy sexual and domestic violence.This should include civil and criminal judicial remedies, and the provision of services to survivors.
- Fully incorporate the Protocol to the African Charter on Human and Peoples' Rights on the Rights of Women in Africa and the Convention on the Elimination of All Forms of Discrimination against Women into domestic law and amend all discriminatory provisions in the law accordingly.
Tothe Ministry of Justice and the Gender in Development Division
- Accelerate efforts to review and transform discriminatory aspects of customary law.
To the Cabinet Committee on AIDS, the National AIDS Council, the Ministry of Health, and the Gender in Development Division
Facilitate the establishment and implementation of programs in the healthcare system to address gender-based abuses, as follows:
Establish a multi-sectoral taskforce that would identify approaches to addressing gender-based abuses in health settings that are appropriate for Zambia.
Integrate initiatives addressing gender-based abuses, especially gender-based violence, into ART and HIV programs.
The Ministry of Health and the Center for Infectious Disease Research in Zambia should continue their current efforts to expand clinics and clinic infrastructure to enable private discussions in adherence sessions before systematic screening for gender-based violence is introduced.
Ensure that HIV treatment adherence counselors integrate screening for and handling of gender-based violence in counseling, establish protocols on detecting and addressing gender-based violence, and provide continuous supervision and support for counselors to assist them in doing so.
Develop campaigns to fight prevalent myths through which HIV is seen as a disease of the "immoral" and "unfaithful."
To the Ministry of Health and the Zambia Counseling Council
- Ensure that institutions providing training for HIV counselors cover the issues of gender-based violence, women's lack of enjoyment of property rights, and other gender-based abuses and their effect on treatment in training courses.
To the Ministry of Health
- Monitor and document the impact of gender-based abuses on ART in on-going research on ART in Zambia, and include gender-based abuses as indicators in existing monitoring databases, including the Continuity of Care Patient Tracking System and database developed by the Center for Infectious Disease Research in Zambia.
- Once the appropriate systems for detecting and addressing gender-based violence are in place, CIDRZ and the Ministry of Health should revise the adherence form used in ART centers to include questions on gender-based abuses.
- Introduce appointment systems into clinics where such systems are not already in place, to reduce waiting time for HIV and ART patients.
- In collaboration with Zambian women's organizations currently conducting research on gender-based abuses and HIV/AIDS, conduct or support research on the impact of gender-based abuses on women's HIV treatment in rural areas of Zambia.
To the Gender in Development Division
- Develop a campaign that emphasizes women's right to decide when, where, and how to seek health services, including access to HIV testing and treatment programs.
- Continue efforts to sensitize Zambian communities on the harmful impacts and illegality of gender-based abuses, particularly property grabbing and gender-based violence.
To the Ministry of Home Affairs
- Ensure the provision of adequate resources and training for the Victim Support Unit (VSU) including vehicles, sexual crime kits, stationery, and appropriate training and supervision for all VSU officers.
To the Ministry of Justice, Ministry of Home Affairs, and the Zambian Police
- Ensure that more officers in the Victim Support Unit, investigators, prosecutors, legal aid providers, judges, and other court staff are trained in appropriate methods for handling cases of domestic and sexual abuse, including techniques for interviewing survivors, maintaining their privacy, referring them to health services and women's organizations, and providing protection for survivors and witnesses.
To the Ministry of Home Affairs, the Zambian Police, and the Central Statistics Office
- In collaboration with women's organizations, compile reliable and comprehensive national statistics on gender-based violence, including violence by intimate partners.Statistics should include, among other information, data on the frequency of violence, rates of prosecution, and types of punishment.
- Undertake further research that evaluates the effectiveness of interventions such as the VSU.
To The Ministry of Community Development and Social Services
- Establish shelters and other relevant services for survivors of gender-based violence in all provinces, and provide additional funding for existing YWCA shelters.
- Establish social housing units for women survivors of violence and other abuses.
To the Ministry of Justice, Ministry of Home Affairs, Ministry of Health, and the Gender in Development Division
- In collaboration with civil society organizations, establish more centers for coordinated response to sexual and gender-based violence in Lusaka, and launch similar projects in the other eight provinces.
To Donors
To the Office of the US Global AIDS Coordinator
- Provide clearer information to the public on the amount of funds allocated to combating gender-based violence and women's lack of enjoyment of property rights in Zambia.
- Increase funding of programs that address gender-based violence in health facilities in Zambia, in line with USAID's guidelines entitled Addressing Gender-based Violence through USAID's Health Programs.
- Fund civil society advocacy towards the enactment and implementation of a law on gender-based violence, improving the implementation of the Intestate Succession Act, and the law on division of property upon divorce.
- Urge the Zambian government to eliminate constitutional provisions that sanction discrimination against women, including in the areas of divorce and inheritance under customary and personal laws.
- Collaborate with and support women's organizations in Zambia in addressing gender-based abuses as they affect women's risk of HIV and access to treatment.
To the Joint United Nations Program on HIV/AIDS, the Global Fund, and the Global Fund's Zambia Country Coordinating Mechanism (CCM)
- The Global Fund should include a representative of women's organizations on the Global Fund's Zambia CCM.
- Develop training materials for CCMs on ways in which women's inequality undermines efforts to fight AIDS and on proven methods of integrating protection of women's rights in HIV/AIDS programs, including in future proposals to the Global Fund.
- Design monitoring and evaluation components that detect abuses of women's rights as part of the evaluation of AIDS programs.
To the World Bank
- Urge the Zambian government to use the funds available to the health sector through debt relief for upgrading health facilities and training healthcare providers to enable them to detect and address gender-based abuses.
- Urge the Zambian government to implement poverty eradication programs incorporated in the Fifth National Development Plan in a way that would adequately target poverty among women in Zambia.
To UN Agencies and the UN Special Rapporteur on the Right to Health
- The United Nations Population Fund and United Nations Development Program in Zambia should expand their work on gender-based violence to address the role of domestic violence in hindering treatment roll-out.In particular, UNFPA should support the health system's response to gender-based violence.
- The UN Special Rapporteur on the Right to the Enjoyment of the Highest Attainable Standard of Physical and Mental Health should investigate the link between gender-based abuses and women's access to ART, particularly in Africa, and make recommendations to governments on how to address this link.
To Regional and Global Actors
To the Congress of the United States
- Enact the Protection Against Transmission of HIV for Women and Youth Act of 2007 (the PATHWAY Act of 2007) into law to remove the abstinence-until-marriage earmark for PEPFAR programs and ensure that HIV prevention programs are based on scientific evidence, good public health practice, and human rights principles.
- Pass the African Health Capacity Investment Act of 2007, and ensure that Congress appropriates sufficient resources to build the capacity of the health workforce in Africa.
To The Office of the US Global Aids Coordinator
- Produce a report on women's inheritance rights and what PEPFAR is doing to promote them, as is called for under the law that established PEPFAR.
To the Southern Africa Development Community
- The heads of state of the SADC should adopt the Draft SADC Protocol on Gender and Development without delay.
XI. Acknowledgements
This report was researched and written by Nada Mustafa Ali, researcher in the Women's Rights Division at Human Rights Watch.Liesl Gerntholtz, consultant, conducted some of the research and contributed to the writing of the background section.
The report was reviewed by Janet Walsh, acting director of the Women's Rights Division; Cynthia Brown, member of the Advisory Committee of the Women's Rights Division; Joseph Amon, director of the HIV/AIDS and Human Rights Program; Helen Epstein, editor at the Africa Division; Aisling Reidy, senior legal advisor; and Iain Levine, program director.Portions of the report were reviewed by Elizabeth Serlemitsos, chief advisor, National Aids Council of Zambia, Dr. Iris Mwanza, deputy director, Center for Infectious Disease Research in Zambia, and Katembu Kaumba, executive director of Young Women's Christian Association in Zambia.Human Rights Watch takes full responsibility for the views expressed in this report.
Rachel Jacobson, Emily Allen, Andrea Holley, Jose Martinez, Fitzroy Hepkins, and Grace Choi provided production assistance. Anna Gressel and Andrea L. Gittleman provided research assistance.
We wish to express our sincere thanks to all the courageous women who shared their rich experiences with us.We also wish to thank all Zambian associations, government officials, and healthcare providers, as well as representatives of multilateral and bilateral agencies in Lusaka who agreed to be interviewed for this report, and Zambia desk officers at the US State Department, USAID, and OGAC in Washington, D.C. We thank Young Women's Christian Association in Lusaka, Ndola, and Kitwe, Women and Law in Southern Africa, Southern Africa HIV/AIDS Information Dissemination Service, the Nongovernmental Organizations' Coordinating Council, Council of Churches in Zambia, the Program for Urban Self-Help, International HIV/AIDS Alliance in Ndola and Kitwe, Zambia National AIDS Network, Center for Coordinated Response to Sexual and Gender-based Violence, Central Statistics Office, Family Health Trust, Women in Law and Development in Africa, the Center for Infectious Disease Research in Zambia and The Lusaka and Chongwe offices of the Health Communication Partnership in Zambia.We also wish to thank the support groups that facilitated our research.
Finally, we acknowledge valuable financial support from Arcadia, the Gruber Family Foundation, the Moriah Fund, the Oak Foundation, the Streisand Foundation, the Banky-LaRocque Foundation, the Schooner Foundation, the Jacob and Hilda Blaustein Foundation, the Frog Crossing Foundation, the Chicago Foundation for Women, and the members of the Advisory Committee of the Women's Rights Division.
Appendix I.
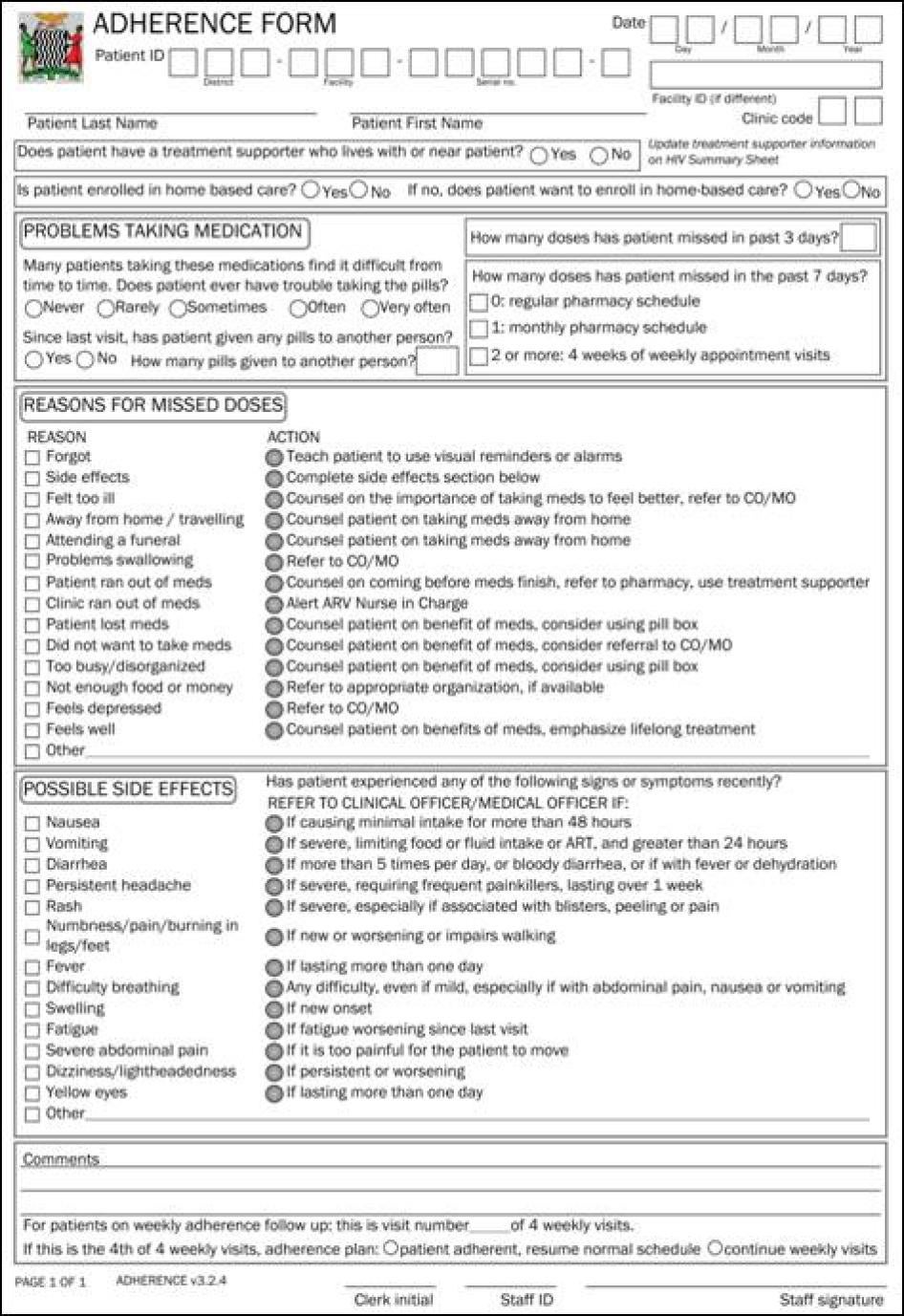
Reproduced with permission from the Center for Infectious Disease Research in Zambia
Appendix II.
Integrating Gender-Based Violence Initiatives into Health Facilities:
Selected Resources
Zambia's response to the HIV epidemic, and especially the roll-out of HIV treatment programs, can benefit substantially from integrating initiatives that detect and address gender-based violence and other abuses as part of an overall strategy to address gender-based abuses.Over the last few years, a number of international and regional agencies have stressed the key role of health facilities in detecting and responding to gender-based violence, and have devised program guides on ways to establish and run such programs.These agencies include USAID, UNFPA, and the Pan American Health Organization (PAHO), among others.Literature and guidelines produced by these agencies[266] can inform planning, implementation, and monitoring of initiatives to address gender-based violence in Zambia's HIV sector.
UNFPA devised a program guide that proposes three models for screening for and addressing gender-based violence in health facilities, especially those providing reproductive and sexual health services.UNFPA's recommended interventions range from displaying information on gender-based violence in waiting rooms and rest rooms to having personnel within the facility specifically trained to screen for gender-based violence and to make appropriate referrals or give legal and other advice.The guide provides clear steps that could inform changes in the healthcare system in Zambia.
The guide seems to influence UNFPA's work in Zambia, although the agency focuses more on the health of adolescent girls in the area of HIV/AIDS, rather than adult women.In August 2004, UNFPA launched a Zambia-specific training manual on gender-based violence and HIV/AIDS for use by local organizations.The manual provides guidelines on planning, conducting, and evaluating workshops on HIV/AIDS and gender-based violence.It also provides a step-by-step explanation of gender, socialization, society's perceptions of males and females, and power relations between men and women.It then introduces gender-based violence, and addresses its nature, extent, causes, and consequences.It provides information on Zambian organizations and institutions to which service providers can refer survivors of gender-based violence, and finally addresses HIV/AIDS and its gender dimensions.[267]
Another important resource is USAID's Addressing Gender-based Violence through USAID's Health Programs. Developed to help USAID program officers integrate responses to gender-based violence into their health sector portfolio during project design, implementation, and evaluation, this guide draws upon promising approaches that address gender-based violence in health settings, and focuses on intimate partner violence and on sexual violence by any perpetrator.The guide establishes principles for programs aiming to address gender-based violence in health settings.These include ensuring survivors' safety and autonomy, devising interventions that are appropriate to local settings, employing both a public health and human rights perspective, encouraging multi-sectoral interventions, and investing in evaluation to assess the success of programs.[268]
USAID's guidelines suggest three different approaches to prevent and respond to gender-based violence:service delivery programs, community mobilization interventions, and communication for social and behavior change.According to the document, community mobilization programs can prevent gender-based violence through changing the dominant gender norms[269] that sanction gender-based violence.This includes challenging beliefs held by healthcare providers-such as considering domestic violence a private matter-that might influence their response to gender-based violence. The document provides guidelines on what community mobilization programs should and should not do.The second approach suggested by USAID is the establishment of "communication for social and behavioral change programs" (CSBC) to raise awareness.CSBC can support initiatives that challenge the acceptability of gender-based violence at individual, community, and national levels; improve community response to gender-based violence; and increase media awareness of the link between HIV/AIDS and gender-based violence.
Most relevant to the findings of this report is USAID's third approach, which focuses on healthcare service delivery programs-particularly those working in the field of sexual and reproductive health-in addressing gender-based violence.The guide lists steps through which healthcare delivery programs can address gender-based violence, starting with institutional commitment to address gender-based violence, followed by introducing changes that fully integrate gender-based violence throughout healthcare facilities, a strategy called a "systems approach."[270] The importance of this strategy is that it recognizes the implications of deciding to tackle gender-based violence on different aspects of healthcare services, including the physical infrastructure of clinics (whether counseling rooms ensure privacy), the professional culture of the facility, patient flow, training and supervision of staff, and the existence of referral networks.[271] Using a systems approach, according to USAID, is particularly important in resource-poor settings where legal systems are weak and referral systems are inadequate.
In integrating a concern with gender-based violence in the work of health facilities, USAID recommends ongoing training and sensitization of healthcare workers on gender-based violence, "routine screening" for gender-based violence only when programs have functioning protections to safeguard women's emotional and physical safety, and the participation of healthcare facilities in "broader prevention efforts, referral networks, and advocacy campaigns."[272]Finally, the guide recommends that healthcare facilities and programs seek economic sustainability before launching specialized services addressing gender-based violence, and not duplicate existing community initiatives.The guide identifies a number of interventions that are feasible in resource-poor settings.These include support groups for survivors of gender-based violence (instead of individual psychotherapy) and finding alternative informal safe havens with friends or family instead of shelters.
USAID's resource would be a useful tool in integrating gender-based violence in health facilities disseminating ART in Zambia, particularly in terms of introducing these initiatives in facilities supported by PEPFAR.Although USAID has a strong presence in the country, as of August 2007 they "have not introduced these guidelines to [USAID's] grantees although [they] are in the process of doing so."[273]
An important resource that shares best practices in terms of health sectors' responses to gender-based violence in the Americas region is the Pan American Health Organization's Violence against Women: The Health Sector Responds.[274] The resource is a step-by-step description of PAHO's interventions to address gender-based violence in Central America, including via the health sector and in clinics. PAHO's strategy, which emphasizes flexibility and respect for local experience, started with analyzing women's experiences of gender-based violence, the ways women respond to it, and the availability of community, legal, and health sector resources in ten countries in Latin America.
Steps applied by PAHO in Latin America include: the development of national policies that recognize gender-based violence as a public health issue; outlining basic principles and guidelines for caring for survivors of gender-based violence using a gender and human rights perspective; drafting protocols on appropriate care for patients affected by gender-based violence; developing training plans for personnel on the use of norms and protocols; creating support groups for survivors of gender-based violence; promoting male involvement in such programs; developing a system that is able to report on gender-based violence cases throughout the health system; and establishing or strengthening community networks so as to coordinate the response to gender-based violence.[275]
At the regional level, the Southern African AIDS Trust has devised counseling guidelines on domestic violence that are specific to Southern Africa.[276]Informed by experiences of professional HIV counselors, people living with HIV/AIDS, and members of HIV/AIDS organizations, the guidelines target both male and female patients seeking counseling, and address myths and misconceptions associated with gender-based violence, the link between domestic violence and the transmission of HIV/AIDS, the need for effective counseling, the signs and symptoms of domestic violence, and how to identify them.One of the important points that this resource covers is how fear of domestic violence can affect women's ability to disclose HIV status or other sexually transmitted infections.It cautions counselors that many women who have followed the advice of healthcare staff and discussed their HIV status with their husbands have suffered greatly.[277]It also provides guidelines on counseling women living with HIV/AIDS who are survivors of violence and on support to counselors.The guidelines mainly target volunteer counselors, non-professional counselors, and professional counselors who do not have extensive experience in counseling people living with HIV/AIDS.It does not discuss the impact of gender-based abuses on HIV treatment.
These resources are useful tools in reforming the healthcare system and equipping it to respond to the two epidemics of HIV/AIDS and gender-based violence in Zambia.
[1] Joint United Nations Programme on AIDS (UNAIDS), AIDS Epidemic Update: December 2007 (Geneva: UNAIDS, December 2007), http://data.unaids.org/pub/EPISlides/2007/2007_epiupdate_en.pdf, (accessed November 20, 2007), p.1.
[2] Ibid., p. 15.
[3] World Health Organization (WHO), UNAIDS, and United Nations Children's Fund (UNICEF), Towards Universal Access: Scaling Up Priority HIV/AIDS Interventions in the Health Sector: Progress Report (Geneva: WHO, April 2007), p. 19; UNAIDS, AIDS Epidemic Update, p. 15.
[4]See for example Julia Kim and Charlotte Watts, "Gaining A Foothold: Tackling Poverty, Gender Inequality and HIV in Africa," British Medical Journal , no. 331, October 1, 2005, pp. 769-772; K. L. Dunkle et al., "Gender-Based Violence, Relationships, Power, and the Risk of HIV Infection in Women Attending Antenatal Clinics in South Africa," The Lancet , vol. 363 (2005), pp. 14151421.
[5]Helen Epstein, The Invisible Cure: Africa, the West, and the Fight Against AIDS(New York: Farrar, Straus and Giroux, 2007) p. 179.
[6] Alpha O. Konare, "Foreword," in WHO Regional Office for Africa, The African Regional Health Report: The Health of the People (Geneva: WHO, 2006), http://www.afro.who.int/regionaldirector/african_regional_health_report2006.pdf (accessed October 1, 2007), p. xi.
[7] WHO and UNAIDS, Progress on Global Access to HIV Antiretroviral Therapy:A Report on "3 by 5" and Beyond (Geneva: WHO, 2006), http://www.who.int/hiv/progreport2006_en.pdf (accessed May 14, 2007), pp. 71-75.
[8] WHO, UNAIDS and UNICEF, Towards Universal Access: Scaling Up Priority HIV/AIDS Interventions in the Health Sector, p. 15.
[9]WHO, Towards Universal Access by 2010: How WHO is Working With Countries to Scale-Up HIV Prevention, Treatment, Care and Support (Geneva: WHO, 2006), p. 5.
[10]WHO and UNAIDS, Progress on Global Access to HIV Antiretroviral Therapy, p. 19.By the end of 2006 1.3 million people in sub-Saharan Africa were on ART, compared to 100,000 in 2003.Sub-Saharan Africa is home to 67 percent of all those on treatment in low-and middle-income countries, up from 42 percent in 2003.WHO and UNAIDS, Progress on Global Access to HIV Antiretroviral Therapy, p. 14.
[11]WHO and UNAIDS, Progress on Global Access to HIV Antiretroviral Therapy, p. 9.
[12]WHO, Antiretroviral Therapy for HIV Infection in Adults and Adolescents, p. 70.
[13] Ibid.
[14] WHO, Adherence to Long-Term Therapies: Evidence for Action (Geneva: WHO, 2003), http://www.who.int/chp/knowledge/publications/adherence_full_report.pdf (accessed October 1, 2007), p. 96.
[15] UNAIDS, "Zambia," Country Profile, http://www.unaids.org/en/Regions_Countries/Countries/zambia.asp (accessed October 9, 2007).
[16] UNAIDS in Zambia, Joint United Nations Programme of Support on AIDS (2007-2010) (Lusaka: UNAIDS, 2006).
[17] Ministry of Finance and National Planning, Fifth National Development Plan (2006-2010)(Lusaka: Ministry of Finance and National Planning, 2006), p. 296.
[18] Ibid.
[19] In 1999 only 21 HIV testing sites were available in Zambia.By the end of 2005 HIV testing facilities were available in 226 centers around the country.By January 2006 the number of testing sites increased to 485 country-wide.Ministry of Health, Zambia National Guidelines for HIV Counseling and Testing (Lusaka: Ministry of Health, 2006), p. 1.
[20] Republic of Zambia Central Statistics Office (CSO), Ministry of Health, and MEASURE Evaluation, "Zambia Sexual Behavior Survey (2005)," March 2006, table A.1.6., p.111.The survey is country-wide and was designed to produce sex disaggregated estimates in rural and urban areas of Zambia.A total number of 2,330 households were covered, where interviews were completed with 2,174 women and 2,046 men in the age range of 15-49 years old.
[21] Ibid., p. 12.
[22]WHO, "Zambia: Summary Country Profile for HIV/AIDS Treatment Scale Up," 2005, http://www.who.int/hiv/HIVCP_ZMB.pdf (accessed October 5, 2007), p. 2.
[23]It appears from our interviews that prior to commencing ARV treatment patients are required to undergo a CD4 count, a full blood count, a chest X-ray, and a liver function test.
[24] WHO, "Zambia: Summary Country Profile," p.2.
[25]WHO, UNAIDS, and UNICEF, "Epidemiological Fact Sheets on HIV/AIDS and Sexually Transmitted Infections - Zambia," http://www.who.int/globalatlas/predefinedReports/EFS2006/EFS_PDFs/EFS2006_ZM.pdf (accessed October 4, 2007), p.12.
[26] PEPFAR "Zambia: 2007 Country Profile," http://www.pepfar.gov/press/81694.htm (accessed December 9, 2007).
[27]WHO, UNAIDS and UNICEF, "Towards Universal Access: Scaling Up Priority HIV/AIDS Interventions in the Health Sector, Progress Report," April 2007, p. 19.
[28]WHO, UNAIDS, and UNICEF, "Epidemiological Fact Sheets on HIV/AIDS and Sexually Transmitted Infections," p.5.
[29] Ministry of Finance and National Planning, Fifth National Development Plan, pp. 160-161.
[30] The United States President's Emergency Plan for AIDS Relief (PEPFAR), "2007 Country Report: Zambia," http://www.pepfar.gov/documents/organization/81673.pdf (accessed September 29, 2007).
[31] Ministry of Health, "Scale-Up Plan for HIV Care and Antiretroviral Therapy Services (2006-2008)," 2006, p. 11.
[32] Ibid.
[33] WHO, "World Health Statistics 2007", 2007, http://www.who.int/whosis/whostat2007_5healthsystems_hrh.pdf (accessed October 10, 2007), p. 62.
[34]Human Rights Watch interview with Dr James Banda, Director, DHMT, Kitwe, February 21, 2007.
[35] Ibid.
[36] Mary Kazunga and Patrick Mumba Chewe, "Violence Against Women" in Central Statistical Office-Zambia, Zambia Demographic and Health Survey 2001 -2002 (Lusaka: Central Statistics Office, 2003), p. 187.The sample for the 2001-2002 survey covered the population residing in private households ages 15 to 49. The survey was country-wide and was designed to produce sex disaggregated estimates in rural and urban areas of Zambia.The number of female respondents to the survey was 7,658 and the number of male respondents was 2,145.
[37] Young Women's Christian Association, 2006 Statistics, on file with Human Rights Watch.Also see "Zambia: More than 10 Girls Raped Every Week," IRIN PlusNews , November 28, 2007, http://www.worldywca.info/index.php/ywca/layout/set/print/world_ywca/ywca_news/association_news/zambia_more_than_10_girls_raped_every_week (accessed October 3, 2007).
[38] Intestate Succession Act, No. 5 of 1989.
[39] Human Rights Watch interview with Pamela Mumbi, lawyer, International Justice Initiative, Lusaka, February 21, 2007.
[40] Human Rights Watch interview with Yoram Siame, HIV/AIDS program officer at the Church Health Association of Zambia, Lusaka, February 20, 2007.
[41] The Matrimonial Causes Act 2007 (draft).Section 57(1) of the draft Matrimonial Causes Act provides for settlement of property upon the dissolution or annulment of a marriage.Christine Zulu, assistant to the Clerk, Zambia National Assembly, informed Human Rights Watch that "the Bill went through with a lot of amendments. As soon as these amendments have been effected and the Bill assented by His Excellency the President and published into an Act, it will be made available on our website" (email correspondence, August 20, 2007).
[42] The Marriage Act, Chapter 50 of the Laws of Zambia.
[43] Women and Law in Southern Africa (WLSA), The Changing Family in Zambia (Lusaka: WLSA, 1997).Informed by earlier research, WLSA's position on the traditional customary law system is that it is "more accessible to most people, mainly because it is directly relevant [to their daily lives], but also to a large extent because it requires less resources to reach it."WLSA, Justice in Zambia: Myth or Reality?p. 1.
[44] Human Rights Watch interview with Matrine Chuulu, WLSA regional coordinator, Lusaka, January 28, 2007 and Engwase Mwale, executive director of NGOCC, Lusaka, February 13, 2007.
[45]WHO, UNAIDS and UNICEF, "Epidemiological Fact Sheets on HIV/AIDS and Sexually Transmitted Infections," p .5.
[46]Republic of Zambia Gender and Development Division, "Zambia's Country Report on the Implementation of the Southern African Declaration on Gender and Development and its Addendum on the Prevention of Violence Against Women and Children," August 2006, p. 33.
[47]Zambia Association for Research and Development and Southern African Research and DocumentationCenter, Beyond Inequalities 2005: Women in Zambia (Lusaka and Harare: ZARD and SARDC, 2005), p. 20.
[48]Gender in Development Division (GIDD), "Zambia's Country Report on the Implementation of the Southern African Declaration on Gender and Development," pp. 15-21.In 1997 the SADC Heads of State committed to "Ensuring the equal representation of women and men in the decision making of Member States and SADC structures at all levels, and the achievement of at least thirty percent target of women in political and decision making structures by 2005."Declaration on Gender and Development, Southern African Development Community, 1997, http://www.sadc.int/key_documents/declarations/gender.php, article H.
[49] Electoral Institute of Southern Africa, "Zambia: 2006 National Assembly Elections Gender Breakdown," October 2006, http://www.eisa.org.za/WEP/zam2006resultsg.htm (accessed October 1, 2007).
[50] Ibid., p. 15.
[51] The 2001-2002 ZDHS preliminary report (CSO 2002) indicates that husbands often make the final decision in areas of a wife's healthcare (58 percent), and large household purchases (63 percent).World Bank, "Zambia Strategic Country Gender Assessment," June 2004, http://siteresources.worldbank.org/EXTAFRREGTOPGENDER/Resources/ZambiaSCGA.pdf (accessed September 20, 2007), p.43.
[52] Ibid., p.43.
[53]ZARD and SARDC, Beyond Inequalities 2005, p. 12.
[54]Human Rights Watch interview with Lumba Siyanga, information and advocacy manager, Women for Change, Lusaka, May 25, 2006.
[55]Human Rights Watch interview with Isabel H., Lusaka, February 3, 2007
[56]CSO - Zambia, "Zambia Demographic and Health Survey 2001 -2002," p. 46.Reasons for wife beating covered in the survey included infidelity, arguing with a husband, neglecting the children, refusing to have sex with a husband, and cooking bad or late food.
[57]Human Rights Watch interview with Sinya Mbale, head of programs, Agricultural Recovery, Lusaka, May 25, 2006.
[58] Human Rights Watch interview with Mercy Z., Lusaka, February 21, 2007.
[59] Human Rights Watch interview with Unique Z., Lusaka, February 20, 2007.
[60] CD4 count is the measure of the number of helper T cells (cells in the immune system) per cubic millimeter of blood, used to analyze the prognosis of patients infected with HIV.
[61] Human Rights Watch interview with Unique Z., Lusaka, February 20, 2007.
[62] Human Rights Watch interview with Monica Mwachande, nurse-sister, Kalingalinga Clinic, Lusaka, February 8, 2007.
[63] Human Rights Watch interview with Precious C., Lusaka, February 8, 2007.
[64] Ibid.
[65] WiLDAF, "Elimination of Discrimination Against Women in Zambia," undated, p.10.
[66] Human Rights Watch interview with Ruth M., Chongwe, February 9, 2007.
[67] In the case of Zambia recent research in five districts including Lusaka, Kitwe, and Ndola found that many women receiving ART experienced daunting barriers to adherence, including fear of disclosure, gender-based violence, and having to share ART with an untested husband.Out of 560 women who took part in the study, 66 percent did not disclose their HIV status to their intimate partners because of "fear of blame, abandonment and losing the economic support of their partner." See K.P. Zulu "Fear of HIV Serodisclosure and ART Success: the Agony of HIV-Positive Married Women in Zambia,"3rd IAS Conference on HIV Pathogenesis and Treatment 2005, Rio de Janeiro, Brazil, 2427 July 2005. (Abstract no. TuPe11.9CO3); http://www.iasociety.org/Abstracts/A2176464.aspx (accessed October 10, 2007).
[68] P.Gaillard et al., "Consequences of Announcing HIV Seropositivity to Women in an African Setting: Lessons for the Implementation of HIV Testing and Interventions to Reduce Mother-to-Child HIV Transmission," abstract no. TuPpB1157, International AIDS Conference, South Africa, July 9-14, 2000.In this study researchers interviewed 331 HIV-positive women participating in a study on the prevention of mother-to-child transmission of HIV in Mombasa, Kenya, two months after they received their HIV test results.Thirty-two percent of those in stable relationships had informed their partners of their test results after receiving counseling.Seventy-three percent of those who informed their partners said that the latter were understanding.See also P. Keogh et al. "The Social Impact of HIV Infection on Women in Kigali, Rwanda: A Prospective Study," Social Science and Medicine, 38(8), 1994, pp. 1047-53; O.A. Grinstead et al., "Positive and Negative Life Events after Counseling and Testing: the Voluntary HIV-1 Counseling and Testing Efficacy Study," Aids , 15(8),2001, pp. 1045-52; S. Issiaka et al., "Living With HIV: Women's Experience in Burkina Faso, West Africa," AIDS Care, 13(1), 2001, pp. 123-8; W.L. Heyward et al., "Impact of HIV Counseling and Testing among Child-Bearing Women in Kinshasa, Zaire", Aids7(12), 1993, pp. 1633-7; Suzanne Maman et al., "High Rates and Positive Outcomes of HIV Serodisclosure to Sexual Partners: Reasons for Cautious Optimism from a Voluntary Counseling and Testing Clinic in Dar es Salaam, Tanzania," AIDS and Behavior, 7(4), 2003, pp. 373-382.
[69] Suzanne Maman, "To Disclose or Not to Disclose: An Overview of Women's HIV Serostatus Disclosure Experiences Globally," in USAID/Synergy, Women's Experiences with HIV Serodisclosure in Africa: Implications for VCT and MTCT, Meeting Report (Washington, DC: USAID, March 2004), p. 3.
[70] Human Rights Watch interview with Berta K., Lusaka, February 3, 2007.
[71] Human Rights Watch interview with Beatrice S., Lusaka, February 3, 2007.
[72] Human Rights Watch interview with Berta K., Lusaka, February 3, 2007.
[73] Human Rights Watch interview with Marrietta M., Ndola, February 20, 2007.
[74] Ibid.
[75] Human Rights Watch interview with Berta K., Lusaka, February 3, 2007.
[76] Human Rights Watch interview with Charity T., Lusaka, February 3, 2007.
[77] Human Rights Watch interview with Maria T., Lusaka, February 3, 2007.
[78] Human Rights Watch interview with Charity T., Lusaka, February 3, 2007.
[79] Human Rights Watch Interview with Ida Mukuka, AIDS activist and former support groups coordinator, Lusaka, January 31, 2007.
[80] Human Rights Watch interview with Eric Nachibanga, member of the Network of Zambian People Living with HIV/AIDS (NZP+) and counselor at the University of Zambia HIV Clinic, January 31, 2007.
[81] Human Rights Watch interview with Yeta Mekazu, YWCA's shelter manager, Lusaka, February 1, 2007 (group interview with the director, programs manager, and shelter manager of YWCA).
[82]Human Rights Watch group meeting with ten women living with HIV/AIDS, Lusaka, February 3, 2007.One woman who uses the services of the Matero main clinic in Lusaka told Human Rights Watch that counselors at the clinic asked about domestic violence, talked to her late husband, and advised her to use YWCA services, which lead to a decrease in the violence but not an end to it.Human Rights Watch interview, Lusaka, February 3, 2007.
[83] Human Rights Watch interview with Lucia G., Lusaka, February 10, 2007.
[84] Ibid.
[85] Human Rights Watch interview with Angela R., Lusaka, February 10, 2007.
[86] WLSA, The Changing Family in Zambia, pp.172-180.According to WLSA, "a number of advantages of contracting marriage under Statutory law have been cited a woman married under statutory law can (at least on paper) claim a share of matrimonial property whereas, under customary law, whether the woman gets a share or not depends on the customary law applicable.Divorce cases observed in Local Courts (which apply customary law) showed that, in most cases going before Local Courts, the court justices [made] no mention [to] what was to happen to the matrimonial property." See WLSA, The Changing Family in Zambia, p. 164.WLSA contends that in reality, a woman married under statutory law in Zambia "is in the same precarious position as one married under customary law." Ibid.On December 9, 2005, however, there was an encouraging development in the divorce case of Martha Kembo Mwanamwalye and Collins Mwanamwalye, where the magistrate ruled that "notwithstanding that the parties in this matter were married under customary law, justice demands that when a marriage has broken down, the parties should be put on equal position to avoid any one of them falling into destitution.""Landmark Judgment for Women in Customary Marriages." IRIN News, December 21, 2005, http://www.irinnews.org/report.aspx?reportid=57641 (accessed December 26, 2006).
[87] Pathfinder International, "Technical Series Number 5: The Essentials of Antiretroviral Therapy for Health Care and Program Managers," April 2007, http://www.pathfind.org/site/DocServer/ART_TGS1.pdf?docID=8481 (accessed May 1, 2007), p. 13.
[88] Human Rights Watch interview with Caroline M., Mandevu, Lusaka, February 10, 2007.
[89] Human Rights Watch interview with Ann K., Kafue, February 7, 2007.
[90] Human Rights Watch interview with Mina P., Ndola, February 20, 2007.
[91] Human Rights Watch interview with Hilda M., Ndola, February 20, 2007.
[92] Human Rights Watch interview with June S., Lusaka, January 31, 2007.
[93] Ibid.
[94] Ibid.
[95] Human Rights Watch interview with Beatrice S., Lusaka, February 3, 2007.
[96] Research by Physicians for Human Rights documented similar experiences of food insufficiency among people accessing ART, particularly women in Botswana and Swaziland. Physicians for Human Rights, Epidemic of Inequality: Women's Rights and HIV/AIDS in Botswana and Swaziland (Cambridge, Massachusetts:PHR, 2007).
[97] Central Statistics Office (CSO), Zambia 2000 Census of Population and Housing (Lusaka: CSO, 2003), p.xxi.
[98] Ministry of Finance and National Planning, Fifth National Development Plan, p. 313.
[99] UNAIDS, "Nutrition and Food Security," http://www.unaids.org/en/Policies/Nutrition/default.asp (accessed on 3 December, 2007).
[100] Pathfinder International, "Technical Series Number 5: The Essentials of Antiretroviral Therapy," p. 13.
[101]Human Rights Watch interview with Dorothy M., Kitwe, February 21, 2007
[102]Human Rights Watch interview with Sarah D., Ndola, February 20, 2007
[103] Human Rights Watch Interview with Dr. Bushimpa Tambatamba, director of Lusaka District Health Management Team, Lusaka, February 13, 2007, and Human Rights Watch phone interview with Dr. Bushimpa Tambatamba, August 1, 2007.
[104] National HIV/AIDS/STI/TB Council, "National HIV and AIDS Strategic Framework (2006-2010)," 2006, p. 3.
[105] Ministry of Finance and National Planning, Fifth National Development Plan, p. 314.
[106] Ibid., p. 316.
[107] In 1996 the World Health Assembly declared violence against women a major public health issue that needed to be tackled by governments and health institutions and organizations.Resolution WHA49.25, of the 49th World Health Assembly, Geneva, 1996.
[108] WHO and UNAIDS, "Ensuring Equitable Access to Antiretroviral Treatment for Women: WHO/UNAIDS Policy Statement," 2004, p. 1.
[109] Ibid., p. 2.
[110] According to the resolution, the UN Commission on Human Rights "Emphasizes that violence against women and girls has an impact on their physical and mental health, including their reproductive and sexual health, and, in this regard, encourages States to ensure the availability towomen and girls of comprehensive and accessible health-care services and programs and to health‑care providers who are knowledgeable and trained to recognize signs of violence against women and girls and to meet the needs of patients who have been subjected to violence, in order to minimize the adverse physical and psychological consequences of violence."Office of the High Commissioner for Human Rights, "Elimination of Violence Against Women," Resolution 2005/41, E/CN.4/2005/41, http://ap.ohchr.org/documents/E/CHR/resolutions/E-CN_4-RES-2005-41.doc (accessed September 14, 2007), para. 7.
[111] UN Committeeon the Elimination of Discrimination against Women, General Recommendation 24, Article 12: Women and Health,(Twentieth session, 1999), Compilation of General Comments and General Recommendations Adopted by Human Rights Treaty Bodies, UN Doc. HRI\GEN\1\Rev. 7, (2008), p. 278.
[112] Jeffery S. A. Stringer et al., "Rapid Scale-Up of Antiretroviral Therapy at Primary Care Sites in Zambia:Feasibility and Early Outcomes," Journal of the American Medical Association, 296(7), August 16, 2006, pp. 783-4.
[113] Human Rights Watch Interview with Dr. Bushimpa Tambatamba, Lusaka, February 13, 2007 and Human Rights Watch phone interview with Dr. Bushimpa Tambatamba, August 1, 2007.
[114] Human Rights Watch interviews with over 25 counselors in Lusaka and the Copperbelt provinces, January and February 2007.
[115] Group interview with the director, programs manager, and shelter manager of the YWCA, Lusaka, February 1, 2007, Human Rights Watch Interview with Dr. Bushimpa Tambatamba, Lusaka, February 13, 2007 and Human Rights Watch phone interview with Dr. Bushimpa Tambatamba, August 1, 2007.
[116] Human Rights Watch interviews with over 25 counselors in Lusaka and the Copperbelt provinces, January and February 2007.
[117] Human Rights Watch interview with Yeta Mekazu, Lusaka, February 1, 2007.
[118] The Centre for Infectious Disease Research in Zambia (CIDRZ) is a nongovernmental organization established in 1999 with support from the University of Alabama at Birmingham, USA.One of the PEPFAR partners in Zambia, it provides support to the Zambian Government in its HIV prevention and treatment programs.
[119] CIDRZ uses the Continuity of Care Patient Tracking System (SmartCare), which is a software system that processes data collected via the adherence monitoring form and other clinical forms.Developed in collaboration with the US Centers for Disease Control and Prevention and the Zambian Ministry of Health, this system is used in health facilities to track patient visits (and missed visits) and to collect indicators for each patient.The Zambian government uses SmartCare, a national health management and monitoring system.Human Rights Watch interview with Dr. Iris Mwanza, Lusaka, February 5, 2007 and Human Rights Watch interview with Samba F. Muvuma, Chongwe District TB and HIV/AIDS Coordinator, Chongwe, February 9, 2007.
[120] A. Guedes, "Addressing Gender-Based Violence from the Reproductive Health/HIV Sector: A Literature Review and Analysis," USAID Bureau for Global Health, May 2004, http://www.prb.org/pdf04/AddressGendrBasedViolence.pdf, p.32, (accessed July 20, 2007).
[121] For a full discussion of why health facilities should address gender-based violence, see S. Bott et al., Improving the Health Sector Response to Gender-based Violence: A Resource Manual for Health Care Professionals in Developing Countries. (New York: IPPF/Western Hemisphere Region, 2004) and A. Guedes, "Addressing Gender-based Violence from the Reproductive/HIV Sector."
[122] Human Rights Watch phone interview with Dr. Kamoto Mbewe, reproductive health specialist at the Ministry of Health, September 28, 2007.
[123] Human Rights Watch interview with Elizabeth Serlemitsos, chief advisor, NAC, February 1, 2007.
[124] Human Rights Watch interview with Mustawe Dennis, manager of planning and development, Kafue District Health Management Team, Kafue, February 7, 2007.
[125] Human Rights Watch interview with Theresa Chidothi, nurse and counselor, Kafue, February 7, 2007.
[126] Ibid.
[127] Human Rights Watch interview with Idah Mthetwa, ART nurse and adherence counselor, Chongwe, February 9, 2007.
[128] Human Rights Watch interview with Idah Mwandwe, ART in charge, counselor, nurse, and midwife at Kalingalinga Clinic. Lusaka, February 8, 2007.
[129] Human Rights Watch interview with Monica Mwachande, senior nurse at Kalingalinga Clinic, Lusaka, February 8, 2007.
[130] Ibid.
[131] Human Rights Watch Interview with Dr. Bushimpa Tambatamba, Lusaka, February 13, 2007, and Human Rights Watch phone interview with Dr. Bushimpa Tambatamba, August 1, 2007, and Mustawe Dennis, Kafue, February 7, 2007.
[132] Human Rights Watch Interview with Dr. Bushimpa Tambatamba, Lusaka, February 13, 2007, and Human Rights Watch phone interview with Dr. Bushimpa Tambatamba, August 1, 2007.
[133] Human Rights Watch interview with Francis Mangani, manager, KaraCounselingTrainingCenter, Lusaka, February 5, 2007.
[134] Human Rights Watch phone interview with Chilimba S. Hamahwa, head of department of counseling studies, Chainama College of Health Sciences, Lusaka, April 26, 2007.Kara Counseling is the Regional AIDS Training Network's (RATN) member institution (focal point) in Zambia.Based in Nairobi, Kenya, the RATN develops training materials that are used by member organizations.According to the RATN training programs manager, Kara Counseling uses a counseling curriculum that wasdeveloped and reviewed jointly by RATN member organizations and experts from the region.RATN also has a Programs Committee of the Board that reviews programs quarterly.In terms of gender training, the training programs manager at RATN stated that, "Gender, ART, Stigma and Discrimination (GASD) are priorities in the RATN collaborative courses. We have developed a toolkit on GASD which the member institutions (including Kara) use to mainstream those components." Human Rights Watch email correspondence with Anastasia Ndiritu, training programs manager for RATN Secretariat, Nairobi, August 16, 2007.
[135] Ibid., and Human Rights Watch Interview with Dr. Bushimpa Tambatamba, Lusaka, February 13, 2007 and Human Rights Watch phone interview with Dr. Bushimpa Tambatamba, August 1, 2007.
[136] Human Rights Watch interview with Elizabeth Serlemitsos, Lusaka, February 1, 2007, Samba F. Muvuma, Chongwe, February 9, 2007, and Ellis Beneder, medical doctor, Kara Clinic, Lusaka, February 13, 2007.
[137] Jeffery S. A. Stringer et al., "Rapid Scale-Up of Antiretroviral Therapy at Primary Care Sites in Zambia:Feasibility and Early Outcomes," p. 791.
[138] GIDD, "Zambia's Country Report on Progress Made on the Implementation of the Southern African Declaration on Gender and Development."
[139]Jeffery S. A. Stringer et al., "Rapid Scale-Up of Antiretroviral Therapy at Primary Care Sites in Zambia:Feasibility and Early Outcomes," p. 791, Human Rights Watch interview with Dr. Bushimpa Tambatamba, Lusaka, February 13, 2007, and Human Rights Watch phone interview with Dr. Bushimpa Tambatamba, August 1, 2007.
[140] Human Rights Watch interview with Margaret Mweetwa, enrolled midwife, Kamwala Clinic, Lusaka, February 16, 2007 and with over 25 counselors.
[141] Human Rights Watch phone interview with Dr. Kamoto Mbewe, Lusaka, September 28, 2007.
[142] Human Rights Watch interview with Pamela Namakando, acting director of counseling, ARTDepartment, Kamwala Clinic, Lusaka, February 16, 2007.
[143] Human Rights Watch interview with a supervisor at a clinic in Lusaka, [name withheld], Lusaka, February 2007.
[144] Human Rights Watch interview with an HIV counselor, [namewithheld], Lusaka, February 2007.
[145] Human Rights Watch interview with Harriet F., Chongwe, February 9, 2007, and Julia N. Chongwe, February 9, 2007.
[146] Jeffery S. A. Stringer et al., "Rapid Scale-Up of Antiretroviral Therapy at Primary Care Sites in Zambia:Feasibility and Early Outcomes," p. 784.
[147] Human Rights Watch interview with Samba F. Muvuma, Chongwe District Health TB and HIV/AIDS coordinator, Chongwe, February 9, 2007.
[148] Human Rights Watch interview with Conrad Tembo, Chongwe district commissioner, Chongwe, February 9, 2007.
[149] Human Rights Watch Interview with Dr. Bushimpa Tambatamba, Lusaka, February 13, 2007, and Human Rights Watch phone interview with Dr. Bushimpa Tambatamba, August 1, 2007.
[150] CIDRZ, "CIDRZ-Supported Enrollment into National HIV Care and Treatment Program, by Site, Through October 2006," http://www.cidrz.org/hivaids/ (accessed August 13, 2007).In 2006 the Zambian government built a double-story, 1,680 square-meter HIV care and treatment center at the University Teaching Hospital, in collaboration with CIDRZ and the Centers for Disease Control and prevention, using PEPFAR resources.That year about $1.5 million was spent to expand and renovate several government health facilities, including clinics at the UTH in Lusaka, Lewinika GeneralHospital and Mulambwa clinic in Mongu.In Lusaka nine facilities providing ART were renovated by 2006, including Kamwala and Kalingalinga clinics.Seven new HIV treatment clinics were also constructed.Three clinics were also established in Kafue.CIDRZ, "Infrastructure Development,"Http://www.cidrz.org/InfrastructureDevelopment (accessed August 13, 2007).
[151] Human Rights Watch Interview with Dr. Bushimpa Tambatamba, Lusaka, February 13, 2007, and Human Rights Watch phone interview with Dr. Bushimpa Tambatamba, August 1, 2007.
[152] Human Rights Watch interview with Sheila Y., Lusaka, February 3, 2007.
[153] National HIV/AIDS/STI/TB Council, "National HIV and AIDS Strategic Framework (2006-2010)," May 2006, p. 34.
[154] Women's leadership in the response to HIV/AIDS was one of the main themes of the International Women's Summit on HIV/AIDS, which took place in Nairobi in July 2007.See for example UN Deputy Secretary-General Asha-Rose Migiro's speech to the International Women's Summit, Nairobi, July 5, 2007, Deputy Secretary-General, DSG/SM/328, WOM/1634, http://www.un.org/News/Press/docs/2007/dsgsm328.doc.htm (accessed December 3, 2007).
[155] Human Rights Watch interview with Confucius Mweene, civil society specialist, NAC, February 22, 2007.
[156] Article 23 of the Zambian Constitution reads as follows: "23 (1) Subject to clauses (4), (5) and (7), a law shall not make any provision that is discriminatory either of itself or in its effect. (2) Subject to clauses (6), (7) and (8), a person shall not be treated in a discriminatory manner by any person acting by virtue of any written law or in the performance of the functions of any public office or any public authority.(3) In this article the expression 'discriminatory' means affording different treatment to different persons attributable, wholly or mainly to their respective descriptions by race, tribe, sex, place of origin, marital status, political opinions, color or creed whereby persons of one such description are subjected to disabilities or restrictions to which persons of another such description are not accorded privileges or advantages which are not accorded to persons of another such description. (4) Clause (1) shall not apply to any law so far as that law makes provision----(c ) with respect to adoption, marriage, divorce, burial, devolution of property on or other matters of personal law;
(d) for application in the case of members of a particular race or tribe, of customary law with respect to any matter to the exclusion of any law with respect to that matter which is applicable in the case of other persons."Constitution of the Republic of Zambia, as amended by Act no. 18 of 1996, art.23.
[157] The Constitution of Zambia Bill, National Assembly of Zambia, January 12, 2006, http://www.parliament.gov.zm (accessed March 12, 2007).
[158] Zambia Penal Code, vol. 7, chap. 87 of the Laws of Zambia, revised 1995, chapter XXIV, sec. 248.
[159] Although no systematic research took place to determine the percentage of women withdrawing complaints, the director of the one-stop center stated that about 50 percent of domestic violence cases are withdrawn.
[160] Human Rights Watch interview with Nelson Mwape, director, Centre for Coordinated Response to Sexual and Gender-Based Violence, Lusaka, February 17, 2007.
[161]Zambia Penal Code, chap. XV, sec. 132.
[162] See for example World Organization Against Torture, "Human Rights Violations in Zambia: II: Women's Rights,"Shadow Report Presented to the United Nations Human Rights Committee, July 2007, http://www.ohchr.org/english/bodies/hrc/docs/ngos/omct_zambia1.pdf(accessed August 30, 2007), p. 11.
[163] Ibid.
[164] Draft Sexual Offences and Gender Violence Bill (2006), part I, art. 3(a).
[165] Ibid., part V, arts.40-60.
[166] Human Rights Watch is concerned by some provisions of the Bill that it believes should be amended before it becomes law.One such provision is for aggravated sentences for rapists who are carriers of sexually transmitted diseases as this perpetuates stigma.Moreover, intentional (willful) transmission of HIV can already be addressed through existing criminal statutes.The International Guidelines on HIV/AIDS and Human Rights, in its guideline number 4, specifically advises that criminal and public health legislation "should not include specific offences against the deliberate and intentional transmission of HIV but rather should apply general criminal offences to these exceptional cases. Such application should ensure that the elements of foreseeability, intent, causality and consent are clearly and legally established to support a guilty verdict and/or harsher penalties." Office Of The United Nations High Commissioner For Human Rights, International Guidelines on HIV/AIDS and Human Rights, (2006 consolidated version) HR/PUB/06/9, B(guideline 4a).The bill also provides for mandatory HIV testing for perpetrators and victims of sexual crimes, which violates international human rights law and provides no public health benefit.
[167] Human Rights Watch interview with Engwase Mwale, executive director of Non Governmental Organizations' Coordinating Council, Lusaka, February 13, 2007.This was confirmed by the then Deputy Minister of Justice who told Human Rights Watch, "the Cabinet has previously resolved that there is a need to have specific legislation on [gender-based violence].However, I am not satisfied that all bodies have been consulted.The Director of Public Prosecutions [was not consulted].As a department, we have taken it on board We need to ensure that that the parliamentary drafting process [of the bill] is completed."Human Rights Watch interview with Bradford Machila, MP, former deputy minister of justice, Lusaka, February 5, 2007.
[168] GIDD, "Zambia's Country Report on Progress Made on the Implementation of the Southern African Declaration on Gender and Development."The amendment raised the sentence for sexual offenders to a minimum of fifteen years in jail.Civil society organizations, particularly women's groups, advocated widely for this change, which applies mainly to children and to cases of sexual harassment at work. Human Rights Watch interview with Engwase Mwale, Lusaka, February 13, 2007.
[169]Matrimonial Causes Act, Zambia National Assembly, 2007.The above analysis is based on the most recent draft of the bill.The Zambia National Assembly informed Human Rights Watch that "the [Matrimonial Causes] Bill went through with a lot of amendments. As soon as these amendments have been effected and the Bill assented by His Excellency the President and published into an Act, it will be made available on our website," Human Rights Watch email communication with Christine M. Zulu, personal assistant to the clerk, Zambia's National Assembly, August 20, 2007.One of the negative provisions in the bill is that it lists infection with a sexually transmitted disease as a ground for presenting a petition for divorce, which can contribute to fostering stigma and discrimination in Zambian communities: "A petition for divorce may be presented to the Court by either party to a marriage on the ground that:. (c ) The respondent is infected with a sexually transmitted disease which is in a communicable form, whether such disease is curable or not."
[170] Marriage Act, Chapter 50 of the Laws of Zambia.
[171] WLSA,The Changing Family in Zambia.Based on its research on the family and on the administration of justice in Zambia, WLSA takes the position that the traditional customary law system is "more accessible to most people, mainly because it is directly relevant [to their daily lives], but also to a large extent because it requires less resources to reach it."WLSA, Justice in Zambia: Myth or Reality?p. 1.
[172]GIDD, "Zambia's Country Report on Progress Made on the Implementation of the Southern African Declaration on Gender and Development."The Zambian Judiciary consists of the Supreme Court, the High Court, the Industrial relations Court, the Magistrates (Subordinate) Courts, and the Local Courts that are administered by chiefs.Women's representation in the judiciary varies between the traditional customary system on one hand, and the statutory system on the other.In the Supreme and High Courts, in 2006 there were 43 judges, out of whom 13 were women.In the Magistrate Court there are 119 magistrates out of whom 27 are women.However, out of a total number of 808 local court justices, only 90 were women in 2006.
[173] World Bank, Engendering Sustainable Growth in Zambia: A Gender Strategy for Promoting Economic Effectiveness, (Washington DC: World Bank, 1994).
[174] Intestate Succession Act of 1989, art. 5.
[175] In polygamous families, widow(s) of a deceased man share 20 percent of the property "proportional to the duration of their respective marriages to the deceased, and factors such as the widow's contribution to the deceased's property may be taken into account when justice so requires." Intestate SuccessionAct, art. 5(1).
[176] United Nations, "Common Country Assessment: Zambia 2000," p. 16.
[177] Human Rights Watch interview with First Lady of Zambia, Mrs. Maureen Mwanawasa, Lusaka, February 5, 2007 and Christine Kalamwina, director of Social, Legal, and Governance Affairs, GIDD, Lusaka, February 14, 2007.
[178] Human Rights Watch group interview with staff at Women for Change, Lusaka, February 2, 2007, and Matrine Chuulu, WLSA regional coordinator, Lusaka, January 28, 2007.
[179] Human Rights Watch interview with Bradford Machila, deputy minister of justice, Lusaka, February 5, 2007, Christine Kalamwina, director of Social, Legal, and Governance Affairs,GIDD, Lusaka, February 14, 2007, and Engwase Mwale, executive director, Nongovernmental Organizations' Coordinating Council, Lusaka, February 13, 2007.
[180] When it was established, the unit used to receive direct funding from Danida, Finnish Aid, and UNICEF.Currently it is funded indirectly through the Ministry of Home Affairs.Human Rights Watch interview with senior officer at the VSU, [name withheld], Lusaka, February 2007.
[181] Human Rights Watch interview with Tresphord Kasale, head of the Community Service Department, Lusaka, February 22, 2007, and Suzanne Matale, gender and justice desk officer, Zambia Council of Churches, Lusaka, January 31, 2007.
[182] Human Rights Watch interview with Theresa Chidothi, nurse and counselor, Kafue, February 7, 2007.
[183] Human Rights Watch interview with Tresphord Kasale, head of the Community Service Department, Lusaka, February 22, 2007.
[184] Central Statistics Office, Census of Population and Housing, (Lusaka: CSO, 2003).
[185] Ibid.
[186] Several individuals interviewed for this report told Human Rights Watch that police officers sometimes feel demoted if stationed at a VSU and as a result they demand to be transferred to other units.Human Rights Watch group interview with YWCA staff, Lusaka, February 1, 2007, and Tresphord Kasale, Lusaka, February 22, 2007.
[187] Human Rights Watch interview with Katembu Kaumba, Director of YWCA (group interview with staff members of YWCA), Lusaka, February 1, 2007.
[188] Interview with Phiri Paul Charles, VSU officer at Kabwata Police station and at the one-stop center, Lusaka, February2007.
[189]Human Rights Watch interview with Katembu Kaumba, Lusaka, February 1, 2007.
[190]Human Rights Watch interview with Greg Marcus, second secretary, Embassy of the United States in Zambia, Lusaka, February 14, 2007.
[191]WLSA, Justice in Zambia: Myth or Reality?Women and the Administration of Justice, p.130.
[192]Human Rights Watch interview with Muzi Kamanga, legal advisory officer, WiLDAF, Lusaka, January 29, 2007.
[193] Ibid.
[194] Human Rights Watch interview with Mercy Z., Lusaka, February 21, 2007.
[195] Human Rights Watch interview with Julie P. on behalf of her sister, Lusaka, February 8, 2007.
[196] Human Rights Watch interview with Rumbidzai Mutasa, legal officer at the Women's Legal Aid Clinic, Lusaka, February 23, 2007.
[197] WLSA, "Preface" in Justice in Zambia: Myth or Reality?
[198] Government of Zambia, "Zambia's Initial State Report on the Implementation of the African Charter on Human and Peoples' [sic.] Rights," May, 2007.
[199] Human Rights Watch group interview with YWCA's director, programs manager, and shelter manager, Lusaka, February 1, 2007.
[200] Human Rights Watch interview with Katembu Kaumba, director of YWCA, Nairobi, July 8, 2007.
[201] Human Rights Watch meeting with 16 representatives of NGOs, HIV support groups, NAC, and the police, Lusaka, February 23, 2007.
[202]Republic of Zambia, National Gender Policy (Lusaka: Gender in Development Division, 2000), pp. 65-66.
[203] After independence, women's issues were coordinated by the women's unit in the then ruling party.In 1985, a women's unit was introduced at the National Commission for Development Planning.This unit was upgraded in 1990 to the Women in Development Department, and mandated with coordinating, monitoring and evaluating national gender related policies.In 1996, the WIDD was elevated to the Gender in Development Division at Cabinet Office. WiLDAF, "Elimination of Discrimination Against Women in Zambia," p. 15.
[204] Human Rights Watch interview with Christine Kalamwina, senior officer at the Social, Legal, and Governance Division, GIDD, Lusaka, February 14, 2007.
[205] Human Rights Watch interview with Josephine Mwenda, principal economist, Ministry of Finance and National Planning, Lusaka, February 21, 2007.
[206] Human Rights Watch interview with Ng'andu P. Magande, minister of finance, Lusaka, February 16, 2007.
[207] "Zambia 365 Day Action Plan to End Gender-Based Violence" Draft Submission to GIDD, Zamcom Lodge, Lusaka, August 2007,http://www.genderlinks.org.za/attachment_view.php?ia_id=187 (accessed August 20, 2007), p. 2.
[208] Ibid., p.2.
[209] Human Rights Watch email correspondence with Samuel Mutale, specialist, Information Management, GIDD, August 21, 2007.
[210] "Zambia 365 Day Action Plan to End Gender-Based Violence," p.5.
[211] Human Rights Watch interview with Joy Lubinga, HIV desk officer, Council of Churches in Zambia and coordinator, Circles of Hope Support Groups, Lusaka, January 30, 2007.
[212] Zambia has ratified the following relevant treaties: the Convention on the Elimination of All Forms of Discrimination against Women (CEDAW), the International Covenant on Economic, Social and Cultural Rights (ICESCR), the International Covenant on Civil and Political Rights (ICCPR), the African Charter on Human and Peoples' Rights, and the Protocol to the African Charter on Human and Peoples' Rights on Women's Rights in Africa.Zambia is also a signatory to the 1997 SADC declaration on Gender and Development and its addendum on the Prevention and Eradication of Violence Against Women and Children (1998), where SADC leaders affirmed their commitment to the prevention and eradication of gender-based violence in the region.Zambia has not domesticated many of these treaties, however.While this does not absolve the country from its international legal obligations, it affects domestic enforceability.Human Rights Watch interview with Engwase Mwale, executive director, NGOCC, Lusaka, February 13, 2007.
[213] Adopted and opened for signature, ratification and, accession by General Assembly Resolution 34/180 of December 18, 1979, entry into force December 3, 1981.Zambia ratified CEDAW on June 21, 1985.
[214] See for example the UN Committee on the Elimination of Discrimination against Women, General Recommendation 19, Violence against Women, (Eleventh session, 1992),Compilation of General Comments and General Recommendations Adopted by Human Rights Treaty Bodies, UNDoc\HRI\GEN\1\Rev.7 (1994), para. 1.
[215]African [Banjul] Charter on Human and Peoples' Rights, adopted June 27, 1981, OAU Doc. CAB/LEG/67/3 rev. 5, 21 I.L.M. 58 (1982), entered into force October 21, 1986, art. 2.
[216] Ibid., art. 18(3).
[217] The Protocol to the African Charter on Human and Peoples' Rights on the Rights of Women in Africa, adopted by the second Ordinary Session of the Assembly of the Union, Maputo, September 13, 2000, CAB/LEG/66.6, entered into force November 25, 2005, art. 3(1).
[218] Ibid., art. 4.
[219] Ibid., art. 4 (a-c, f).
[220] International Covenant on Economic, Social and Cultural Rights. (ICESCR), adopted December 16, 1966, G.A. Res. 2200A (XXI), 21 U.S. GAOR Supp. (No. 16) at 49, U.N. Doc. A/6316 (1966), 993 U.N.T.S. 3, entered into force January 3, 1976.
[221] UN Committee on Economic, Social and Cultural Rights, "Substantive Issues Arising in the Implementation of the International Covenant on Economic, Social and Cultural Rights," General Comment No. 14, The Right to the Highest Attainable Standard of Health, E/C.12/2000/4 (2000), para. 14(20).
[222] Ibid., para. 21.
[223] Ibid., para. 21.
[224] Ibid., para. 51.
[225] Ibid., para. 52.
[226] Ibid., para. 52.
[227] Convention on the Elimination of All Forms of Discrimination against Women (CEDAW), adopted December 18, 1979, G.A. res. 34/180, 34 U.N. GAOR Supp. (No. 46) at 193, U.N. Doc. A/34/46, entered into force September 3, 1981, art. 15(2).
[228] Ibid., art. 16, para. 1(c).
[229] Ibid., art. 16, para. 1(h).
[230]UN Committee on the Elimination of Discrimination against Women, General Recommendation 21, Equality in Marriage and Family Relations, (13th session, 1994).
[231] Ibid., para. 26.
[232] Ibid., para. 28.
[233] Protocol to the African Charter on Human And Peoples' Rights On The Rights Of Women In Africa, art. 6.
[234] Ibid., art. 7.
[235] Ibid., art. 6(j).
[236] Ibid., art. 7(d).
[237]UN Committee on the Elimination of Discrimination against Women,General Recommendation 21, Equality in Marriage and Family Relations, para. 35.Para. 34 of this recommendation requires party states to include comments on inheritance laws (both statutory and customary) and their effects on women.
[238] Office of the High Commissioner for Human Rights and UNAIDS, "HIVAIDS and Human Rights: International Guidelines," from the second international consultation on HIV/AIDS and human rights, September 23-25, 1996, Geneva), U.N. Doc. HR/PUB/98/1, Geneva, 1998, art. 61.
[239] Human Rights Watch interview with Matrine Chuulu, WLSA regional coordinator, Lusaka, January 28, 2007. See alsoWLSA, "Report of the Situational Analysis on the Development of an HIV/AIDS Human Rights Charter," unpublished draft, on file with Human Rights Watch.
[240] UNAIDS, UNAIDS Regional Support Team for East and Southern Africa:Annual Report 2004 (Johannesburg:UNAIDS, 2005), p. 9.
[241] WHO, Towards Universal Access by 2010:How WHO is Working with Countries to Scale-Up HIV Prevention, Treatment, Care and Support , p. 5.
[242] The former UN Secretary General appointed James Morris as his Special Envoy for Humanitarian Needs in Southern Africa in July, 2002.
[243] UN Secretary-General's Taskforce on Women, Girls and AIDS in Southern Africa, "National Report: Zambia," September, 2003.The final version of the report is entitled "Facing the Future Together: Zambia Country Report of the United Nations Secretary-General's Taskforce on Women, Girls, and HIV/AIDS in Southern Africa," 2004.For an elaborate account of the work of the task-force and lack of follow up see Stephen Lewis, Race Against Time: Searching for Hope in AIDS-Ravaged Africa (Toronto: Anansi, 2005), pp. 133-142.
[244] UN Secretary-General's Taskforce on Women, Girls and AIDS in Southern Africa, "National Report: Zambia," p. 3.
[245] WHO, Towards Universal Access by 2010, p. 12.
[246] On May 30, 2007, President Bush announced his intention to work with Congress towards PEPFAR reauthorization.He presented a five-year, $30 billion proposal, which would be in addition to the United States initial $15 billion commitment made in 2003. The United States President's Emergency Plan for AIDS Relief (PEPFAR), "Reauthorizing PEPFAR," July 2007, http://www.pepfar.gov/press/88590.htm (accessed August 1, 2007).
[247] Human Rights Watch interview with Greg Marcus, second secretary, Embassy of the United States in Zambia, Lusaka, February 14, 2007 and PEPFAR, "2007 Country Profile: Zambia," http://www.pepfar.gov/press/81694.htm (accessed September 15, 2007).
[248] PEPFAR, "2007 Country Profile: Zambia."
[249]In 2005 the Office of the US Global AIDS Coordinator formed a Gender Technical Working Group to provide technical support to focus countries on gender and HIV.During the financial year 2006 PEPFAR allocated $104 million to support activities on gender-based violence in focus countries.
[250]For example, the Global AIDS Alliance wrote the following about PEPFAR's response to gender-based violence in countries such as Zambia: "[p]rograms designed to prevent and respond to gender-based violence, a major risk factor for HIV, are not well funded as discrete programs, and a lack of transparency makes it nearly impossible to determine their efficacy and impact." The Global AIDS Alliance, "First Lady's Trip to Africa Highlights Problems with US Policies on Health and Education," http://www.globalaidsalliance.org/index.php/673/ (accessed August 3, 2007).
[251] In July 2007 USAID issued an Annual Program Statement on WJEI, where it called for grants applications from US and Zambian private voluntary organizations, toward programs that aim at reducing gender-based violence, for up to US$5.369 million in four provinces in Zambia, including Lusaka and the Copperbelt.This includes $ 1.7 million for "raising awareness" and $3.7M for "victim support, rehabilitation, and reintegration." A separate program, administered by the Department of Justice, will complement these activities.It will focus on "the justice sector response to gender-based violence." USAID, "USAID's Annual Program Statement on The Presidential Women's Justice & Empowerment Initiative (WJEI)," APS Number: M-OAA-EGAT-WID-07-250, July, 2007, http://www07.grants.gov/search/announce.do;jsessionid=HqrFQ7K1r51Gnxkx1plsMQCp5LJCr1s34JZPf3tJpX5J21JJrY28!1320028050 (accessed November 1, 2007), p. 12.
[252] Human Rights Watch interview with Greg Marcus, second secretary, Embassy of the United States, Lusaka, February 14, 2007. See also United States Department of State, "Presidential Initiatives," http://www.usaid.gov/about_usaid/presidential_initiative/init_othermech.html#wje (accessed September 18, 2007).
[253] United States Department of State, "Women's Justice and Empowerment Initiative," http://www.state.gov/p/af/rt/wjei/ (accessed September 18, 2007).
[254] Phone communication with Camille E. Jackson, Office of Economic Policy Staff, US Department of State, Washington DC, November 1, 2007.Jackson told Human Rights Watch that USAID and the Department of Justice were negotiating an agreement with the Zambian government.
[255] United States Department of State, "Women's Justice and Empowerment Initiative."
[256] Ibid.
[257]United States Leadership Against HIV/AIDS, Tuberculosis, and Malaria Act of 2003, Pub.L. No. 108-25, sect.403(a).See also "President's Emergency Plan for AIDS Relief," http://www.avert.org/pepfar.htm (accessed September 2, 2007).
[258] In 2006 the United States Government Accountability Office (GAO) reported that the Office of the US Global AIDS Coordinator advised Congress in 2004 that it defined abstinence-until-marriage activities to include those that promote both abstinence and fidelity. OGAC stated that "abstinence-until-marriage programswould focus on achieving two goals: (1) encouraging individuals to be abstinent from sexual activity outside of marriage to protect themselves from exposure to HIV and other sexually transmitted infections and (2) encouraging individuals to practice fidelity in sexual relationships, including marriage, to reduce their risk of exposure to HIV."GAO, "Global Health: Spending Requirement Presents Challenges for Allocating Prevention Funding under the President's Emergency Plan for AIDS Relief," GAO-06-395, April 2006,http://www.gao.gov/new.items/d06395.pdf (accessed November 17, 2007), p. 14
[259] "HIV Prevention Policy Needs an Urgent Cure," The Lancet, 367(9518), April 15-21, 2006.
[260] Health Triangle Trust Kabwe, "Press Statement by Health Triangle Trust on the Occasion of the Visit of the US First Lady," June 28, 2007,http://www.globalaidsalliance.org/index.php/646 (accessed August 19, 2007)
[261] Ibid.
[262]''Protection against Transmission of HIV for Women and Youth Act of 2006''(The PATHWAY Act), 109th US Congress, 2nd Session, 2006, http://www.pepfarwatch.org/pubs/WomenandAIDSLeeBill.pdf (accessed October 17, 2007)
[263] African Capacity Investment Act of 2007 (introduced in US Senate and House, 2007).
[264] Ibid., sec.5.
[265] Human Rights Watch interview with Elizabeth Mataka, executive director of Zambia National AIDS Network and member of Zambia's Country Coordinating Mechanism, Lusaka, February 14, 2007.
[266] USAID, Addressing Gender-based Violence through USAID's Health Programs; Pan American Health Organization (PAHO), Violence Against Women: The Health Sector response (Washington, DC: PAHO, 2003); and UNFPA, Practical Approach to Gender-based Violence: A Programme Guide for Health Care Providers and Managers(New York: UNFPA, 2002), http://www.unfpa.org/upload/lib_pub_file/99_filename_genderbased.pdf (accessed April 17, 2007).Also see UNFPA, Programming to Address Violence Against Women: 10 Case Studies. (New York: UNFPA, 2007), chapters 1, 5 and 8; and A. Guedes, "Addressing Gender-Based Violence from the Reproductive Health/HIV Sector: A Literature Review and Analysis."
[267] UNFPA, "Gender Based Violence and HIV and AIDS: A Training Manual," 2004. In Zambia UNFPA's activities in the area of gender and HIV/AIDS currently focus on adolescent girls' attitudes to sex, dating, and HIV.The agency also places United Nations Volunteers who cover gender and AIDS generally. Human Rights Watch interview with Mekia Mohamed Redi, gender and HIV/AIDS officer, UNFPA, Lusaka, February 14, 2007.
[268] USAID, Addressing Gender-based Violence through USAID's Health Programs, pp. 11-12.
[269] Gender norms are the "learned and evolving beliefs and customs in a society that define what is 'socially acceptable' in terms of roles, behaviors, and status for both men and women.In the context of HIV/AIDS, these gender norms strongly influence both men's and women's risk-taking behavioras well as HIV treatment."UNAIDS, "Summary Presentation of Findings of HIV and Gender Assessments of National HIV Responses and Draft Policy Guidelines to Address Gender Equality and Equity," 20th Meeting of the UNAIDS Program Coordinating Board, Geneva, Switzerland, June 25-27, 2007, p. 3.
[270] Ibid., p. 22.
[271] Ibid., p. 22.
[272] Ibid., p. 24.
[273] Human Rights Watch email correspondence from Ngaitila Phiri, USAID, Lusaka, August 3, 2007.
[274] PAHO, Violence against Women: The Health Sector Responds.
[275] Ibid., pp.43-46.
[276] Southern Africa AIDS Trust (SAT) - Harare, "Counseling Guidelines on Domestic Violence," 2004, http://www.satregional.org/attachments/Publications/Skills%20Training%20E/Domestic%20Violence.pdf (accessed May 20, 2007).
[277] Ibid., p. 6.