
“Treat Us Like Human Beings”
Discrimination against Sex Workers, Sexual and Gender Minorities, and People Who Use Drugs in Tanzania
Glossary
Biological Sex: Biological classification of bodies as female or male based on factors such as external sex organs, internal sexual and reproductive organs, hormones, and chromosomes.
Bisexual: Sexual orientation of a person who is sexually and romantically attracted to both women and men.
Gay: Synonym in many parts of the world for homosexual; used here to refer to the sexual orientation of a man whose primary sexual and romantic attraction is towards other men.
Gender: Social and cultural codes (as opposed to biological sex) used to distinguish between what a society considers "masculine" or "feminine" conduct.
Gender-Based Violence: Violence directed against a person based on gender or sex. Gender-based violence includes sexual violence, domestic violence, psychological abuse, sexual exploitation, sexual harassment, harmful traditional practices, and discriminatory practices based on gender.
Gender Identity: Person’s internal, deeply felt sense of being female or male, both, or something other than female and male. It does not necessarily correspond to the biological sex assigned at birth.
Heterosexual: Person whose primary sexual and romantic attraction, or sexual orientation, is toward people of the other sex.
Homophobia: Fear and contempt of homosexuals, usually based on negative stereotypes of homosexuality.
Homosexual: Sexual orientation of a person whose primary sexual and romantic attractions are toward people of the same sex.
Intersex People: People born with reproductive or sexual anatomy that does not seem to fit the typical definitions of “female” or “male”; for instance, they may have sexual organs that correspond to both sexes.
Key Populations/Key Populations at Higher Risk of HIV Exposure: Those most likely to be exposed to HIV or to transmit it. In most settings, those at high risk of HIV exposure include men who have sex with men, transgender persons, people who inject drugs, sex workers and their clients, and HIV-negative partners in serodiscordant couples (couples in which one partner is HIV-positive and one is HIV-negative). Each country should define the specific populations that are key to their epidemic and response based on the epidemiological and social context.[1]
LGBTI: Lesbian, gay, bisexual, transgender, and intersex; an inclusive term for groups and identities sometimes associated together as “sexual minorities.”
Lesbian: Sexual orientation of a woman whose primary sexual and romantic attraction is toward other women.
Maskani: Kiswahili slang term used to signify an outdoor location for using drugs.
Men Who Have Sex With Men (MSM): Men who have sexual relations with persons of the same sex, but may or may not identify themselves as gay or bisexual. MSM may or may not also have sexual relationships with women.
Most At-Risk Populations (MARPs): Used by public health workers to describe groups likely to be exposed to HIV or to transmit it. This report uses the terms “key populations” and “most at-risk populations” interchangeably. It also uses the terms “marginalized groups” and “vulnerable groups,” to refer collectively to sexual and gender minorities, sex workers, and people who use drugs.
Panga: Kiswahili word for machete.
People Who Inject Drugs/People Who Use Drugs: Used here instead of “injecting drug users” (IDUs) or “drug users,” terms that some drug users reject as defining them based on drug use alone. In Kiswahili, the non-pejorative slang term “teja” (plural: “mateja”) is often used to refer to people who use drugs; “mtumiaji wa madawa ya kulevya” (literally, person who uses drugs) is also used.
Police Form Number 3 (PF3): Form that police must fill out before most Tanzanian hospitals will treat victims of assault.
Police Jamii: Community police; groups of civilians in mainland Tanzania and Zanzibar that provide information to the police and in some cases carry out patrols.
Sexual Minorities: Inclusive term that includes all persons with non-conforming sexualities and gender identities, such as LGBTI, men who have sex with men (and may not self-identify as LGBTI) and women who have sex with women.
Sexual Orientation: The way a person’s sexual and romantic desires are directed. The term describes whether a person is attracted primarily to people of the same sex, the opposite sex, or to both. Kiswahili, Tanzania’s national language, has a number of derogatory terms to describe people whose sexual orientation is not heterosexual. They include “shoga” and “msenge” (used to refer to men who have sex with men) and “msagaji” (used to refer to women who have sex with women). These terms are sometimes used by LGBTI people themselves in a non-derogatory way to refer to themselves or community members. “Mtu mwenye uhusiano we jinsia moja” (“a person having same-gender relationships”) is a neutral, non-offensive way to refer to someone who has same-sex relationships.
Sex Workers: Used here to refer to adult women and men who provide sexual services in exchange for money. Child sex work is strictly prohibited under international law and is a form of commercial sexual exploitation. Children engaged in sex work, however, should never be treated as criminals but are entitled to protection from the state from such exploitation and provided with appropriate assistance.
Sungu Sungu: Initially used to refer to a vigilante group formed to combat cattle rustling in western Tanzania in the 1980s; more recently, the term has come to be used to describe any neighborhood militia. (Also “Sungusungu.”)
Transgender: The gender identity of people whose birth gender (which they were declared to have upon birth) does not conform to their lived and/or perceived gender (the gender that they are most comfortable with expressing or would express given a choice). A transgender person usually adopts, or would prefer to adopt, a gender expression in consonance with their preferred gender, but may or may not desire to permanently alter their bodily characteristics in order to conform to their preferred gender.
Women Who Have Sex With Women (WSW): Women who may or may not identify as lesbian or bisexual; some WSW may also have sexual relationships with men.
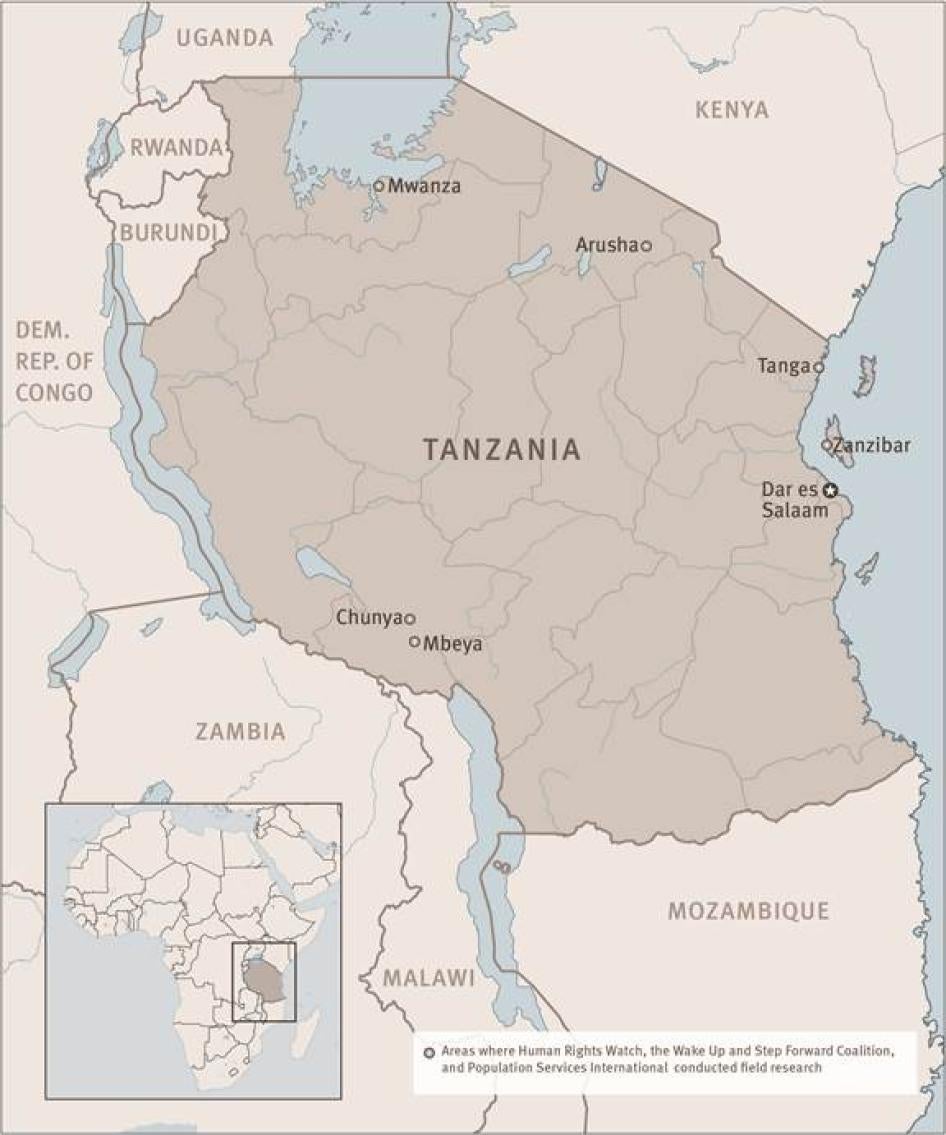
Map of Tanzania
© 2013 Human Rights Watch
Summary
In December 2010, police arrested Saidi W., an 18-year-old man in Dar es Salaam, Tanzania, who identifies as gay. A police officer forced him at gunpoint to call five gay friends and tell them to meet him at a bar. When they arrived, the police arrested all of them, undressed them at the bar, beat them, and took them to Central Police Station. There the men were repeatedly raped by fellow detainees. When Saidi and his friends asked the police for help, police said, “This is what you want.” Saidi’s mother had to pay 400,000 Tanzania shillings (Tsh) (about US$250) as a bribe to release her son and his friends.
* * *
In 2012, Mwamini K., a female sex worker, was raped at gunpoint by a client who got angry when she asked that he use a condom. Mistrustful of police and hospitals, she was afraid to seek help: in 2011, when she was in the street in Dar es Salaam soliciting clients, three police officers caught her, called her a “dog” and a “pig,” and beat her for about 10 minutes before leaving her in the street. On that occasion, Mwamini went to the hospital for treatment, but told hospital workers that she had fallen down the stairs, afraid that she would be denied services if she told the truth about how she was beaten. She had also had problems with hospitals in the past: at one hospital, staff refused to treat her when she told them she had been infected with a sexually transmitted infection (STI) because of her sex work.
* * *
In December 2011, Dar es Salaam police arrested and tortured Suleiman R., who uses heroin, in an effort to extract a confession for a robbery he said he had not committed. They struck him with iron bars and burned his arm with a clothes iron. Police held Suleiman overnight and made his mother pay a Tsh 200,000 bribe ($125) to have him released the next day. Upon release, Suleiman asked the police to provide him with Police Form Number 3 (PF3), which public hospitals require before treating victims of assault. The police refused, saying, “If we give you a PF3, you will accuse the police in court.” Suleiman was forced to seek expensive treatment at a private hospital.
* * *
Saidi W., Mwamini K., and Suleiman R. have at least two things in common. First, they all belong to what public health specialists seeking to address the HIV/AIDS epidemic (see Glossary) refer to as “most at-risk populations” (MARPs) or “key populations.” While HIV prevalence among the general population has decreased in Tanzania, available data suggest it has increased among key populations, including men who have sex with men (MSM), sex workers, and people who inject drugs.
They also share another dubious distinction: Tanzanian law considers them all to be criminals. This criminal status drives them underground, making them easy targets for human rights violations by law enforcement officials; legitimizing stigma among the broader public; and giving government bodies an excuse to devote inadequate attention to key populations.
This report results from research conducted between May 2012 and April 2013 by Human Rights Watch and Wake Up and Step Forward Network (WASO), a Dar es Salaam-based network of groups that represent men who have sex with men. It documents human rights violations experienced by sex workers, people who use drugs, and lesbian, gay, bisexual, transgender, and intersex people (LGBTI), including MSM. It also exposes the very troubling situation of sexual exploitation of children in sex work. The report highlights two main categories of human rights violations: those for which law enforcement officials bear primary responsibility, and those within the health sector.
Violations by the Police
The research documents dozens of grave human rights violations by the police, including torture and rape, assault, arbitrary arrest, and extortion, as well as refusal to accept complaints from members of vulnerable groups that have been victims of crime. In one especially horrific case, police arrested John Elias, a heroin user, in a drug bust in the Kigamboni area of Dar es Salaam in February 18, 2010. At the police post, a police officer injected both of Elias’s eyes with a syringe full of liquid. A week later, when Elias went to the hospital, he discovered the liquid was acid. Today, Elias has gaping holes where his eyes should be.
Semi-official security forces, most notably the Sungu Sungu, a vigilante group, are also implicated in violence against at-risk populations, “policing” their behavior, often through the use of force. Their abuses include an attack on Mwanahamisi K. near the railroad in Tandika, Dar es Salaam, in May 2012, where she had gone to smoke heroin. She told Human Rights Watch: “Six of them forced me to have sex with them…. They didn’t use condoms. The rape lasted one or two hours. I was with my child. The baby boy was lying on the ground to the side while I was being raped…. After raping me, they told me “Don’t move around at night.”
Further reinforcing the second-class status of vulnerable groups, police sometimes refuse to accept complaints when sex workers, people who use drugs, or LGBTI people are victims of crime, whether by the security forces themselves or by private citizens. As a public health worker in Mwanza explained, “Sex workers do not have a place to speak against injustices done to them, and the police can take advantage of them if they go and report. If they go to the police, the police just become their customers for that night.”
All of these human rights violations reinforce stigma and contribute to an environment in which men who have sex with men, sex workers, and people who inject drugs become increasingly marginalized and distrustful of the state, undermining public health initiatives that depend on cooperation and partnership between the government and populations that are most at risk of HIV infection.
Among all three key populations, our research suggests that those who are the most vulnerable to police abuse are from lower socioeconomic classes. In all cases highlighted here, state actors and their proxies operate with impunity.
Violations within the Health Sector
Human rights violations within the health sector include denial of services, verbal harassment and abuse, and violations of confidentiality. Such incidents include a 2011 case in Dar es Salaam’s Temeke hospital when staff refused to use anesthesia when stitching up a person who uses drugs after he was attacked by a mob, and an incident in March 2012 when a doctor at Zanzibar’s Mnazi Mmoja Hospital refused to treat a gay man for gonorrhea, declaring, “You already have sex with men, now you come here to bring us problems. Go away.”
The report also documents onerous requirements in the health sector that, while not intended to discriminate, pose particular obstacles to access to health care for men who have sex with men, sex workers, and people who use drugs. For example, Jamila H., a sex worker, was gang-raped in February 2012 and went to a public hospital, but she was told she needed the police to fill out a form about the assault before she could receive treatment. “They said I should go to the police, but I couldn’t because I was a sex worker,” she said. Two of her rapists had not used condoms, but without access to hospital services, she did not get tested for HIV. Halima Y., also a sex worker, said health workers at Mwananyamala Hospital in Dar es Salaam refused to treat her for an STI because she could not comply with a requirement to bring in her sexual partner for testing and treatment.
Discriminatory treatment, combined with the absence of clear messages from the government that no one will be arrested or persecuted for seeking services, leads people to stay away from health services. When police or semi-official vigilante groups mistreat or arbitrarily arrest members of any marginalized group, or when health workers deny them services, their actions also violate clear international human rights principles, and also often violate Tanzanian law.
Most At-Risk Populations (MARPs)/Key Populations
The Tanzanian Ministry of Health and Social Welfare, like many health ministries around the world, has recognized that men who have sex with men (MSM), sex workers, and people who inject drugs are essential partners in the fight against HIV.
Tanzania’s Second National Multi-sectoral Strategic Framework on HIV and AIDS, 2008-2012, recognized that stigma inhibits access to services. (An updated strategic framework for 2013 to 2017 was being drafted as of this writing.) The Strategic Framework set forth several strategies aimed at reducing the risk of infection among the “most vulnerable,” including men who have sex with men, sex workers, and people who inject drugs. These included three particularly critical strategies. The framework pledged, in its own words:
- To promote increased access to HIV preventive information and services (IEC [Information, Education and Communication], condom access, peer education, friendly testing and counseling and STIs services) for the vulnerable populations.
- To build partnerships between government and CSOs [civil society organizations] and other agencies working with vulnerable populations to advocate for their empowerment and protection and stimulate documentation and exchange of experiences.
- To acknowledge the vulnerability of sex workers and men who have sex with men and advocate for their access to HIV preventive information and services and for decriminalization of their activities. (The Kiswahili version of the Strategic Framework uses slightly different language, discussed below.)
In Zanzibar—a semi-autonomous territory that maintains a political union with Tanzania, but has its own parliament and president—the National HIV Strategic Plan II (2011-1016) does not specifically call for decriminalizing sex work or consensual sex amongst men, but it recommends a national advocacy campaign promoting tolerance toward key populations. It also calls for other progressive measures, including needle exchange for people who inject drugs and for condoms and water-based lubricant to be distributed to men who have sex with men.
Unfortunately, existing law, combined with abusive practices by both law enforcement and health officials, undermines all these strategies, both in the mainland and in Zanzibar.
Criminals under the Law
Tanzanian law criminalizes consensual sexual conduct between adult males, with a penalty of 30 years to life in prison, one of the most severe punishments for same-sex intimacy in the world. Zanzibar has slightly different laws but criminalizes both male homosexual conduct and lesbianism. In both regions, prosecutions for same-sex conduct have not taken place in recent years, but the law—and the abusive way that it is often enforced—keeps lesbian, gay, bisexual, transgender, and intersex (LGBTI) people marginalized. It also makes them more vulnerable to police blackmail and extortion as they seek to maintain their secret status.
Tanzanian law also criminalizes sex work: loitering for the purposes of prostitution carries a three-month prison penalty on the mainland, and providing sex in exchange for money carries a three-year penalty in Zanzibar.
Personal use of any narcotic drug or psychotropic substance is punishable by 10 years in prison on the mainland, a fine of Tsh 1 million (about $614), or both. In Zanzibar, it is punishable by up to seven years in prison.
Children
The use, offer, procurement, or provision of a child under 18 years old for sex work is a form of commercial sexual exploitation. This is prohibited under both Tanzanian and international law. Children who engage in sex work, or are otherwise commercially sexually exploited, should not be prosecuted or penalized for having been party to illegal sex work, but should receive appropriate assistance. Those who commit crimes of sexual exploitation should be prosecuted. However, commercial sexual exploitation of children—especially of girls—is frequent in Tanzania and usually goes unpunished. Moreover, children engaged in sex work with whom we spoke are frequently victims of police abuse and have no remedy against violence by private actors. Some of the most serious human rights violations we documented involved police raping children involved in sex work. For instance, Rosemary I., a child engaged in sex work in Mbeya, told us that police had raped her “about seven times,” the first time when she was just 12. According to the US State Department, no one was prosecuted in Tanzania in 2012 for sexual exploitation of children.
Limited Progress
Some progress has been achieved under the existing Strategic Framework and Strategic Plan, with a few state hospitals and some nongovernmental organizations (NGOs) throughout the country providing “MARPs-friendly” services. The government has also, through its health agencies, supported several outreach programs implemented by local and international organizations that target key populations. However, health workers continue to discriminate against patients based on their presumed sexual orientation, engagement in sex work, or drug use, compromising their right to the highest attainable standard of health.
The conduct of Tanzanian state agents systematically undermines the framework’s strategies, including its pledge to “promote increased access to HIV preventive information and services,” including “friendly testing,” to vulnerable groups. Many people interviewed for this report said that discriminatory treatment still poses a serious obstacle to testing and treatment. When it comes to access to information, marginalized groups, particularly men who have sex with men, are often ignored by public outreach campaigns around HIV/AIDS.
The Strategic Framework pledges to “build partnerships between government and CSOs [civil society organizations] and other agencies working with vulnerable populations to advocate for their empowerment and protection.” The government has, through its health agencies, supported several outreach programs implemented by CSOs and other non-governmental organizations (NGOs) targeting key populations. But the best representatives of vulnerable populations’ needs are membership organizations composed of those populations themselves – and in a context where men who have sex with men, sex workers, and people who use drugs face a constant threat of violence at the hands of police and other state actors, including torture and rape, it is difficult to speak of a “partnership” between these groups and the government.
MSM and sex worker activists told us that they were not aware of any efforts by government health agencies to advocate for decriminalization of same-sex conduct or sex work since the Strategic Framework was published, despite its commitment to “acknowledge the vulnerability of sex workers and men who have sex with men and advocate for their access to HIV preventive information and services and for decriminalization of their activities.” In early 2013, a government health official informed Human Rights Watch that his agency was beginning to reach out to police, with hopes of initiating discussions on decriminalization. But no further concrete advocacy initiatives – which would ultimately have to include lawmakers, not just police – had been undertaken. This may be due, in part, to some public officials’ lack of awareness of the Strategic Framework’s content in English: Human Rights Watch discovered that where the English version calls for “decriminalization of their activities,” the Kiswahili version only calls for “not scorning their activities” (kutokudharau shughuli zao).
A Holistic, Rights-Based Approach to HIV/AIDS
If Tanzania is truly committed to addressing HIV/AIDS among key populations, it should do so holistically. Institutions in the public eye, such as police and the health sector, should provide protection and treatment to at-risk groups, modeling positive behavior to other Tanzanians, rather than setting an example of hatred and bigotry.
Tanzanian laws and practices toward men who have sex with men, sex workers, and people who use drugs do not only prevent full realization of Tanzania’s commitment to stamp out HIV, they also violate international law. The criminalization of voluntary, consensual sexual relations amongadults is incompatible with respect for a number of internationally recognized human rights, including the rights to privacy and non-discrimination. Criminalization of the voluntary, commercial exchange of sexual services, as in the case of consensual sex work by adults, is also incompatible with the right to privacy, including personal autonomy. Human rights violations also often accompany enforcement of both sets of criminal laws, and enforcement of criminal laws against drug use and possession for personal use.
Human Rights Watch and WASO call on Tanzania to uphold human rights for all people, including marginalized groups. The Criminal Code should reflect principles of equality, rather than cementing discrimination into law. State agents’ actions should consistently reflect an understanding that LGBTI people (including men who have sex with men), sex workers, and people who use drugs are entitled to the full spectrum of rights enjoyed by other Tanzanians.
There is a clear link between human rights and the public health imperative to reduce HIV infections and treat existing ones. Ending discrimination and abuse against key populations is both a public health imperative, and a question of basic human dignity.
Key Recommendations
To President Kikwete
- Publicly call for an end to police abuse, discrimination in the health care sector, and all other forms of discrimination against sex workers, people who use drugs, and lesbian, gay, bisexual, transgender, and intersex people.
To the Government of the United Republic of Tanzania
- Establish an independent civilian policing oversight authority mandated to receive complaints regarding police misconduct, carry out investigations, and refer such complaints to prosecutors.
To the Parliaments of Tanzania and Zanzibar
- Begin decriminalizing consensual sexual activity between adults, including same-sex conduct and consensual adult sex work. Also review laws on personal drug consumption and possession in order to ensure they are consistent with public health and human rights imperatives.
To the Ministry of Health and Social Welfare of the Republic of Tanzania, Ministry of Health of Zanzibar, and all Government Institutions Working on HIV/AIDS
- Issue orders to health workers that discrimination against members of marginalized groups will not be tolerated, and conduct trainings and inspections to ensure this order is followed.
To the Tanzania Police and Office of the Director of Public Prosecutions
- Issue orders to all police that no crime victim should be denied assistance, arrested, or harassed on the basis of their sexual orientation or gender identity, or their status as a sex worker or drug user. Publicly announce that members of at-risk populations can report crimes without facing the risk of arrest, and establish police liaisons to these communities.
To Donor Governments and Institutions Supporting HIV/AIDS Programs or Human Rights Programs in Tanzania
- Support the development of membership organizations among sex workers, LGBTI people, and people who use drugs, such that these persons can have collective institutional voices.
- Ensure that funding directed to HIV/AIDS in Tanzania includes funds specifically aimed at key populations’ health needs.
Methodology
This report is a collaboration between Human Rights Watch and the Wake Up and Step Forward Coalition (WASO), a coalition of organizations serving men who have sex with men (MSM) in Dar es Salaam. The Tanzania Gender Networking Program (TGNP) and the Nyerere Centre for Human Rights, both based in Dar es Salaam, also helped to conceive and research this report.
Between May 2012 and April 2013, Human Rights Watch and WASO conducted field research in Dar es Salaam, Zanzibar, Tanga, Arusha, and Mwanza. Human Rights Watch conducted additional research in Mbeya and Chunya with the assistance of Population Services International (PSI), an international NGO focusing on reproductive and sexual health.
Two Human Rights Watch researchers and two WASO researchers interviewed 254 people for this report, including 121 members of key populations:
- 47 men who have sex with men (14 of whom also engaged in sex work, either occasionally or as a full-time occupation)
- 3 transgender people (two male-to-female and one female-to-male)
- 39 adult women sex workers
- 13 girls under 18 engaged in sex work
- 19 people who inject drugs, 5 of them female
Interviewers asked young women and girls engaged in sex work to state their own ages in order to determine which of them were children. In Tanzania, many people do not have birth certificates so exact age can be difficult to determine.
We also spoke with other members of vulnerable populations that are not necessarily considered most at-risk, including nine lesbians or women who have sex with women (WSW), one of whom was also a sex worker, and one of whom also identified as intersex; 13 people who use non-injection drugs; and 12 people who formerly used drugs.
Most interview subjects were approached with the assistance of local or international NGOs. In some cases, particularly where we could find no organizations working with female sex workers, we approached female sex workers in bars or in the street to request interviews with them.
In locations outside Dar es Salaam and Zanzibar, it was difficult to identify and interview members of key populations, in part because of a near-total absence of local organizations that liaise with them. Our two- to four-day visits to mid-size towns, where same-sex intimacy and other socially controversial issues are rarely discussed openly, did not allow sufficient time to gain the trust of a significant number of LGBTI people, sex workers, and people who use drugs. Due to this limitation, and the greater amount of time we spent conducting interviews in Dar es Salaam, this report includes many more case studies from Dar es Salaam compared to other parts of the country. Further research into the specific situations facing key populations in other parts of the country would be beneficial for stakeholders seeking to develop interventions that address their needs.
In each location, we spoke with local and international NGOs, specifically those engaged on issues such as HIV education and outreach, gender equality, and harm reduction.
We also interviewed officials from the government, including from the police; the Ministry of Health and Social Welfare; the Ministry of Gender, Youth, and Community Development; and the Preventing and Combating Corruption Bureau, as well as members of government commissions addressing human rights, HIV/AIDS, and drugs. We also interviewed academics at Muhimbili University and the University of Dar es Salaam who are conducting research on HIV among key populations.
Interviews were conducted in English and Kiswahili by researchers and a consultant fluent in those languages. Interview subjects who traveled to meet with us, generally on public buses, were reimbursed for transport and lunch, up to Tsh 5,000 ($3) depending on the distance traveled. All interview subjects consented to take part in our interviews, which they were informed would be included in a human rights report.
The names of most interview subjects from key population groups have been withheld to assure their anonymity. Each has been assigned a first name and an initial that bear no relation to their real name.
I. Background
HIV in Tanzania: High Prevalence amongst Key Populations
KEY DATES |
|
|
1983 |
First AIDS cases documented in mainland Tanzania.[2] |
|
1980s, early 90s |
HIV prevalence escalates rapidly. |
|
1996 |
AIDS epidemic peaks: 8.4 percent of the population aged 15-49 is infected with HIV.[3] |
|
1988 |
National AIDS Control Programme (NACP) set up to coordinate HIV/AIDS response. |
|
2001 |
Tanzania develops national AIDS policy, establishes the Tanzania Commission for AIDS (TACAIDS) to coordinate a multi-sectoral response. Rates begin to decline.[4] |
|
2007 |
Prevalence decreases to 5.8 percent.[5] |
|
2007-2012 |
Progress stagnates. |
|
2012 |
TACAIDS places prevalence at 5 percent.[6] |
A recent report by World Bank economists finds
Tanzania is falling behind other countries in the region in reducing Aids-related deaths.… The fact that so many Tanzanians still die from Aids, despite the existence of treatment, signals that the country’s health system does not reach those in need of HIV testing and therapy.[7]
Today, Tanzania ranks fourth in the world in terms of the total number of AIDS deaths.
The stagnation in reducing prevalence does not reflect lack of investment by Tanzania and its partners in the fight against HIV/AIDS. Between 2004 and 2012, the Global Fund to Fight AIDS, Tuberculosis and Malaria disbursed over US$400 million to Tanzania for HIV/AIDS.[8] And between 2009 and 2011, the United States President’s Emergency Plan for AIDS Relief (PEPFAR) gave Tanzania over $1 billion for HIV/AIDS prevention and treatment, signing a five-year partnership agreement with Tanzania’s government in 2010 that commits both the US and the Tanzanian government to reducing new HIV infections and AIDS-related deaths.[9] According to PEPFAR, the Tanzanian government has steadily increased its expenditures on HIV/AIDS activities, and there have been notable gains in public awareness, testing, and the availability of antiretroviral therapy (ART).[10]
But the stagnation in reducing prevalence suggests that some groups are not being reached. Among those hard-to-reach groups are those who belong to what public health agencies have identified as “key populations” or “most at-risk populations” (MARPs). These populations—comprising men who have sex with men (MSM), transgender people, people who inject drugs, and commercial sex workers—are most likely to be exposed to HIV or to transmit it.[11]
Indeed, while overall HIV prevalence hovers around 5 percent on the Tanzanian mainland, some studies indicate that rates are significantly higher among MSM, sex workers, and people who inject drugs. Reliable figures on a nationwide scale are not available. However:
- HIV prevalence was 31 percent among Dar es Salaam female sex workers compared to 10 percent among women in the general population, according to a 2010 NACP study;[12]
- A staggering 70 percent of female sex workers in Mbeya were HIV positive, according to a 2001 study;[13]
- HIV prevalence among men who have sex with men in Dar es Salaam is as high as 40 percent, according to preliminary results from a recent study;[14]
- An estimated 35 percent of people who inject drugs in Dar es Salaam have HIV.[15]
In semi-autonomous Zanzibar,[16] HIV prevalence among the general population has remained low—around 0.6 percent in 2008—since the first reported AIDS cases in 1986.[17] But Zanzibar faces a concentrated epidemic, with key populations bearing the brunt. According to government estimates, 12.8 percent of female sex workers, 10.8 percent of men who have sex with men, and 16 percent of people who inject drugs have HIV.[18]
Legal and Policy Environment
Health specialists have called upon governments to acknowledge the link between human rights and the public health imperative to reduce HIV infections and treat existing ones. As UNAIDS argues, criminalization and discrimination drive key populations away from essential services:
The criminalization of people who are at higher risk of infection, such as men who have sex with men, sex workers, transgender people and people who use drugs, drives them underground and away from HIV services. This increases their vulnerability to HIV, as well as to stigma, discrimination, marginalization and violence.[19]
The Global Commission on HIV and the Law, a commission of experts that the United Nations Development Programme (UNDP) established in 2010, also calls for decriminalizing sex work and same-sex conduct.[20] Even Zanzibar’s own National HIV Strategic Plan II recognizes the barriers erected by discriminatory laws and policies:
Discriminatory laws, and both unhelpful policies and regulatory frameworks, have had a negative bearing on some of the key sub populations limiting their access to services.[21]
However, Tanzania criminalizes the activities of all three groups. Consensual “carnal knowledge against the order of nature” is punishable in mainland Tanzania by a minimum of 30 years and a maximum of life in prison, [22] while “gross indecency” between males is punishable by five years in prison. [23] In Zanzibar, the law prohibits consensual same-sex relations between men (with a 14-year penalty) and women (with a 5-year penalty). [24] Zanzibar also criminalizes undefined “unions” between couples of the same sex. [25] The laws prohibiting same-sex conduct are rarely enforced, but do serve to drive LGBTI people underground.
Engaging in sex work is illegal in both mainland Tanzania and in Zanzibar, and sex workers are frequently arrested in both places.[26] Tanzania’s penal code punishes with three months in prison “loitering or soliciting in a public place for the purposes of prostitution.”[27] Zanzibar’s penal code is harsher, stating, “Any person who for consideration offers her or his body for sexual intercourse commits an offence and shall on conviction be liable to imprisonment for a term of three years.”[28]
Personal consumption of narcotic drugs and psychotropic substances is prohibited in both the mainland and in Zanzibar, with sentences ranging from seven to ten years.[29] A 2009 Zanzibar law allowed for an alternative sentence by which first-time offenders convicted of possessing a small quantity of drugs for personal consumption may be sentenced to six months in an education center followed by treatment at a rehabilitation center.[30] The law was modified in 2011, replacing the education center option with six months in prison.[31]
Tanzania’s Second National Multi-sectoral Strategic Framework on HIV and AIDS lists, as one strategy to reduce prevalence among vulnerable groups, “To acknowledge the vulnerability of sex workers and men who have sex with men and advocate … for decriminalization of their activities.”[32] But Tanzanian lawmakers have not engaged in serious discussion about decriminalizing same-sex conduct or sex work.
A former health official in Arusha, in northern Tanzania, confirmed that the criminalization of same-sex conduct made it more difficult to reach MSM in public health campaigns:
There is no specific program here for MARPs… it’s very difficult for the medical authorities to find them. We know they exist, but how can you access them when it’s illegal? If it were a legal activity, maybe it wouldn’t be difficult.[33]
Criminalization also complicates outreach by NGOs. The representative of an Arusha-based organization that conducts sensitizations on HIV and safer sex told Human Rights Watch and WASO that she had thought about trying to reach out to men who have sex with men, but had been afraid to do so, thinking that it was illegal to conduct workshops for MSM and that she would run into problems with the government.[34]
Mistrust of state officials—a result of both criminal laws and abusive practices—constitutes an obstacle to outreach work. In Zanzibar, a representative of the HIV/AIDS organization ZAYEDESA explained:
The police are a problem. In our HIV prevention work we had to convince them [key populations] that we’re not coming with the police to arrest them. [35]
In Mwanza, a representative of a local HIV/AIDS organization working with people who use drugs told Human Rights Watch, “We have to build trust with them, to explain that we are not from the government.”[36] Similarly, a representative of an international NGO seeking to do HIV outreach with sex workers in Mwanza said, “There is a need to sit and address some of the issues relevant to them. They need to know you, to build trust. They may think we want to chase them from this town.”[37]
Dr. Joyce Nyoni, a lecturer at the University of Dar es Salaam who is carrying out research among men who have sex with men, told Human Rights Watch that criminalization complicates academic research on key populations:
Because [same sex conduct] is illegal, it’s more difficult for us to do outreach and sensitization. It would be easier to find a platform to do so if it were legal. People are afraid to come to us. Just for doing the research I had an office outside the university. We had to do things in a low-key way, not have groups come…
The main challenge is, how do we reach them? It’s more difficult now with SIM cards being registered. They [the government] can track people. We were giving messages by cell phone about HIV/AIDS and condom use, to correct misinformation. Some thought condoms don’t prevent HIV/AIDS, or that anal sex doesn’t spread HIV/AIDS. It could be harder to do this programing now. [38]
Criminalization also gives other government bodies an excuse to devote inadequate attention to key populations. An official at the Commission on Human Rights and Good Governance (CHRAGG), Tanzania’s national human rights institution, told Human Rights Watch that the commission does not address rights abuses against LGBTI people. According to the official, “It’s sensitive, no one wants to talk about it. As a government institution, we can’t do it. It would be against the framework that is in place. It’s a criminal case.”
Despite having conducted no research on the subject, the CHRAGG official assured Human Rights Watch that key populations are nonetheless “not harassed or discriminated against.” [39]
Access to Information
Public health campaigns around HIV in Tanzania largely target heterosexual couples. In a study on condom use among MSM, the key researchers noted, “Almost no HIV prevention materials in Tanzania are written with MSM mentioned…. There is an urgent need for MSM-relevant and accessible HIV prevention materials.” The researchers attribute this information gap to the law that criminalizes sex between men, as well as to a social context “where MSM are almost universally denigrated.”[40]
The information gap contributes to ignorance on the part of some of the people most vulnerable to HIV. Dr. M.T. Leshabari, a public health professor at Muhimbili University, said he had encountered many misconceptions about HIV among MSM:
Some believe anal sex is not a form of transmission, because in popular sensitization campaigns in Tanzania, it’s sex between a man and a woman that is portrayed as a form of transmission. Some believe the anus is hot and can kill the virus; some believe they can flush it out afterwards. There is nothing specific for MSM in terms of public awareness campaigns.[41]
Human Rights Watch and WASO’s research also found evidence of these misperceptions. Daudi L., a gay man in Mwanza, told Human Rights Watch and WASO that he did not know HIV could be spread through anal sex.[42] Kashif M. told us he does not consider himself gay, but had anal sex with a man on one occasion, with no awareness of the risks:
I had sexual relations with a guy the other day. He wanted me to have sex with him, so I did it. I did not use a condom. I did not know you could get AIDS from anal sex.[43]
The Second National Multi-sectoral Strategic Framework on HIV and AIDS calls for collaboration between government and civil society groups representing key populations, but men who have sex with men, people who use drugs, and sex workers have few organizations that directly represent them, and are often excluded from public debates about issues that directly concern them.
As far as Human Rights Watch and WASO could ascertain, LGBTI organizations exist only in Dar es Salaam and Zanzibar. These organizations cannot operate with complete openness, as they are afraid of being shut down by the government, but they have established working relationships with government health institutions such as TACAIDS and the Zanzibar AIDS Commission. There are no harm reduction programs for people who use drugs outside of Dar es Salaam. There is currently no organization of any kind working with sex workers in Arusha, a tourist hub, despite the sizable sex worker population there.[44] While sex worker organizations exist in Dar es Salaam, none of them have even attempted to register with the government.
As noted above, some mainstream human rights organizations hesitate to reach out to key populations out of fear that programming for these marginalized groups may be illegal. The criminalization of key populations poses a challenge to human rights defenders. For the small but burgeoning community of self-identified human rights defenders in Tanzania, a lack of clarity regarding the legality of work with LGBTI people and sex workers—combined with intolerant attitudes on the part of some human rights defenders—poses a barrier to collaboration between LGBTI and sex worker activists and mainstream human rights groups. One human rights activist told Human Rights Watch that if the government were to demonstrate greater tolerance toward LGBTI people and sex workers, his network would feel safer in reaching out to marginalized groups and collaborating with them on addressing basic human rights violations, including arbitrary arrests, torture, and denial of access to health care and justice.[45]
Ujamaa and ExclusionUnder Tanzania’s first president, Julius Nyerere (1961-1985), Tanzania developed a unique ideology of African socialism, known as Ujamaa—Kiswahili for “relationship, kin, or brotherhood.” Nyerere’s Ujamaa was a socialist philosophy of development, said to be based on principles of freedom, equality, and unity. Nyerere established Kiswahili as the national language to promote national identity and prevent ethnic conflict. Tanzania’s constitution includes strong language on non-discrimination, human dignity, and the eradication of all forms of discrimination and injustice (see Section VII for citations). The model of national unity and non-discrimination has, in many regards, been effective. Tanzania is the only East African country that has not suffered vicious cycles of ethnic and political violence. For a country with large Christian and Muslim populations, religiously motivated violence is rare, although recent attacks on churches have raised concerns. [46] But Tanzania is not free from social exclusion. Due to either their immutable characteristics or their general social status, there have always been outsiders in Tanzania. In recent decades, “outcasts” have included groups such as people with albinism, refugees, and street children. [47] Further, an overstated emphasis on social cohesion has not always been good for human rights in Tanzania. A ruling party member of parliament (MP) told a journalist in 2012 following a wave of opposition protests, several of which the police shut down, “This is a country where consensus is valued—calm and peace is a big deal. Law enforcement authorities probably need to learn how to deal with this [new] kind of expression.”[48] Under an enforced veneer of unity, discussion of human rights can seem provocative. One Dar es Salaam-based activist explained, “There were no human rights organizations before because of the community system…. When we started to talk about human rights, for many in Tanzania, it was a strange thing.”[49] Discussion about the rights of marginalized groups, such as LGBTI people, sex workers, or people who use drugs, is considered especially sensitive.[50] The HIV crisis has to some extent brought these groups into the spotlight, with government ministries for the first time recognizing them as vulnerable to HIV infection and particularly marginalized within Tanzanian society. But most rhetoric around “key populations” in Tanzania has focused exclusively on access to HIV services and health care. |
II. Social and Legal Context for Abuses against LGBTI People, Sex Workers, People Who Use Drugs
The three key populations addressed in this report face a similar array of human rights abuses. This section provides an overview of the particular ways in which the law, discriminatory application of the law, and social stigma combine to reinforce the marginalization of each group. The three stories highlighted in text boxes demonstrate how members of marginalized groups are victims of multiple, compounded violations.
Lesbian, Gay, Bisexual, Transgender, and Intersex (LGBTI) People
Tanzania has one of the most stringent anti-homosexuality laws in the world, with penalties in the mainland of 30 years to life in prison for consensual sex between men.[51] The legal provisions that criminalize same-sex conduct are based on a British colonial law, which provided for 14-year prison sentences for “carnal knowledge against the order of nature.”[52] The sentence was revised in 1998 and again in 2002, and is now the second most draconian anti-homosexuality law in East Africa after Uganda’s law, which mandates a life sentence for same-sex conduct.[53] Zanzibar’s law, as noted, does not criminalize just sexual relations, but also undefined “unions” between same-sex partners.
The status of LGBTI people in Tanzania was rarely discussed openly until the last decade, and the initiation of public discussion on the subject has met with backlash. In 2003, about 300 Tanzanians protested a planned visit to Dar es Salaam by a gay tour group from the United States. The visit was subsequently canceled.[54] In 2007, a Tanzanian bishop came under fire for proposing further dialogue about homosexuality in the community and the church.[55] In September 2011, the Gender Festival—an event bringing together gender activists from throughout Africa since 1996 and organized by the Tanzania Gender Networking Programme (TGNP) and the Feminist Activist Network, two Tanzanian NGOs—became a flashpoint for heated debate on sexual rights and whether same-sex conduct was “natural.” Participants who self-identified as LGBTI were chased by media and forced to flee the premises, and then attacked by members of the public.[56] According to one gay participant, “[A] mob had gathered there saying they wanted to kill gays. I was getting into a dala dala [public minibus] and the conductor started to beat me. Then everyone started beating me.” A popular TV anchor rescued him and drove him to the hospital.[57]
The events contributed to heightened backlash from certain media and social networking sites, and the “outing” of MSM participants affected their relationships with families, employers, and landlords. Participants told Human Rights Watch that at least six MSM lost their jobs or were forced to change their residence after the festival, some because they had been seen on television, others simply because the debate provoked by the Gender Festival led to a witch hunt in which suspected gays were publicly accused by family members, neighbors, and employers.[58]
In October 2011, the United Nations Human Rights Council held its Universal Periodic Review (UPR) of Tanzania.[59] During the UPR, Tanzania refused to accept all three recommendations from fellow UN members related to sexual rights: to take steps to protect the rights of all persons irrespective of their sexual orientation, to adopt anti-discrimination legislation, and to decriminalize consensual same-sex conduct.[60]
In November 2011, Tanzanian officials responded critically to comments by British Prime Minister David Cameron to the effect that a country’s record on LGBTI rights would play a role in British foreign aid determination. While donor countries linking human rights to aid is not a new concept, the specific mention of human rights for LGBTI people produced a backlash. A Tanzanian daily newspaper reported Foreign Minister Bernard Membe as saying, “Our position on this matter is crystal clear. Our moral values and culture will always prevail even if we remained poor.”[61] The paper offered its own opinion, arguing that homosexuality is
[A] cardinal sin that smells to high Heaven [which] can only happen in a rabid world where lunatic men and scarlet women have no qualms about flouting the tenets established societal customs or offending Almighty God.[62]
Against this backdrop, arrests, violence, and harassment of LGBTI people are common, particularly for MSM.[63] Examples of discrimination in housing, education and employment have also been reported and affect lesbians and bisexual women as well as gay and bisexual men.[64]
Discrimination against sexual and gender minorities is partly rooted in a misunderstanding of homosexuality as something one “does,” not something one “is.” A representative of a local NGO in Tanga, while emphasizing the importance of providing services to LGBTI people, said being gay is “a business,” conflating male homosexuality with sex work—reflecting a common assumption throughout Tanzania.[65] This belief contributes to homophobia even among those working in fields such public health and human rights: in an interview with Human Rights Watch, the regional manager of a well-respected international public health organization called for “killing the gays” in order to prevent others from “becoming members.”[66]
While discrimination occurs at many levels, one gay man blamed the lack of positive leadership at the highest level of government: “The president doesn’t promote the rights of LGBT people. When he does—one day when he says ‘These people have equal rights’— people will stop abusing us.”[67] Abdalla J., a 32-year-old gay man whose father expelled him from the family home after he attended the 2011 Gender Festival, blamed Tanzania’s anti-homosexuality law: “You should tell the government to decriminalize us. What I do is my personal life. I don’t know who it affects but me.”[68] A gay man in Tanga expressed a simple wish: “I just want the government to treat us like human beings.”[69]
Transgender and Intersex People
LGBTI organizations working in Tanzania were only aware of a few cases of individuals who identify as transgender or who publicly present a non-normative gender expression. Of the three transgender Tanzanians Human Rights Watch and WASO were able to identify and interview in the course of this research, two had experienced human rights abuses at the hands of the police, documented in Section III.[70]
Human Rights Watch interviewed one intersex person in Tanzania (see Glossary). The concept of “intersex” is even less understood in Tanzania than that of being transgender, and it is likely that many intersex people “pass” as one gender identity or the other. However, the many documented cases of discriminatory treatment on the basis of sexual orientation in the Tanzanian health care system suggest intersex people may experience discrimination as well.
No research has been published on HIV among transgender or intersex people in Tanzania. In other countries, stigma against transgender and intersex people has been found to significantly impede prevention and treatment efforts.[71]
SAIDI W.’S STORYSaidi W., a 20-year-old gay university student who sometimes does sex work to support himself, told the following story: In December [2011], I was in a place where I look for clients. I met a client, but [it turned out] it was not a normal person, it was a police officer. We went to a guest house. The client said, “Take off your clothes.” I took off my clothes and suddenly the man pointed a pistol at me. Suddenly the guy had a tape recorder and a video camera. He said “You will be an example for others. I am from CID [Criminal Investigation Department] and I’m looking for people like you.” He took me to Central Police Station and put me in lock-up. The police there told me, “Call your fellow gays. We are going to a bar.” They were asking for gays in general, not just sex workers. They were five police. They gave me their phone and said, “Call your friends, tell them there is a party here, so there are a lot of drinks.” They were threatening to shoot me if I didn’t call my friends. They had SMG [submachine] guns. They cocked the guns at me, saying, “If you don’t call your friends, we’ll shoot you.” We went together to Sun Cillo Club in Sinza. The police put out a lot of drinks. I called five friends. All of them came. Some of them were in skirts, some were wearing make-up. Police came and put them in the Defender [police vehicle]. They said, “We’re arresting you because you’re gays and you’re shaming us. Our country does not allow homosexuals. Our law and our religion and customs don’t allow this.” They beat all of us a lot in the bar. They beat us with our belts. The bar owner and others didn’t help us—they laughed, they were happy that this was happening. The police undressed us and started to beat us with sticks. They beat us everywhere on the body. They took us to the lock-up at Central Police Station. They were calling us mashoga [derogatory term for gay] while beating us—“You are gay, why are you selling your body?” We were in the police station for four days. The other detainees gave us problems. On the fourth day, those guys decided to rape us. They didn’t use condoms. We refused, but they were bigger and older than us and used force. We called to the police and screamed for help, saying, “These guys are forcing us to have sex with them.” But the police said, “That is good, that’s what you want.” So the police were encouraging the guys in there. There were about 50 other detainees, and five of them were raping us. Three of them raped me personally. I got a lot of pain. The following day, the five men were taken to Sitakishari Police Station. A female police officer interrogated them, and seemed sympathetic when they said they had been raped: “She said, ‘Wait until tomorrow, we’ll go to the hospital.’ She gave us her phone to tell us to call a relative to come for bail.” Saidi called his mother, who came in to meet the officer. However, despite the officer’s sympathetic attitude, she wanted her cut: [The officer] wanted money as a bribe to let us free and end the case. The police were asking Tsh 500,000 (about $307) for all five. My mother cried a lot, saying, “I don’t have money.” I said, “Mom, this case is really bad.” My mother managed to get Tsh 400,000 after three more days [from] someone who loans money. After bribing the police, we were released…. It took a long time for my mom to pay that money back. Saidi concluded: “When I remember that situation I want to cry.”[72] |
Sex Work and Commercial Sexual Exploitation
Although sex work is illegal in Tanzania, it takes place openly in many cities and towns, with sex workers gathering at well-known locations. While they are occasionally prosecuted and serve prison sentences, sex workers are often simply beaten or raped by police and then return to the streets, as documented in Section III.
A recent World Bank-funded study describes “addressing violence, stigma and discrimination against sex workers” as “a human rights imperative.”[73] According to the study,
Criminalization enables police to perpetrate abuse and humiliation, demand free sexual services, and extort fines from sex workers with impunity, and renders those who suffer violence and other human rights abuses with little legal recourse…. By driving sex work underground, criminalization is also counterproductive to community mobilization efforts to strengthen sex workers rights and promote autonomy.[74]
These impacts of criminalization are manifest in Tanzania. Sex workers who suffer violence, at the hands of both police and civilians, rarely report the crimes against them. A National AIDS Control Programme study of sex workers in Dar es Salaam found that 33.3 percent reported being beaten by their clients.[75] A representative of an international public health organization in Mwanza explained, “Sex workers do not have a place to speak against injustices done to them, and the police can take advantage of them if they go and report. If they go to the police, the police just become their customers for that night.”[76]
Both adults and children engaged in sex work are regularly forced into sex without condoms, including by police officers. As a sex worker in a small mining village put it: “Some men have knives, and if you want to use a condom, they threaten to kill you. This happened to me here in Itumbi. I decided to have sex without a condom because I was afraid. All the men here carry knives.”[77] In Dar es Salaam, while NACP found high levels of reported condom use among sex workers, it also found that “the high prevalence of sexual and physical abuse by partners indicates that FSWs [female sex workers] may not be able to make protective choices.”[78]
Many sex workers mistrust public hospitals, where they risk being refused service or stigmatized, as seen below. NACP found that while most female sex workers in their study had been tested at least once for HIV, “Access to services and HIV testing were not as routine or frequent as is recommended for members of high-risk groups.”[79]
Sexual Exploitation of Children
A particularly vulnerable group comprises children who are sexually exploited through sex work. Girls engaged in sex work, or otherwise sexually exploited, are significantly more likely to experience sexual, physical, and emotional violence, according to a national study on violence against children in Tanzania.[80]
International law strictly prohibits commercial sexual exploitation of children.[81]Any child who is engaged in sex work or otherwise commercially sexually exploited should not be prosecuted or penalized for having been party to illegal sex work but should be provided all appropriate assistance. The use of children in sex work is punishable by a prison term of up to 20 years under Tanzanian law.[82] However in several cases that Human Rights Watch and WASO documented, police physically and sexually abused children engaged in sex work, rather than protect them. According to the US State Department, no one was prosecuted in Tanzania in 2012 for sexual exploitation of children.[83]
ROSEMARY I.’S STORYRosemary I., an orphan, started sex work when she was 10. When Human Rights Watch interviewed her in Mbeya, she was 14 and had a one-year-old child. She was expelled from school in Form 3 after becoming pregnant.[84] Rosemary sees little opportunity for herself beyond earning money through sex work. Rosemary is a child under international and Tanzanian law, but to the Tanzanian police, she is also a criminal. She is also easy prey for sexual predators within the police force. She has been raped by police “about seven times” by her calculations. She explained, “When they catch you, they don’t send you to the police station. Wherever they meet you, they could take you to the toilets in the club, or if they meet you in the road, they just find a hidden place and have sex with you there. They don’t use condoms—they always refuse.” Refusing sex with police is not an option for most sex workers we interviewed. In December 2010, when Rosemary was 12, she was arrested while working in Tunduma, near the Zambian border. The police asked for sex, and she refused. She told Human Rights Watch, One time I refused and they sent me to [Tunduma] police station. I asked for forgiveness when I reached the station. They were four or five cops. They said, “If you want forgiveness, you have to sleep with us.” So I slept with all of them, because all of them wanted it. After I slept with them all, they let me go. The same month, Rosemary was beaten and raped by another set of police officers, again at Tunduma police station: Once I was beaten on the road and sent to the police station. They were beating me with the thick sticks they carry. They beat me on the head, on the arms. When I arrived at the station, I was in pain and bleeding from the nose. Other police there said, “We have to have sex with you if you want us to release you.” In April 2011, Rosemary was drugged by a client in Mbeya. She later deduced that the client had taken her to a guest house, vaginally and anally raped her while she was unconscious, and left her naked body outside the guest house. According to Rosemary, I woke up in the morning and found myself outside, bleeding from my private parts. People found me and wanted to send me to the hospital, but I refused because I was afraid. How was I going to explain myself? I was also afraid to go to the police because the police might just want money, and I had no money. Also, I couldn’t explain that I was selling myself because then it could be a case against me.[85] |
People Who Use Drugs
Parts of Tanzania, including Dar es Salaam, Zanzibar, and Arusha, have high levels of drug use, especially injection drug use. An estimated 25,000 to 50,000 people inject drugs in Tanzania.[86] Most are injecting heroin, which spread in the 1990s when drug smugglers switched from traditional overland routes from Asia to Europe, opting instead for transport across the Indian Ocean. Zanzibar and Dar es Salaam both became ports of entry.[87]
People who inject drugs (PWID) are particularly vulnerable to HIV/AIDS, largely because of sharing needles. Research suggests that new HIV infections among PWID in Tanzania are increasing. [88]
To address high HIV rates, Médecins du Monde (MdM), an international NGO, is pioneering harm reduction work among people who inject drugs in Temeke, Dar es Salaam’s poorest district. MdM runs a needle and syringe program, and has trained at least 150 police officers in Dar es Salaam on the importance of access to clean needles and syringes.[89] It is also documenting human rights abuses affecting its beneficiaries, and working with police commanders to address the cases systematically. There are no needle and syringe programs in Tanzania outside Dar es Salaam, although they have been considered in Zanzibar.[90]
Tanzanian public health officials have also introduced methadone treatment for heroin users.[91] The methadone clinic at Dar es Salaam’s Muhimbili Hospital, founded in 2011 and funded by PEPFAR, is only the second such clinic in sub-Saharan Africa.[92] A second methadone clinic in Dar es Salaam opened at Mwananyamala Hospital in 2012.
In Zanzibar, the government has begun to recognize that heroin use is widespread, and is not best addressed through punitive measures. The president of Zanzibar has spoken publicly about the need to support people who use drugs and provide them with services; according to members of the Zanzibar Drug Control Commission, the president’s statements have played a positive role in decreasing stigma by introducing non-punitive approaches into the public debate.[93]
Nonetheless, people who use drugs in Tanzania are heavily stigmatized and subjected to abuse. Dozens of those interviewed by Human Rights Watch and WASO spoke of being victims of physical violence at the hands of the police, vigilante groups, and neighbors. A number of them told us that people who use drugs are generally regarded as “thieves,” regardless of whether they have actually stolen anything.
JANUARY H.’s STORYJanuary H. lives in Temeke District and uses heroin. In 2011, he was attacked by members of a mob of Sungu Sungu—a militia group, discussed further below—who accused him of robbery. They dragged him to a nearby schoolyard, where they cut him on the head and face with pangas [machetes]. January extracted himself from the mob and ran to the Mashini ya Maji police post, where he lost consciousness. When he came to, he said, I heard the police saying [to the Sungu Sungu], “Why didn’t you kill him? Why did you bring him here?” Then a senior police officer asked “Who did he steal from?” and nobody answered. The police took me to another police station, Mtongani. They asked who the complainant was and what the R.B. [Reporting Book] number was, but there was none. When no one complained, the Mtongani police called the Chang’ombe police. They came… and took me to the hospital. January thought his travails were over, but the health workers at Temeke District Hospital who treated him only made things worse. He recounted: The doctor examined me, wrote things down, and sent me for stitches in Ward 10. There they started sewing me up without any injection [anesthesia]. I asked for it, and the nurse said, “We don’t need to. We are going to sew you without. We could inject you with poison rather than with anesthesia.” I heard them [hospital staff] saying, “That one is a thief.” So they stitched me everywhere without anesthesia. When January was discharged, he considered filing a complaint with the police against his attackers, but had second thoughts: “[For] many of us youth who use drugs, the police create obstacles to us opening cases. They might keep telling you to wait. And then later they’ll make up a fraud [fraudulent] case against you and take you to prison.” He added, with regard to the Sungu Sungu, “I know the reality is one day they’ll kill me.” [94] |
III. Police Violence, Intimidation, and Extortion
Violence, prejudice, and extortion by police contribute to severe mistrust between key populations and state institutions. For many Tanzanians, police are the face of the Tanzanian state that they encounter most regularly. For key populations, these interactions are anything but positive. Human Rights Watch and WASO documented cases of violent assault by the police against all three groups that are the focus of this report: LGBTI people, people who use drugs, and sex workers. Police also targeted children who were victims of commercial sexual exploitation. Of those who had not experienced assault, nearly everyone had experienced extortion for money, sexual favors, or both.
Among all three key populations, our research suggests that those who are the most vulnerable to police abuse are from lower socioeconomic classes. Men who have sex with men, people who use drugs, and sex workers from secure economic backgrounds often manage to avoid the police. A heroin user from a middle-class family told Human Rights Watch he was never caught by police because he used drugs in the privacy of his own home.[95] Similarly, a group of sex workers in Arusha said that because they were working in an enclosed bar frequented by a middle-class clientele, they were relatively protected from police harassment, whereas their colleagues who worked the streets were more frequently arrested and beaten.[96] While police abuse of male sex workers is common, Human Rights Watch and WASO heard of no cases in which their clients, generally well-off men, were arrested or ill-treated by police. Wealthier individuals’ ability to pay bribes also helped them, in some cases, to escape detention and violence.
Marginalized groups are not the only ones who suffer violence and abuse at the hands of the Tanzanian police. The Legal and Human Rights Centre (LHRC), an NGO, reports that the Tanzanian police extra-judicially executed at least 11 people in 2012.[97] LHRC cited a culture of impunity and the lack of an external, independent oversight body as explanations for high levels of police violence against civilians.[98]
Police corruption is also a widespread problem in Tanzania.[99] According to a representative of a foreign aid agency that works with the Tanzanian police, “Police are worse on corruption than other institutions. They may also be the worst institution on human rights.”[100] Tanzanian police regularly shake down civilians for bribes. This may include for instance, drivers, whether they do or do not break the law; victims of crime, who are seeking police assistance and are told it only comes at a price; refugees or asylum seekers who are caught without proper documentation; or people involved in unlawful sexual conduct or drug consumption.[101] Police know that the latter group is an easy target, as members of marginalized groups are less likely to file complaints.
Some efforts have been undertaken to combat police corruption. Police told Human Rights Watch that 47 officers were dismissed due to corruption in the first half of 2012.[102] However, vulnerable groups are particularly unlikely to report corrupt or violent police, as the stories below demonstrate.
Torture and Ill-Treatment
Human Rights Watch and WASO interviewed dozens of members of key populations that had been tortured, raped, ill-treated, or coerced into paying bribes by police in the last several years. In none of these cases were police held accountable for the abuses.
In Temeke, a Dar es Salaam district with high levels of drug use, victims frequently referred to a police officer nicknamed “Tyson,” based at Chang’ombe Police Station, who by all accounts seemed to draw sadistic pleasure from assaulting and humiliating people who use drugs. In one such case, Suleiman R. was arrested on December 31, 2011, and taken to Chang’ombe Police Station. There had been three robberies the previous week, and since Suleiman was known to inject drugs, police suspected him. He said,
They took me to a special room to torture me and get me to confess to the cases…. First they hit me with iron bars on the right arm. Then they took a clothes iron and ironed me on the arm. They ironed me two times. One of them was Tyson, who is also known as Adnan.[103]
Human Rights Watch saw burn marks on Suleiman’s arm consistent with those that might be left by an iron. The following day, Suleiman’s parents paid a bribe of Tsh 200,000 (about $123) in order to have him released.
Zeitoun Y. was arrested in January 2009 just after smoking heroin in his maskani.[104] He tried to run away; when police caught him, he said, “I was tied around the neck with a rope. I was dragged about 200 meters. Tyson put the rope on me and dragged me personally.” Zeitoun was taken to Chang’ombe Police Station, where he said police beat him and tried to make him confess to a robbery.[105]
Mwajuma P. reported that in 2011, Tyson beat and humiliated a group of women who use drugs:
He came to a maskani with two other police, rounded us up, and forced us to pray…. He told us to put our hands on our heads. Then he made us walk to the police and sing songs: “Us, we are drug users. Us, we steal phones.” Tyson started treating us like cows, beating us with a five-foot long heavy plastic pipe. He came with it. He beat me on the back, on the legs.[106]
Tyson forced the women to walk more than four kilometers in the hot, midday sun, according to Mwajuma. At Chang’ombe station, police took their statements. Mwajuma was released without charge after two days, when her sister-in-law paid Tsh 20,000 (about $12).
Ally H., who uses heroin, said that police from Chang’ombe beat him and his wife in August 2012:
The police came from Chang’ombe at about 8 p.m. They kicked in the door by force. They came in and started to beat me and my wife.... They were suspecting us of being drug sellers. They didn’t have any warrant. They were about seven police.
I was beaten with a rungu [club] on the knees and forearms and back. I still have pain on my knees. They hit me on the back with a stick that was like a thick branch. [107]
At the station, Ally said, an investigating officer ordered him to lie down on the floor, and different police beat him. Even after Ally paid a bribe of Tsh 40,000, he said, police “continued beating us with sticks while chasing us out of the police station. It was afternoon, and all the other police officers saw.” [108] Approximately a month after his release, a Human Rights Watch researcher observed bruises on Ally’s back that were consistent with being beaten by sticks.
Several victims also cited police from Dar es Salaam’s Oysterbay Police Station as being responsible for assault, sexual exploitation, and extortion. Fazila Y. said police from Oysterbay Police Station beat her in the middle of the street when she was caught in the maskani in October 2011 using drugs with friends:
Passers-by and shopkeepers looked on as the police kicked me, verbally assaulted me, and tore my clothes. After they were satisfied that I was hurt to their liking, they dragged me into the back of the police car. [109]
Asked whether she considered filing a complaint against the officers who beat her, Fazila said, “I do not see the point of complaining about treatment that we receive from police. What will change? Who will listen?” [110]
A police sergeant arrested and beat Mickdad J., in Tandika, Dar es Salaam, in June 2012 because he was carrying unused syringes from Médecins du Monde’s (MdM) harm reduction program:
I was coming from MdM with syringes, yellow boxes [for disposal of sharps], things that I use to inject. I was outside my home arranging these things. The sergeant saw me, stopped and arrested me. I wanted to call MdM, but [the sergeant] took me to Mamboleyo Police Post. There, he beat me with his hands, a stick, and also with his police boots.[111]
Mickdad’s mother came to the police post and paid Tsh 30,000 (about $18) to have him released, but the experience had a lasting impact due to his fragile health, Mickdad said, “Even now I have pain in my spinal cord and my coordination is not good. I am HIV positive, so when people beat me it’s a problem.”[112]
One particularly horrific case of alleged police abuse involved John Elias (his real name), a heroin user in the Kigamboni area of Dar es Salaam. On February 18, 2010, he was arrested in a drug bust in Kurasini neighborhood. According to Elias, one of the police officers involved in the arrest had a personal problem with him: the officer believed Elias was having an affair with his girlfriend. The officer seemingly used the drug bust, and Elias’s vulnerable status, as an opportunity to get revenge.
Elias told Human Rights Watch that police burst into the house at 4 p.m. and said they were conducting an operation to look for drugs:
They looked but found nothing. They arrested three of us. I was arrested by a policeman called James who suspected me of walking with his girlfriend. He knew me from before. He suspected me of using drugs, but also walking with his woman. The other two were arrested because they were drug users. [113]
All three men were taken to Kilwa Road police station. Police began taking statements from Elias’s friends, but Elias said the Officer Commanding District (OCD)—the superior of James and other officers present—ordered that he be taken to a different police post.
I was put inside a car with chains on my hands and feet. They didn’t say why. James said, “We’re sending you to Chang’ombe to break your leg.” But they were lying—they took me to Minazini post.
They put chains on my arms and legs and pushed me down. I saw a syringe with liquid inside. James was holding it. He said, “Today is your last day to see, Mr. John.” First he injected my right eye, and then the left one. I was lying on the ground. About five police were there. They were grabbing me, holding me, stepping on me with boots…. I felt like my eyes were burning. It was so hot. [114]
At around 7 p.m., Elias said, the police returned him to Kilwa Rd Police Station and put him in lockup with his friends. Police took him directly to court in the morning. Although he told court officials what the police had done to him, he was taken directly to prison and was not taken to the hospital until a week later. [115] There, he discovered that the police had injected his eyes with acid.
Today, Elias has gaping holes where his eyes should be.
The Nyerere Centre for Human Rights, a local NGO based in Temeke district, has been following the case since 2010. Edward Nsajigwa of the Nyerere Centre told Human Rights Watch, “He went to open a case at the police station, but they wouldn’t help him.… He went to the general secretary at the Ministry of Home Affairs, but the general secretary said his eyes were busted out by mob justice.”[116] The Commission on Human Rights and Good Governance (CHRAGG), Tanzania’s national human rights institution, has visited Elias’s home to investigate the case. In April 2013, a CHRAGG official told Human Rights Watch the file is still under investigation at CHRAGG, without providing further detail.[117]
Police torture and ill-treatment of people who use drugs is not limited to Dar es Salaam. In Mbeya, Musa E., a teenager who has been orphaned since he was eight and who used to use heroin, says he agreed to transport a sack of heroin across the border from Zambia to support his habit. Tanzanian police arrested him at the border town of Tunduma and tortured him in order to find out for whom he was working. Musa said the police squeezed his fingernails and toenails with pliers; elbowed him in the jaw, causing his mouth to ooze pus for a month from the resultant infection; and stepped on his ankles in boots, until he provided his employer’s name. [118]
In Zanzibar, former drug users told Human Rights Watch that most of their complaints were with police jamii (see Section IV below). Local organizations have organized trainings and dialogues to sensitize the regular police about the importance of treatment rather than punishment. These have been largely successful. But some cases of police ill-treatment linger. Police caught Omary Q. in possession of heroin in his neighborhood in late 2011. Omary said,
They grabbed my neck and punched me in the lungs and kicked me so that I fell down. Then they handcuffed me and took me to the station. They asked me, “How much can you pay [to be released]?” I said, “I don’t have any money, but if we go to a place I can get some.” I left with two of them. We went to my brother’s. My brother bribed them with Tsh 50,000 ($35) and they freed me.
You can’t go to the police and make a complaint if you’re abused by them. We can’t trust them. They’ll accuse us of being against the law.[119]
One former heroin user told Human Rights Watch of the humiliation he suffered in police custody in Zanzibar:
One time I was in custody and had withdrawal symptoms – diarrhea, vomiting. The police didn’t care; they left me in the room [cell]. I was crying, “Take me to the toilet!” They would let me go to the toilet once a night only. So I would have to just shit in the cell. [120]
Several women interviewed in a drug treatment center in Zanzibar said they had also been beaten by police. Sharifa Z. was beaten in police custody at Ngambo police post in 2011, apparently as punishment for vomiting as part of her withdrawal symptoms: “I was puking because of withdrawal, so they were upset and they hit me a bit.” [121] Police beat Suhayla F., a pregnant 23-year-old woman, in mid-2012 for using heroin. Suhayla recalled, “One of the police said to the other ‘She’s pregnant, don’t hit her,’ but the other hit me on the back.” [122]
Men who have sex with men are also subjected to violence by the police, especially in Dar es Salaam, where they tend to be slightly more open and thus identifiable. Saidi A., whose story is recounted in Section II, above, was threatened by police at gunpoint and forced to call his gay friends. Police beat them with belts, stripped them naked, and mocked them as they were repeatedly raped in police custody.
Collins A., a gay man in Tandika, was arrested and beaten for attempting to organize a seminar on health issues for men who have sex with men, which he hoped would be the first step toward establishing a local MSM association in his neighborhood:
I asked the warden of Tandika for permission to have a seminar. We were open, asking to have a seminar for MSM. The warden called the police. The police came and arrested me at the warden’s office…. They slapped my face and took me to the police cell. They detained me for two days at Changombe police station. They told me, “We’re arresting you because you’re same-sex.” They didn’t tell me my rights. They insulted me while questioning me, said, “We don’t need you people, we don’t need you to survive, that’s why we’re fighting against you.” They tore my clothes. They beat my legs with a baton. I had trouble walking afterwards.[123]
A friend brought Tsh 12,000 (about $7) to bribe the police to release Collins. When he sought medical treatment after the beating, Collins confronted another obstacle:
I went to the hospital afterwards because I was in pain from the beating. But the hospital said I had to get a PF3. I went to the station to ask, and the police refused to give it to me. So I had to bribe the doctor in order to get treated…. I gave up on the idea of forming an association.[124]
In Arusha, Lester F., an 18-year-old gay man, recounted his arrest in October 2012. He had made the mistake of dating a married man, whose wife discovered the affair:
We were in a bar. His wife came to the bar with her brother, who was a policeman, and caught us. He called other policemen, and about four came, and arrested me.
They beat me all the way from the bar to the car to the police station. They beat me with clubs and with belts. They even told me they might shoot me. Where they beat me, I had hand marks on my face, and marks from the belt on my arms. I cried a lot.[125]
Police took Lester to the station, where, in the lobby, other police asked why he had been arrested. When they were informed that Lester was gay, he recalled, “Then all the police started beating me. Every police who was there was beating me. Some insulted me. Some pushed me.”[126] Lester F. was freed after he telephoned a soldier, whom he described to Human Rights Watch and WASO as a boyfriend, who came to the station to intervene.
Mariam H., a sex worker, said police in Dar es Salaam’s Kinondoni district detained and beat her in early 2012 after catching her on the street. She paid a Tsh 30,000 ($about 18) bribe to be released. Several days later, she decided to report the beating at the local police station:
I tried to go and report them. It was two days after, when I felt strong enough to leave the house. The police lied and said that I had been beaten by the people [civilians]. They mentioned that it might be because I am a thief as well as a sex worker. They had physically hurt me, and nowhere is it legal for policemen to physically abuse “criminals.”[127]
Sexual Assault and Sexual Extortion by Police
One specific form of violence that police inflicted on key populations is sexual violence, which can be a form of torture or cruel, inhuman, and degrading treatment.
Walid A., a 19-year-old MSM in Zanzibar who occasionally does sex work, was raped by police and police jamii on his way home from a club in 2011. He said,
They have water pipes and electrical wires. They beat me with those. They forced me to have sex with them. Five or six of them came [to arrest me], and two of them raped me…. They had canes and pipes, and they hit me on the bottoms of the feet. I couldn’t walk afterwards. I didn’t go to the hospital afterwards because they harass you there.[128]
Human Rights Watch observed scars on Walid’s legs that were consistent with having been beaten with electrical cable.
Alex N., a transgender man, was sexually assaulted by the police at Buguruni Police Station in Dar es Salaam in 2009. He was 18 at the time. The manager at the bar where he worked, who accused him of being a lesbian and having a “bad attitude,” turned him in to the police. When Alex arrived at the police station, he said, police told him to take off his clothes and touched his breasts and vagina. They beat him on his arms and back with a belt and then forced him to wear women’s clothing and clean the police station. He was released after six days, and said, “I did not make a complaint. I was afraid.”[129]
Jessie L., a transgender woman and sex worker in Dar es Salaam who is biologically male but passes as a woman, said she had been arrested for sex work more than 10 times. On at least one occasion, police sexually assaulted her:
I normally tell them the truth. So the police get shocked. “You are a gay? No, you are a woman.” So they don’t beat me. They take me to the special room and check me. They have me stay in a special room with neither men nor women. They call everyone to come and look at me—male and female police officers. They call each other, “Come, come! Look at this gay!” And they ask me more questions. “How did you start to have anal sex? How do you feel when you are penetrated?” They normally force me to take off my clothes and I don’t have an option, so I agree with them.
The police never forced me to have sex with them to be released. But they did touch me, joking about me and squeezing my fake breasts. They said “Show us an example of when you handle your partner, when you have sex, how does it look.” I refused. But they were touching me, “Are you really a woman?” They touched me everywhere. They asked “Do you have a vagina?” and touched my genitals.[130]
Of the 66 people we interviewed who were or had previously been engaged in sex work – men, women, and children – at least 23 said the police had forced them into sex. Five such victims were children. Women who use drugs also reported being forced into sex with police in exchange for release from custody. Some police refuse to use condoms, making the police possible conduits for transmission of HIV and other STIs. All acts of forced non-consensual sex constitute rape.
Halima Y. was gang-raped by eight police officers in March 2013. She explained,
I have had sex with policemen so many times I cannot even remember how many. He catches me, he wants money, but I do not have money so he will force me to have sex with him…. On Easter [2013], three policemen arrested me and wanted money. I did not have any money. I bribed them with sex. Then, three others policemen came. I also bribed them with sex. Again, two others policemen came, and I gave them sex. I was sick… I got a UTI [urinary tract infection] and I even got gonorrhea. I am now on medication.[131]
Amanda Z., a female sex worker in Dar es Salaam, said police had forced her to have sex on two occasions without condoms, most recently in early 2013:
[In both cases], they would not use a condom and I did not tell them [to do so] because I just wanted to get released and get home to my kids. If I have to have unsafe sex in exchange for my release then I do it and go.[132]
Ramazani H., a 22-year-old male sex worker in Dar es Salaam, has been arrested in the streets at least four times. The first two times, police beat him with sticks and asked him for bribes. The third time, he said,
Two police arrested me in Kariakoo. They beat me again and took me to the police station. I spent one night there. They forced me to have sex [with them], but I refused, so they said “If you refuse, just suck our dicks.” So I sucked their dicks outside of the police station.
Ramazani still had to pay Tsh 30,000 (about $18) in order to be released.[133]
Wilson N., a former sex worker in Dar es Salaam, said that on two occasions, in 2009 and 2011, police arrested him while he was doing sex work and forced him to have sex with them. The first time, two police officers took him to Keko Police Post and insisted on sex without condoms, then made him spend the night in jail. On the second occasion, Wilson recalled:
I passed near Tandika Police Post and the police officer called to me. I was wearing women’s clothes. He said “You are loitering and looking for clients. If you want me to leave you free, you have to have sex with me.” I decided to have sex with him. He used a condom and oil-based lubricant. He wanted to do it fast because he was afraid of other police officers coming.... We did it in the toilet of the police post.[134]
Police Rape and Assault of Children
Some of the most troubling cases of police abuses against members of key populations involve children, particularly children engaged in sex work. Police rape, sexually assault, and beat children engaged in sex work with impunity. Sexual abuse of children is a serious crime in Tanzania, for which police should be investigated and prosecuted. Children engaged in sex work should never themselves be arrested and prosecuted for engaging in sex work, but should be provided with the appropriate assistance.
As recounted in Section I, multiple police officers in Tunduma raped Rosemary I. on two different occasions when she was 12. Three police officers raped another girl involved in sex work, Alamisi V., after arresting her at Magorofani truck stop in Mbeya during Easter 2011. She was 14 years old.[135]
In July 2012, two police in Mbeya detained Jenifer A., a 16-year-old girl engaged in sex work. They took her to CCM Police Station, raped her on the ground outside the station, and then beat and kicked her while she lay on the ground. She said that while beating her, “They told me I should not be going to the bars to have sex.”[136]
Sex with police does not necessarily protect against arrest. Khadija J., a 16-year-old in Mbeya, has been raped by police at least eight times in the year-and-a-half that she has been doing sex work. On two occasions, police officers took her home and forced her to spend the night with them. But, she said, “Both times they had sex with me but then sent me to Central Police Station in the morning. Then I just had to wait until I could call my friends and they paid money to release me. They had to give Tsh 30,000 or 40,000.” [137]
On another occasion, Khadija tried to refuse a policeman who insisted on having sex with her, but to no avail: “After he punched me in the eye and slapped me, I had to agree.”[138]
Because of their illegal status, both children and adults are forced into sex with police officers even when they are not caught while working, especially in smaller towns where sex workers become easily known. Adimu S., a 16-year-old in Mbeya, explained, “Sometimes, the first time they catch you, they have sex with you or you give them money. Then they mark you, and use you again for sex, even if they don’t catch you doing sex work. They threaten to take you to the station.” [139] This possible exposure explains why children engaged in commercial sexual exploitation, as well as adult sex workers, might be reluctant to file complaints with the police, even when the perpetrators are civilians (discussed further in Section VI): they will be “marked,” and will risk becoming victims of exploitation in the future.
In addition to sexual abuse, police also inflict physical abuse in children. Rosemary I. said that when she was 13 years old, a police officer burned her on the arm with a lighter, while asking her, “Why are you selling yourself?”[140]
Ruby C., a 17-year-old girl engaged in sex work in Mwanza, told Human Rights Watch and WASO in October 2012 that the previous week police beat her outside Mwanza’s Villa Hotel:
There were three police officers that were accusing me of selling myself. The police forced me to kneel down and they started to beat me. They kicked me with their boots. They beat me on the back with the club that they normally carry. I was in pain—I swelled up. I didn’t go to the hospital after I got out because I didn’t have money. I didn’t go to report it because I was afraid that the police would beat me again.[141]
Another street child engaged in sex work, Bishara A., age 16, said three police officers stopped her in the street and beat her in Mwanza in 2011:
The police asked, “What are you doing?” because it was late. I told them, “I sleep here.” They started accusing me of being a sex worker, and beat me. They took me to Kati Police Station. At the police station they beat me with a rubber tube from a car tire. They told me to lie down and they beat me on the buttocks.
The police insisted on a bribe of Tsh 30,000 (about $18) to free Bishara, which she could not pay. After two days, the officer in charge, a woman, ordered her release.[142]
Extortion of Money
When police do not demand sex from at-risk populations, they often demand money. Harun Z., a man in Temeke who uses heroin, spoke of extortion by the police as a regular aspect of daily life:
It’s happened to me a lot: in small police posts, Kilimahewa, Vianiza, Tandika. They ask for an amount depending on how well-off your appearance is. If you look well-off they ask for Tsh 50,000. If not, they ask for Tsh 10,000 or 20,000 or 30,000.[143]
Ilham K., a sex worker in Dar es Salaam, went to a guest house in 2011 with a client, who refused to use a condom. When she insisted, he began violently pushing her around. Ilham called for help, and staff from the guest house came to the room. The client then claimed she had robbed him, and took her to Oysterbay Police Station. The police officers were sympathetic to her story, but still held her in custody and insisted on a bribe: according to Ilham, when her sister came to the station in the morning, “The police told her, ‘We know your sister hasn’t done anything, but this man insists, so we’ll wait for this man to go and then you and your sister can go, but you have to pay Tsh 20,000.’ (about $12).”[144]
Evelyn D. was arrested in late 2011 while preparing to inject heroin. She said, “In the police station I was subjected to a lot of harsh words from the police, especially because I was a woman. They said things like, ‘You are a stupid woman. You are a whore!’” Evelyn was released the same night after her boyfriend brought Tsh 20,000 for the police.[145]
Edwin J., an MSM, had to pay a bribe of Tsh 30,000 (about $18) to officers from Kongwe Police Post in Dar es Salaam in January 2012, after a guest house attendant called the police to report that there were “homosexuals” in a room.[146]
Extortion of money, like sexual extortion, can take place even when members of key populations are not involved in any illegal activity. Henry O., a Mwanza man who uses drugs, explained: “They know me very well, these policemen, and I have become someone for them to get money from. I usually give them around Tsh 10,000-20,000 depending on the day. Sometimes they beat me up, sometimes they don’t.”[147]
Extortion is not only a crime in itself. It leads to a breakdown of trust between members of key populations and the security forces. For Ilham K., a sex worker in Dar es Salaam:
The police’s problem is money. They just want money and know that sex workers have got money. So there’s no friendship there. If there were, we would ask them for help and go to the police when we’re wronged. But we fear them and run away from them.[148]
Arbitrary Arrests
Sex workers, LGBTI people, and people who use drugs all reported that the Tanzanian police had arbitrarily arrested them. The United Nations Working Group on Arbitrary Detention has ruled that arrests made on the basis of same-sex activity are, by definition, arbitrary.[149] When police arrest people for sex work or drug use, many cases are also clearly arbitrary, taking place in the absence of any evidence of criminal activity. Some such arrests also involve police extorting money or sex from victims.
Mohammed R. and his friend were arrested in Dar es Salaam and held in police custody for “walking like women”:
One time I was in the market buying things with a friend, and then suddenly people started shouting because my friend was very homosexual-looking. So we ran to the shop of one woman. [But] she called the police, and they arrested us and took us to Buguruni Police Station. We asked the police why we were arrested, but the police were just harsh and ignorant. They locked us up and told us that our crime was walking like women. The police beat me after I tried to argue and defend myself, saying I was not involved in any crime.
In the morning, a policeman suggested Mohammed provide money or sex in exchange for freedom. Mohammed refused to have sex with the officer, but paid Tsh 30,000 and was released.[150]
Victor G., a 24-year-old gay man in Dar es Salaam, said he had been detained twice because of his sexual orientation:
The first time was in 2009. I was with three people, all gay. We went to the student hostel to visit a friend. We had a disagreement with the owner of the hostel, who didn’t want to let us in. He called the police and reported us as gays. They came and put handcuffs on us. [The owner] just told them we were gay, he didn’t accuse us of any other crime. A policewoman at the station felt something for us, because we were young and had college IDs. We got out without paying a bribe.
Another time, Victor said, police picked up Victor and his friends in the street when they were returning home from a bar at 11:30 p.m. and took them to Magomeni Sub-Central Police Station. According to Victor, “They accused us of ‘disorderly conduct’ just because we were gay. We spent the night at the station. My aunt came the next morning and bribed them with Tsh 150,000 to get me out.”[151]
Joseph S. was arrested for kissing his partner in the street while walking home from a bar in 2010. Police forced Joseph and his partner into a police car. While in the car,
They were beating us, kicking. They said they would take pictures of us and we were afraid that they could put us on the front page of the newspapers. But they didn’t take pictures. They were insulting us, calling us “bitches.” [152]
Police compelled Joseph and his partner to pay a Tsh 10,000 bribe to be released.
Hussein M. was turned in to the police by his family at the age of 16, in 2007, when they found out he was gay. His uncle beat him and then took him to Minazini Police Station in Dar es Salaam. Hussein is not sure what his uncle told the police, but after being detained for two days without being questioned, he was released. When he went home, his parents said they would no longer pay for his school fees as punishment for his homosexuality, so Hussein, in turn, went to the police to report his parents for neglect.
The police summoned Hussein’s parents, but it was his uncle who came in to discuss the case. According to Hussein,
This time my uncle told [the police officer], “This guy is having sex with other men.” Then the policeman started to support my uncle. The police started complaining, “Why don’t you stop doing this?” He gave me five strokes with a stick on the thighs. Then he released me and told my uncle, “Go with him and check on him for two days. If he continues having sex with men, return him back to police station again.”
Hussein went home, but his family chased him away after a week. He said, “Up to today I stay with friends, and my parents refuse to pay for school fees because I’m gay.”[153]
Police in Zanzibar detained Hamisi K. in 2009 and attempted to subject him to an anal examination to “prove” he had sex with men. Hamisi recounted:
We were having a party. The police got information and came. They said men were getting married… They thought it was a wedding, but it was just a party. They even took us to the Mnazi Mmoja hospital to “test” us for anal sex, to do an anal exam. But the doctor refused to test us.[154]
Hayat E. is an intersex person in Dar es Salaam who identifies as a woman. She has dated both men and women, but on several occasions has been subjected to violence by male partners after they realize that she has both male and female sexual organs. Unfortunately, when she attempted a relationship with a woman, it resulted in her being arbitrarily detained:
In March [2012], I was living with a woman. I moved her into my rented room and we were happy together. The local government representative found out that I was living with someone, a female, and they got very upset. The local representative went to the police station to report me. Shockingly, the police took the matter very seriously. They asked me to pay a bribe of Tsh 350,000 (about $214) in order to let the case go. Also the police wanted me to show them my naked body so they could see how I looked.
This was very disturbing to me, and I decided to vacate the room I was renting. Since then, I have decided not to try and live with anyone else.[155]
Mwajuma P., a woman who injects heroin, was arrested for possession of unused syringes. She was assisted by harm reduction and human rights organizations in Temeke:
[I was arrested by] Sungu Sungu and police mixed together, about six months ago. They caught me with syringes at home. They knocked and I opened. They didn’t have a search warrant. They came in and found five boxes of syringes. The Sungu Sungu beat me with the palms of their hands, just because they found me with those boxes. They took me to the police. I sent information to MdM. MdM sent the Nyerere [Human Rights] Centre to bail me out, and the case ended there.[156]
IV. Police Jamii, Sungu Sungu, and Other Vigilante Groups
Tanzania has several community policing organizations and vigilante groups, with varying degrees of formality. While the intent of Tanzanian law enforcement officials in collaborating with vigilante groups is to work with communities to stem crime, members of such groups, like the police themselves, at times use physical and sexual violence and extortion against people who are suspected of engaging in criminal activity.
Some of these groups are legally established and have official communication channels with state law enforcement agencies. [157] One such grouping is the “community police,” also known as “police jamii” or “polisi jamii” in Kiswahili. Through an official community policing program, squads patrol their neighborhoods and provide daily reports to the official Tanzania police. In some parts of Tanzania, residents lauded their work. However, the police jamii were reported to be responsible for a large number of human rights violations in Zanzibar. [158]
Sungu Sungu
The most problematic group is the “Sungu Sungu.” “Sungu Sungu” initially referred to a vigilante group formed to combat cattle rustling in western Tanzania in the 1980s, which then transferred its energy to fighting “witchcraft,” an early indication of the group’s dangerous potential to serve as a form of moral police.[159] In more recent years, the term has come to be used to describe any neighborhood militia.
In theory, Sungu Sungu operate under the guidance of the local government and the police, but in some areas they appear to operate on their own. The People’s Militia Act of 1973, amended in 1989 to make specific reference to the Sungu Sungu, grants them the power to make arrests.[160] According to a US State Department report, “Sungu Sungu members are not permitted to carry firearms or machetes, but they carry sticks or clubs.”[161] But Human Rights Watch research found that Sungu Sungu are often armed with machetes.
Some officials in Dar es Salaam deny that Sungu Sungu even exist. [162] The residents of Temeke, Dar es Salaam’s poorest district, know otherwise. In poor, peripheral neighborhoods, Sungu Sungu members—who are unpaid, untrained, and, according to residents, often have criminal records—patrol the streets at night with machetes (pangas) and clubs (rungus), a walking recipe for human rights violations. [163] In addition to policing actual crimes, they sometimes take on the role of moral police, targeting sex workers and people who use drugs, in particular.
Temeke residents say that Sungu Sungu members killed 34-year-old Abdallah Yunus (his real name), known as “Dula,” and another man, also named Abdallah, in April 2012. According to neighbors, Dula and Abdallah both used heroin. Dula was staying in Abdallah’s house. A woman that stayed in the same house recalled being awakened in the middle of the night by a crowd:
They were saying “Thief! Thief!” They were banging on doors, asking “Where is Dula?”… I don’t know if they wanted both Abdallahs or one of them. I knew they were Sungu Sungu because they were more than 50, and there aren’t other guys like that. People didn’t take any action to stop them.[164]
Another witness saw Dula being beaten by people armed with stones, pangas, and concrete blocks. He explained,
There are Sungu Sungu from two areas. The Sungu Sungu from this area went and said, “Why are you abusing these people?” The others were 50 [people], while the ones from this area were just 7 or 8. I know they are Sungu Sungu because they often patrol, in groups of 40 to 50. They patrol every night.
They were coming with two people. They dumped one person there. Both were alive, but one had already been beaten. He fell. He had been beaten with stones, and he died. I didn’t see the beating, because they had come from around the corner. The second one ran…. They chased him, caught him, and beat him with stones, sticks and pangas.
Then they stopped a motorcycle…. they surrounded it, with pangas. They opened the pipe from the tank and put fuel into a water bottle. They put tires on the two men’s chests. And then they poured the fuel and burned the two people. They already seemed dead at this point.
The witness said police came around 3 a.m.:
They had one person inside the car who they had arrested [in another case]. They told him to put the bodies in the car. I don’t know which police station they came from. The police must have been informed about what happened…. They didn’t come back to do investigations. They didn’t ask residents about it. [165]
According to Dula’s mother:
After three days the family went to ask at Chang’ombe Police Station about investigations, but the investigating officer refused to receive us. He said, “You say it was Sungu Sungu, but if it was banditry, how would you know?” Dula’s brother asked, “If it was bandits, why are you not arresting them?” The police said, “You are bothering us”…. When we failed to get aid from the police, we lost hope.[166]
Although the Sungu Sungu were reportedly shouting, “Thief! Thief!” while abducting Dula, his mother did not know of any particular case in which Dula was accused of theft:
I don’t understand why they killed him. I have never gotten information that he stole anything. Both Abdallah and Dula were using drugs. Dula was calm, he didn’t fight with people; maybe just drugs was the problem.[167]
In December 2012, Human Rights Watch received information from Médecins du Monde outreach workers that a man known as Maliki, was killed by Sungu Sungu in Temeke. According to MdM staff members, witnesses saw Sungu Sungu abduct Maliki from the maskani where he was using drugs and cut him to death with pangas.[168]
Rashid E. was arrested by Sungu Sungu in Temeke who passed by while he was sitting outside in his neighborhood, eating chips, around December 2011:
I think they knew I use drugs because they’re from my area. They just came and grabbed me and started beating me. They beat me with pangas, iron window bars, and sticks. I have a finger that doesn’t straighten ever since. They beat me on the hand with iron bars until it was swollen and black.
The Sungu Sungu took Rashid to Vyaniza Police Post, where police accused him of being a thief. The next day, a friend came to pay a bribe of Tsh 7,000 and Rashid was released.[169]
Sungu Sungu members raped Mwanahamisi K. in May 2012 near the same maskani where Human Rights Watch interviewed her:
I had come here to smoke [heroin]. I was going home when I met with Sungu Sungu at the railroad. It was midnight or 1 a.m. They asked, “Where are you coming from, and where are you going?” I told them, but they wouldn’t understand. They had pangas. I screamed but no one helped me. It was night, so no one passed by.
Six of them forced me to have sex with them. All six of them raped me and left me there. They didn’t use condoms. The rape lasted one or two hours. I was with my child. The baby boy was lying on the ground to the side while I was being raped…. After raping me, they told me “Don’t move around at night.” [170]
In the morning, Mwanahamisi went to Mashini ya Maji Police Post to file a complaint, but police refused to help her unless she paid them Tsh 10,000, so she went home.[171]
Sex workers in Dar es Salaam also reported that the Sungu Sungu committed physical and sexual violence against them. One sex worker in Kinondoni District said, “We are forced to hide from them. When they know that someone is a sex worker, they beat them.”[172] According to another female sex worker,
The Sungu Sungu in the area I live are harsh. When they see you coming back from work or working in the middle of the night, they force you to join them while they make their rounds. The only problem with this is they then feel it is their right to touch you when they feel like.[173]
The presence of Sungu Sungu was also reported in Mbeya and Arusha. In Mbeya, three sex workers told Human Rights Watch they had been beaten by Sungu Sungu.[174] In Arusha, a community activist working to rehabilitate people who use drugs said that Sungu Sungu uses preemptive violence: “At night, they go around. If they meet the users, they beat them, because they think they will steal something.”[175]
Police Jamii
As noted above, the police jamii are part of formal community policing programs. Some Tanzanians spoke somewhat favorably of the police jamii. In Mwanza, for instance, a representative of a local NGO told Human Rights Watch and WASO that the police jamii were assisting NGOs in their work with street children; they would turn children over to NGOs that can assist them.[176]
In Zanzibar, however, police jamii were frequently and virulently condemned. An outreach worker at a drug rehabilitation center told Human Rights Watch that police jamii—who he said usually traveled in groups that include one regular police officer—posed a challenge to outreach:
We go and try to counsel people; we arrive at places, and the people have fled because the police jamii have come and beat them. If they catch you smoking [heroin], they take you to the police or beat you. They sometimes severely hurt people. They use whips, belts, a fish tail whip called mkia wa taa. Sometimes they beat people with HIV or TB or hepatitis without knowing it. It has been reported several times.[177]
His colleague added, “They think they’re above the law.”[178]
Idris Z. is among those who have suffered brutality at the hands of the police jamii, with the complicity of the regular police. He recounted that in late 2011, police jamii arrested him while he was sleeping outside in a location known to be frequented by people who use drugs, and took him to Jangombe Police Station:
The police jamii said, “We caught him because he’s always sleeping outside and he steals.” The police jamii [told] the regular police, “Give us these guys.” The regular police accepted.
The police jamii took us back to the neighborhood. They took us to a field and beat us. They took mucuna bean [upupu] and spread it on us to make us itch. Then they told us to go home. They laughed, because they were happy to be torturing someone, especially an addict.[179]
One MSM activist complained that he had been beaten by police jamii in Dar es Salaam, although it was not clear whether the perpetrators were police jamii or Sungu Sungu:
Last year me and my boyfriend were sitting somewhere talking. The police jamii came, they assist the police. We used to call them Sungu Sungu. They said, “What are you doing here with this guy? Do you have sex here?” We said, “No, we’re just talking.” [One of them] said, “Ok, take them. Tie them.”
My boyfriend got a chance to run away. They tied my hands behind my back with a rope. I was not able to do anything…. They took me somewhere, untied me, and forced me to bend over. They started to beat me with wire, electric wire that is used to supply the power. They seriously hurt me. They beat me on the back and on the behind. I was screaming “You’re hurting me, please.” [180]
The activist eventually managed to run away, and went to the regular police to report the incident, but there was no follow up by the police despite their promises to investigate. He concluded, “The ones who beat me dislike homosexuals—that’s why they beat me.”[181]
By failing to investigate such crimes, or by encouraging them, as in Idris’s case above, the regular police are often complicit in abuses by police jamii and vigilante groups. One person reported that police attempted to rein in police jamii abuses. Ally H. was arrested at home by six police officers from Kilimahewa Police Post and an informant from the police jamii on suspicion of selling drugs in September 2012:
The police jamii started to beat me. The real police told him to stop. And also the informant collected some syringes and boxes from my house, but the real police told him, “Stop taking these, because they’re providing them from somewhere [an NGO].” [182]
Nonetheless, the police still extorted a Tsh 5,000 bribe (about $3) in exchange for Ally’s release.[183]
V. Lack of Access to Justice for Crime Victims from Marginalized Groups
When members of at-risk populations are assaulted by fellow citizens, they feel they have nowhere to go to seek justice, out of fear that they themselves will be treated as criminals.
The majority of sex workers interviewed by Human Rights Watch and WASO have been violently mistreated by clients, but in almost all cases, the sex workers said they could not press charges. Asha W., a 15-year-old girl engaged in sex work in Mbeya, was drugged by a client in a bar and then vaginally and anally raped while unconscious. She was in pain for several days afterwards. Asha explained why she did not complain to the police: “I was afraid, because if I went to the police I would have to say I was selling myself, and the police would say I agreed to it, and the case would end there.”[184]
Mwamini K., a sex worker in Dar es Salaam, was forced at gunpoint to have sex with a client without a condom:
I said I didn’t want to do it without a condom. Suddenly he pulled out a gun and pointed it at me. I continued to refuse. Finally I decided to have sex without a condom ... I couldn’t go to the police.[185]
Police sometimes outright refused to assist members of key populations when they were subjected to violence. According to Louisa T., a sex worker in Mwanza,
We don’t have any rights. In September I was coming from a guest house. I met with two guys in the street. One guy grabbed me and picked me up. He was carrying me and I was screaming. The police were there. They saw but they didn’t do anything because they knew I was a sex worker.[186]
In other cases, police only inflicted further violence on victims. Mickdad J. said that in February 2012, he was nearly beaten to death by a mob in Dar es Salaam who suspected him of drug use and theft:
I was coming from my sister’s place at 5 a.m. and there was a place with local music. An incident happened there where someone stole a phone. So they suspected me. People surrounded me because I use drugs. They said “That’s him,” and they started to beat me. They beat me with stones, on the head, on the back, on various parts of the body. After that, they were asking to set me on fire with tires. Some were going to find kerosene and some were going to find tires. I heard this and got a power from God and started running away to the Mamboleyo police post by myself.
When I got there, the police knew me. They know me as a drug user. So they believed I took the phone and started to beat me…. One of them was holding me by the neck from behind, another took a belt and started to beat me. It’s a belt from a milling machine [for running motors]—it left marks of one inch wide. He hit me with the belt in various places—on the head, on the butt, on the foot—he didn’t choose. I was beaten until my eye was swollen. I slept in the cell.
In the morning, Mickdad’s mother bribed the police to release him out of custody. He then reported the case to Médecins du Monde. They sent him with a local human rights activist from the Nyerere Human Rights Centre to file a complaint, but they only found police jamii at the station. He said:
We asked for the police officers who were there at night. But someone phoned those police and said “Don’t come, there’s a drug user here with other people.” We went back at 4 p.m. and they weren’t there.
After that I was left with pain from having been beaten and I was silenced. The police failed to help me….[187]
Watende A. was accused of thefts in his neighborhood in March 2012. He was followed by an angry mob to the Médecins du Monde office, and staff defused the situation.[188] Two days later, however, Watende said, community members found him in the maskani preparing to use drugs:
They started to beat me with pangas and sticks. [They took me to] the police. The police said, “Why did you bring him alive? This is the thief you were talking about? You could have just killed him and we could have taken the body.” [189]
The police did provide Watende A. with Police Form Number 3 (PF3), which hospitals require in order to treat assault victims. However, they took no steps to arrest or investigate the perpetrators. When Human Rights Watch met Watende three months after the incident, he had scars across his chest and back that were consistent with being cut with machetes.
It is not unusual for Tanzanian police to demand bribes from crime victims in order to help them. But marginalized groups may be particularly vulnerable. Jamal P., an MSM in Zanzibar, said four of his neighbors beat him in the street in December 2011, while shouting homophobic insults at him. They cut him on the bridge of the nose and on the head with a panga, and left him lying in the street. Jamal made it to Mnazi Moja Hospital for treatment and then reported the incident to the police:
I told the police the names of the people who beat me, but the police despise me—they know I’m MSM. They wrote down my statement, including the names. But they didn’t follow up. I went back two times to see what was happening with the case, but they weren’t doing anything, so I gave up. One time when I tried to follow up, a policeman asked for money, and I refused. Then he said, “If you don’t have money, give me sex.” I continued to refuse.[190]
Abdalla J. was attacked in 2011 at a Dar es Salaam bus stop by a man who called him a derogatory term for gay, beat him, and stole his phone. Abdalla told Human Rights Watch and WASO:
I couldn’t go to the police. If I said I was beaten, they would have asked why. We used to go to the police, some time back. But the police would recognize us as gay. We would try to lie about why we were beaten, and we would say, “I was robbed,” or something like that. But then someone would come through and say, “He’s a gay,” and then they would refuse to help us.[191]
Rahim R., an MSM who was beaten and cut on the stomach with a knife in 2008 after dancing with other men at a party, had similar fears: “I didn’t go to the police. What could I say? What was I going to explain to the police about what I was doing in order to get beaten?” [192]
Ramazani H., a 22-year-old male sex worker in Dar es Salaam, told Human Rights Watch and WASO that he has been beaten by neighbors at least 10 times, but never went to the police. He explained, “I’m afraid to go to the police because they might tell me I don’t have rights. They might say “we’re not dealing with gays’ cases, go away.”[193]
Wilson N., a former sex worker in Dar es Salaam’s Temeke district, said bandits often confronted him on his way home from doing sex work and beat, robbed, and raped him. Wilson feared going to the police, though: “I’m afraid of being stigmatized by the police. I can’t go to report that somebody raped me, because the law does not allow anal sex, so I’m afraid of being arrested.”[194]
The case of another male sex worker, Ismail P., shows that such fears have a basis in reality. Ismail told Human Rights Watch and WASO,
When coming from sex work, I have met street boys who go around at night. They took my phones, money, raped me, beat me. I don’t remember how many times—I have been raped many, many, many times, too many times to remember. It happens in the alley ways on the way home.
I’ve gone to the police about this, but when I got there they refused to listen to me and said, “Go away, we don’t have time to listen to your case, we can’t listen to the gays’ cases.” So I was discouraged about reporting cases to the police.[195]
Starting in 2011, the police have established Gender and Children’s Desks at a number of police stations, and plan to eventually have such desks operative at every police station in the country.[196] The desks are to be staffed by specially trained police officers that can handle issues such as sexual and gender based violence and child abuse. Most Gender Desks are only partially operative, with frequent staffing changes making it difficult to retain trained officers. Most sex workers and LGBTI people interviewed by Human Rights Watch and WASO had not turned to Gender and Children’s Desks in order to address their complaints. In part, this is because the Gender and Children’s Desks remain part of the same police system that subjects LGBTI people, sex workers, and people who use drugs to violence and repression.
VI. Discrimination in the Health Care Sector
In September 2012, an official at the Ministry of Health and Social Welfare told Human Rights Watch,
The policy is clear: no one is to be denied health services, even if someone may equate [their behavior] with something that is not legally acceptable. Criminalizing it does not amount to denying someone health services. The service side should not be informed by the legal position of our country.[197]
But despite government commitments to equal access to health care, members of key populations experience multiple violations of their right to the highest attainable standard of health. These included outright denial of care, verbal abuse and harassment, and onerous requirements that disproportionately impact marginalized groups. This occurs when hospitals require that those being tested for sexually transmitted infections (STIs) bring in their partner, a requirement with which sex workers and men who have sex with men cannot easily comply, since even if they could convince their partners to come in, they would risk stigma—or require that assault victims obtain a form from the police before being treated, even when victims have been assaulted by the police themselves.
Government agencies and NGOs have undertaken recent efforts to sensitize health workers about the needs of key populations. In Zanzibar, the AIDS Commission and the Zanzibar AIDS Control Programme (ZACP) have taken a pragmatic approach to HIV, providing training on most-at-risk populations aimed at health workers, the police, and the police jamii.[198] An MSM activist in Dar es Salaam told Human Rights Watch that as part of the government-sponsored Tanzania AIDS Prevention Program (TAPP)
We’re trying to collaborate with Muhimbili [National Hospital] to provide condoms, lubricants, and peer education. At other health clinics you lie in order to get tested—they ask you when you last had sex, and where your girlfriend is. There are Angaza centers [Voluntary Counseling and Treatment Centers (VCTs)] in the districts. I went to one and the woman started preaching to me not to have sex with men. I left, and went to another place. We need a friendlier place to get tested.[199]
TAPP outreach workers are also working with other government hospitals to improve their receptiveness to MSM. Additionally, three NGOs—Engender Health, PSI, and T-Marc—have joined forces in the Husika Project, which seeks not only to conduct HIV outreach to MSM and sex workers, but also to train government health workers in order to reduce stigma.[200] Médecins du Monde has implemented a training curriculum for health workers in Temeke to raise awareness regarding drug use and people who use drugs. So far more than 100 employees working in various hospitals, clinics, and dispensaries have been trained.[201]
Even absent specific training, some health professionals in Tanzania carry out their functions without bias. Christian B., a gay man, went to Mbeya Referral Hospital with a case of anal gonorrhea. He told Human Rights Watch, “They examined my body, including my anus. They did not stigmatize me. They just gave me medication, and I left.”[202] In Arusha, Mt. Meru Hospital has a good reputation for dealing sensitively with people who use drugs.[203] The testimonies below, however, suggest these cases are the exception rather than the norm, and that training and accountability for health professionals is required.
When public hospitals are inaccessible, NGOs often step in to fill the gap. An international NGO with an office in Mwanza, AMREF, has trained staff at VCTs to be attentive to the needs of female sex workers. AMREF advises female sex workers that they can go to these VCTs to get friendly services.[204] In Dar es Salaam’s Temeke district, PASADA, a Catholic-run clinic, is friendly and accessible to key populations.[205] In Zanzibar, ZAYEDESA runs a VCT that is accessible to key populations.
However, most Tanzanians still rely on public dispensaries and hospitals as their primary course of health care. At these institutions, despite slight improvements in recent years, numerous obstacles to the right to health remain.
Denial of Health Care
Some members of key populations face outright denial of health services. A gay man in Dar es Salaam, Collins A., was turned away from a government dispensary in the Tandika neighborhood of Dar es Salaam in December 2011. Collins told Human Rights Watch and WASO, “The nurses said, ‘We can’t give you services here. We can’t treat a person like you. Even the public doesn’t want to see you.’”[206]
When Alex N., a transgender man, sought treatment for an STI at a Dar es Salaam dispensary, a doctor told him, “It’s not possible. What kind of person are you?” and refused to treat him. After asking friends for advice, Alex returned to the dispensary to see another doctor who was known to be more open-minded, and who provided him service.[207]
Lack of care can have serious and even fatal consequences. Human Rights Watch and WASO interviewed the friend of a gay man who died in 2011 after being turned away from Temeke District Hospital. He told us:
I was the one who was taking care of him and who took him to the hospital. He was suffering malaria and had a high fever. At Temeke District Hospital, there was a doctor at the reception who knew we were gay. The doctor said “Go away! There’s no service for people like you.” So we went to PASADA [a Catholic-run health clinic]. He was tested for HIV there. They said, “Come next week for your results.” They don’t have hospital beds, it’s just a VCT. But within the next week, before getting his results, he died. No one went to get his results.[208]
Recently, activists providing support to the MSM community in Temele met with district hospital officials to sensitize them about MSM health issues. The activists expressed optimism that treatment may improve following this initiative.[209]
Jamal P., a 28-year-old gay man in Zanzibar, told Human Rights Watch that in March 2012, he went to Mnazi Mmoja Hospital to be treated for an STI. Jamal said,
The doctor examined me and told me it was gonorrhea, but then refused to treat me. He said “You already have sex with men, now you come here to bring us problems—go away.” He told me he wouldn’t treat me because I’m MSM. I came back home and my mom took me to a private hospital.[210]
The following month, however, Mnazi Mmoja Hospital initiated a groundbreaking program in which a doctor, trained specifically to address the needs of key populations, is available to provide services two days a week.[211] LGBTI rights activists in Zanzibar were optimistic about opportunities for improved services under this program.[212] Mnazi Mmoja personnel have proactively informed key populations of the services available: when they realized that few people were accessing their services, they began sending out peer educators and partnering with community organizations in order to conduct outreach, a model that could be replicated elsewhere in Zanzibar and on the mainland.[213]
Verbal Abuse, Harassment, and Violations of Confidentiality
Human Rights Watch and WASO documented a number of cases in which health workers verbally abused and harassed individuals, deterring them from seeking services in the future. Lester F., an 18-year-old gay man in Arusha, is effeminate and sometimes wears make-up, and is often identified as gay. He told Human Rights Watch and WASO,
Once I was discriminated against when I went to test for HIV. I went to the Angaza (VCT) as usual. After the test, I was waiting for the results. When the results came, the doctor looked at me and said, “I know what you’re doing. Stop what you’re doing, it’s very bad.” I just took the results and said, “Thank you,” and left to avoid problems.[214]
Carlos B. developed an anal STI and went to Mwananyamala Hospital (also known as Kinondoni District Hospital) in Dar es Salaam. Despite Carlos’s efforts to mask his sexual orientation, the doctor verbally abused him:
I was afraid to tell the doctors about my sexual orientation because of the stigma and discrimination in society, so I created a fake story to convince the doctor to listen to me. I said, “Three days ago, I was drunk, I passed out somewhere, and people raped me. So I think I got anal STIs.” The doctor started to insult me, saying, “You are a man, why are you doing this? It’s not right for a real man to do something like this.” I said “I’m not a gay, it wasn’t my fault, it just happened.” The doctor said, “Next time, don’t do something like that, you are a man, you should not drink so much alcohol so that you let something like this happen, you have to have a limit.”[215]
Treatment varies widely from one medical professional to another. Ismail P., a sex worker, told Human Rights Watch and WASO he frequently caught STIs, in part due to the large number of clients who refused to use condoms. He said,
When I got STIs and went to the hospital, some doctors treated me well, others mistreated me—it depends on the doctors who are there for that day. Some treat me like any other patient. Others say, “I’m not feeling comfortable to treat you, let me call another doctor.” Some say, “You know, my religion doesn’t allow this,” or “The law of the country doesn’t allow this.”[216]
Many LGBTI people resort to paying high fees at private hospitals in order to avoid discrimination at public hospitals. Mohamed R. said, “I once had an STI in the anus. I went to Temeke District Hospital, and I was mistreated and not even checked on. But I was treated well in a private hospital, where I brought my lover and he got treated too.”[217]
Men who have sex with men also experience harassment and abuse when they seek treatment for problems other than sexually transmitted infections. Peter E. also went to the hospital after being beaten because of his sexual orientation. He explained to the doctor the circumstances under which he had been attacked. He said, “When I was open to a doctor about my sexual orientation, the doctor started to call others, saying ‘Hey doctor, come here!’ and told them I was gay…. You feel inhuman to be there.”[218]
Ismail P. told Human Rights Watch and WASO that he was also attacked in the street because of his effeminate appearance. He was beaten unconscious and woke up in the hospital. There, he experienced varying treatment:
Some doctors were treating me well, but others were abusing me, insulting me, saying, “These people, it was his fault, he’s supposed to be beaten. You shouldn’t give him a treatment, just leave him. Why do men come and do such things? Why is he a gay? Why’d he decide to be a gay? It’s his fault. It’s good for people to beat him.” And others were saying “No this is unfair, this is also a human being, he is not supposed to be beaten.”[219]
Hayat E., an intersex person born with both male and female sexual organs, told Human Rights Watch that at public hospitals, “They begin to point fingers at you, and I can hear them talking. They call each other to see me, and then the other patients also begin to wonder about me…. I get scared to attend hospitals.”[220]
People who use drugs, too, are humiliated and mistreated by medical professionals, perhaps largely because they are assumed to be “thieves.” As described in Section II above, after January H. was attacked in Dar es Salaam by a mob of Sungu Sungu who cut him on the face with pangas, Temeke Hospital staff called him a “thief” and refused to use anesthesia while stitching him up.
Mwajuma P. said she believed women who use drugs were particularly stigmatized: “At Temeke Hospital and Muhimbili Hospital, I’ve been stigmatized. Drug users in this country, especially women, are not valued…. At Muhimbili sometimes the nurses say, ‘These are drug users,’ and they call others. At Temeke they also do this.”[221]
In both Dar es Salaam and Tanga, NGO-run drug treatment programs provide beneficiaries with cards that identify them as participants in treatment programs, which assist them in accessing hospital care. Those who participated in such programs reported a lower level of stigma.[222] A representative of a Tanga community-based organization explained, “Without a card, it’s hard to get service, because of stigma from providers. The providers think they might steal something, or just don’t like the way they look.”[223]
Requirement to Submit Police Form Number 3 (PF3) before Treatment
Tanzanian hospitals require that assault victims submit a form known as Police Form Number 3 (PF3) prior to being treated.[224] The purpose of the form is to ensure that police have a record of all assaults, and that crimes can be investigated and perpetrators prosecuted.[225] Hospitals will occasionally admit a patient without a PF3 if their situation is judged urgent, but in other cases, patients without PF3s are sent to the police station before receiving treatment.[226] Victims told Human Rights Watch and WASO that private hospitals were more likely than public hospitals to waive the requirement, but most Tanzanians cannot afford private hospitals.
The PF3 requirement impedes access to health. For those who have been assaulted by the police themselves—or who are reluctant to go to the police for fear of facing repercussions—treatment is out of reach, either because police outright refuse to provide the form or because victims are afraid to request it. Medical treatment in the aftermath of any assault, including sexual assault, should not be linked to or dependent on criminal proceedings. Victims should be able to seek and receive medical care, regardless of whether they choose to report the crime.
Suleiman R., suspected of robbery because of his drug use, was assaulted with a hot iron by a police officer in Temeke district in December 2011 (see Section III, above). After he was released from custody, he went to Chang’ombe police station with his mother in order to get a PF3 and seek treatment:
My mother explained, “He was beaten by the police and needs to go to the hospital.” A corporal at the station refused and said “If we give you a PF3, you will accuse the police in court.”
Suleiman had to go to a private hospital, where he paid Tsh 35,000[about $20] for treatment.[227]
Susan N., a sex worker, went to a public hospital in 2011 after a client forced her to have anal sex, but she could not get treatment without filing a police report:
When I went to the hospital on that night with a bruised anus they refused to treat me unless I reported to the police first. This made me decide to go home and seek medical attention the following day at a private hospital. It cost a lot of money but at least I got the service I required.[228]
Some members of key populations lie to police or hospital staff in order to acquire a PF3 or to evade the requirement to have one. This may lead to inadequate treatment: if patients cannot be forthright about the causes of their injuries, health workers may not know what to look for. Walter S. has invented stories in order to get a PF3 on the several occasions that he has been beaten by neighbors because of his drug use: “Sometimes you go and make a fake story to the police that you fell or something like that to get the PF3. You do not want to tell them that you were beaten because you are a drug user. So you say, ‘I had an accident with a motorbike.’”[229]
Mwamini K., a sex worker in Dar es Salaam, lied to hospital staff in order to get treatment after being beaten by police officers in Kinondoni District in 2011:
They were three police officers. They beat me with their hands, and kicked me. They were saying, “What are you doing here, you’re a prostitute, a dog, you are a pig”…. I went to the hospital because they had hurt me badly. I had damage on my skin. My whole body was hurting. I told the doctor that I fell down the stairs. If I had told them what really happened, they would need a PF3. I was afraid to go to the police to get forms because they would ask me many questions and they would want to arrest the person who beat me—and if those police [officers] were arrested, they would say that I was a sex worker.[230]
Others simply self-medicate or do not get any form of treatment because of the PF3 requirement. Jamila H., a sex worker, was gang-raped in February 2012 and went to a public hospital, but was told she needed a PF3. She told Human Rights Watch, “They said I should go to the police, but I couldn’t because I was a sex worker.” Two of her rapists had not used condoms, but absent access to hospital services, she did not get tested for HIV.”[231] Denied hospital treatment, Jamila bought basic medicines at the pharmacy.
Some police take advantage of the vulnerable position of key populations in order to extort money from them in exchange for a PF3. Maureen B., a sex worker in Dar es Salaam, was beaten by a client in 2010:
I was taken to the hospital by another girl, but first they wanted a PF3. We had to go to the police station to get the document and because they realized I was a sex worker, they made me pay Tsh 20,000.[232]
Others paid bribes to medical professionals rather than the police. Dalili S., a sex worker, said, “When I get injured when working, I have to bribe some of the night doctors so that I can receive service without going through the process of obtaining a PF3.”[233]
In December 2011, the Ministry of Health and Social Welfare launched national guidelines on gender-based violence that would allow victims of sexual and gender-based violence to receive medical services before acquiring PF3 forms from police stations.[234] Such guidelines are an excellent initiative, but experiences such as that of Jamila H., above, suggest that as of 2012 the guidelines were not being uniformly implemented. Additionally, because they only apply to sexual and gender-based violence cases, they only provided limited relief: those who are victims of police torture or who are attacked by angry mobs due to their presumed sexual orientation or drug use would not benefit from such waivers.
Requirement to “Bring Your Partner”
Some Tanzanian health workers refuse to treat patients for sexually transmitted infections unless they bring their partner. Human Rights Watch and WASO were unable to determine whether this requirement is based on an official policy or law, and the Ministry of Health and Social Welfare did not respond to written inquiries regarding the nature of the requirement. While such a requirement may derive from a desire to ensure treatment of all people infected or affected by HIV and other STIs, it is counterproductive when it comes to sex workers and LGBTI people who may be unable to convince partners to seek treatment, even if they themselves are willing to do so and only serves to drive patients underground. Mwamini K., a sex worker in Dar es Salaam, recounted her experience going to Mwananyamala Hospital to seek treatment for a fungus:
They normally ask you to bring your partner. I told them the truth, “I don’t have a partner, I’m a sex worker, and I got this STI in my work.” The nurse refused to treat me. She said “I can’t treat you without getting your partner.” I left and went to a private hospital.[235]
Pili M. had a similar experience at Sinza Hospital in Dar es Salaam. When she went for STI treatment and said she could not bring in her partner, according to Pili,
[The nurse] said “Do you do sex work or what? You are a liar. Because this STI is very bad”… She refused to treat me, saying “I can’t treat you until you bring your partner.”[236]
This requirement is not uniform. According to Melissa L., a sex worker in Arusha, “It’s OK when we explain that we can’t bring our partners. Even at government hospitals, they understand. They don’t judge us, but give us advice to use condoms.” [237] In Zanzibar, organizations working with sex workers said testing was not conditioned on bringing in a partner. [238]
These models should be adopted across Tanzania, given that the alternative is that vulnerable populations go without testing and treatment.
Lack of Access to Lubricant
The use of water-based lubricant is an important protective measure during anal sex. Condoms are more likely to tear when sexual partners engage in anal sex without lubricant, or when they use oil-based lubricants such as Vaseline. Unfortunately, in most of Tanzania, water-based lubricant is unavailable or prohibitively expensive. Almost all the MSM interviewed by Human Rights Watch and WASO said they did not know where to get water-based lubricant or could not afford it; several did not know the benefits of water-based lubricant or did not know what it is. The few who did have access to water-based lubricant relied on Dar es Salaam’s HIV/AIDS organizations that serve MSM, which themselves sometimes have an irregular supply.
Access to water-based lubricant appears most severely limited outside of Dar es Salaam. According to Lester F. in Arusha, “It’s easy to get condoms, but not lubricant. You might go to five stores asking for it without getting KY. So I’m using Vaseline.”[239] Lester was aware that Vaseline posed the risk of damaging condoms, but did not see an alternative.
In Mbeya, Christian B., a sex worker, told Human Rights Watch he had only once tried water-based lubricant, when a client brought it from Dar es Salaam. On other occasions, he used oil-based lubricant. Christian B. knows he takes risks, but he has never been tested for HIV; he said he is afraid to know his status because he does not know where he will get support if he finds out he is HIV-positive.[240]
A 19-year-old MSM in Tanga that did occasional sex work told Human Rights Watch and WASO that he had never heard about lubricant, either water-based or oil-based; he only used saliva for lubrication during anal sex.[241]
VII. Tanzanian, Regional, and International Law
This report deals with three forms of conduct—consensual same-sex conduct, sex work, and personal drug consumption—which international law does not address in a uniform manner.
However, human rights protections apply in all three cases. When police or semi-official vigilante groups mistreat or arbitrarily arrest members of any marginalized group, or when health workers deny them services, their actions violate clear international human rights principles. They also often violate Tanzanian law.
Tanzania has initiated a constitutional review process, which provides an opportunity to further domesticate human rights. Drafters should consider establishing a Bill of Rights; building in strong anti-discrimination provisions; and clarifying the primacy of international treaties that Tanzania has ratified.
Consensual Same-Sex Conduct
The criminalization of same-sex conduct between consenting adults violates the right to privacy and the right to freedom from discrimination, both of which are guaranteed rights under the International Covenant on Civil and Political Rights (ICCPR) to which Tanzania is a party. [242] To arrest someone on the basis of consensual same-sex conduct is a violation of the prohibition on arbitrary detention. [243]
The African Commission on Human and People’s Rights has argued that discrimination on the basis of sexual orientation is in violation of non-discrimination provisions in the African Charter on Human and People’s Rights.[244] Tanzania’s constitution also prohibits discrimination. Article 9, “The pursuit of Ujamaa and self-reliance,” sets forth:
… [T]he state authority and all its agencies are obliged to direct their policies and programmes towards ensuring… that human dignity is preserved and upheld in accordance with the spirit of the Universal Declaration of Human Rights… [and] that all forms of injustice, Intimidation, Discrimination, corruption, oppression or favoritism are eradicated.[245]
Further, article 13 provides for equal protection before the law and prohibits the government from enacting discriminatory laws. [246] Article 16 protects the right to privacy. [247]
No one has ever brought a case before a Tanzanian court that tests these provisions’ applicability to sexual orientation or gender identity, but a court could find that laws banning same-sex conduct are unconstitutional.
Sex Work
Human Rights Watch believes that the criminalization of the voluntary, commercial exchange of sexual services between consenting adults, as in the case of sex work by consenting adults, violates the right to privacy, including personal autonomy, protected under the International Covenant on Civil and Political Rights (ICCPR).[248]
In addition, the type of identity-based arrests that take place frequently in Tanzania—the practice of police arresting someone solely because she or he is known as a “sex worker” –violates prohibitions on arbitrary arrest under article 9 of ICCPR and articles 4 and 6 of the African Charter on Human and People’s Rights (ACHPR). [249] Tanzania’s constitution also prohibits arbitrary arrests. [250]
Sexual Exploitation
Commercial sexual exploitation of children is strictly prohibited under both national and international law.[251] In all such cases, the person exploiting the child—not the child him or herself—should be penalized. Tanzania’s National Costed Plan of Action for Most Vulnerable Children identifies as one of its target groups “children involved in the worst forms of child labour,” including “sexual exploitation.”[252] The plan, if implemented, will lead to increased resources for protection and rehabilitation of children engaged in sex work.
Personal Drug Consumption
States are obliged to protect the human rights of all persons, regardless of whether or not their actions violate domestic law. By arresting suspected drug users arbitrarily, on the basis of their “status” as persons who use drugs and in the absence of evidence that they are actually engaged in drug use, Tanzanian police violate article 9 of the ICCPR and articles 4 and 6 of the ACHPR, which protect all persons from arbitrary arrest.[253]
Tanzania should review and reform existing laws that criminalize personal drug consumption and possession of drugs for personal use, in order to ensure that the human rights of people who use drugs are protected and that drug laws do not increase vulnerability to HIV infection or impede access to HIV prevention, care, or treatment.
Right to Be Free From Torture
International law strictly prohibits torture. This prohibition is reflected in article 5 of the ACHPR and articles 7 and 10 of the ICCPR. [254] Tanzania is one of a handful of countries that has not ratified the Convention against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment, which codifies the prohibition on torture and ill-treatment and imposes a series of procedural obligations on states aimed at preventing torture and remedying it, should it occur. [255] The beatings and forced sex to which many Tanzanians have been subjected in police custody clearly contravene the prohibition on torture.
Tanzania’s constitution states that “no person shall be subjected to torture or inhuman or degrading punishment or treatment.” [256] Further, “for the purposes of preserving the right or equality of human beings, human dignity shall be protected in all activities pertaining to criminal investigations and process.” [257]
In order to demonstrate its commitment to human rights and human dignity, Tanzania should ratify that Convention against Torture and should ensure that torture is a crime prosecutable under its Penal Code and Criminal Procedure Code.
Right to the Highest Attainable Standard of Health
The right to the highest attainable standard of health is guaranteed under the African Charter on Human and People’s Rights, the International Covenant on Economic, Social and Cultural Rights, and the U.N. Convention on the Elimination of all Forms of Discrimination Against Women. [258] Importantly for key populations, access to the right to health must be on a non-discriminatory basis. Discrimination on the basis of sexual orientation and gender identity is explicitly prohibited by international law. [259]
This right imposes an obligation on states to take necessary steps for the prevention, treatment and control of epidemic and other diseases. In meeting this obligation, states “should ensure that appropriate goods, services and information for the prevention and treatment of STDs, including HIV/AIDS, are available and accessible.”[260]For drug users, ensuring the right to the highest attainable standard of health should involve expanding harm reduction programs.[261] For all key populations, in should involve ensuring access to condoms and water-based lubricant.
Regionally, the East African Community (EAC) has begun to take steps toward protecting the right to health, specifically with regard to HIV/AIDS. The East African Legislative Assembly, which includes representatives from Burundi, Kenya, Rwanda, Tanzania and Uganda, passed the East African Community HIV & AIDS Prevention and Management Bill in April 2012. [262] The bill has not yet been signed into law by the East African Community (EAC) heads of state. If it becomes law, it may offer some protections for sex workers, men who have sex with men, and people who inject drugs: it calls on governments to challenge stigma and discrimination against most-at-risk populations; [263] to implement strategies to promote and protect the health of most-at-risk populations; [264] and to ensure that recognized protective methods are available to most-at-risk populations. [265]
The Maputo Protocol on the Rights of Women in Africa, to which Tanzania is a state party, provides that states must ensure the “the right to self-protection and to be protected against sexually transmitted infections, including HIV/AIDS.” [266]
Right to Security and Bodily Integrity
Tanzania is obligated to protect all persons, including members of marginalized groups, from violence. The state has the responsibility of the state to investigate and prosecute violence, whether by state or non-state actors. [267]
Tanzania is also a state party to the Maputo Protocol, which commits states to adopting and implementing appropriate measures “to ensure the protection of every woman’s right to respect for her dignity and protection of women from all forms of violence, particularly sexual and verbal violence.” [268] States parties to the Maputo Protocol further pledge to “enact and enforce laws to prohibit all forms of violence against women including unwanted or forced sex whether the violence takes place in private or public” [269] and to “punish the perpetrators of violence against women and implement programmes for the rehabilitation of women victims.” [270]
Sexual violence—including when the victims are engaged in sex work, and including when the perpetrators are police—is a serious crime under Tanzanian law. Rape is punishable by a maximum sentence of life in prison.[271]
The Penal Code does not currently punish rape of men and boys, who, as this report shows, are sometimes victims of rape, including by police officers. Both penal codes currently define the rape as follows: “It is an offence for a man to rape a girl or a woman.” [272]
While taking steps to remove penal code provisions that criminalize consensual same-sex conduct, legislators should replace them with provisions that criminalize rape of boys and men.
Corruption
Tanzanian law has strong prohibitions on corruption, which includes extorting money or sex. It is illegal for a public official to request sexual favors under section 25 of Prevention and Combating Corruption Act of 2007. [273] A representative of the Prevention and Combating of Corruption Bureau told Human Rights Watch, “It’s a crime even if the victims are sex workers.” The official said that the law protects whistle blowers, and that sex workers, LGBTI people, and people who use drugs cannot be prosecuted on the basis of information they provide to the bureau. [274]
VIII. Tanzanian Government Response
The Tanzanian government has taken some steps toward reducing human rights abuses against members of key populations, most notably by cooperating with NGOs involved in harm reduction and HIV outreach to marginalized groups. However, much remains to be done.
During research for this report, Human Rights Watch met with the Tanzanian Police; the Ministry of Health and Social Welfare; and the Ministry of Community Development, Gender, and Children; as well as with members of government commissions responsible for human rights, HIV, corruption, and drug policy. Government officials were forthcoming in providing information, and acknowledged the seriousness of preliminary findings that Human Rights Watch presented.
Some of the most severe human rights violations documented in this report, including torture and rape, were by police. Elice Mapunda, the chief of Development and Training of the Tanzania Police and founder of the Tanzania Women Police Network, assured Human Rights Watch that she would circulate copies of this report to all 42 regional police commanders and would call on them to ensure accountability for police abuses.
Mapunda said she hoped the Gender Desks would be able to address some of the mistrust between members of key populations and the police, but acknowledged that Gender Desk staff need more training. She recognized the specific need to build police capacity in addressing LGBTI issues. Mapunda defended the requirement for victims of assault to seek a PF3 form from the police, saying it was necessary to allow police to identify crimes and investigate them, a position that Human Rights Watch and WASO maintain poses an obstacle to the right to health. [275]
Officials at government health agencies, including the Tanzania AIDS Commission (TACAIDS) and the Zanzibar AIDS Control Programme, told Human Rights Watch they are seeking to ensure that HIV services are friendly and accessible to all key populations. In early 2013, TACAIDS established a “Key Populations Task Force,” including members of marginalized communities. The Task Force has provided a space for members of key populations to have a say in government policies that affect them. According to Dr. William Kafura of TACAIDS, the police have been invited to send a representative to the Task Force, in order for the police to gain greater exposure to health and human rights issues affecting key populations; Kafura said he hoped this would improve police treatment and reduce arrests. [276]
The Ministry of Community Development, Gender and Children has done little work related to protecting the rights of sex workers, apart from collaborating with civil society organizations such as KIWOHEDE that provide sex workers with alternative sources of income. According to Deputy Permanent Secretary Anna Maembe, “We know sex workers face violence from police and clients, but we rarely follow up on these issues—it’s the police who should follow up.” Maembe explained that ministry officials are involved in training the police on the Gender Desks, but that they have not trained the police on dealing with sex workers. Maembe said the ministry would be open to the possibility of addressing sex worker issues in trainings with the police. The ministry has done no work to date on issues related to women who have sex with women (WSW). [277]
Tanzania has taken insufficient steps to address corruption, including police extortion of money and sex. According to a survey by Afrobarometer, an independent, African-led survey research organization, Tanzanians perceived the police as more corrupt in 2012 than they did in 2008. [278] The Prevention and Combating of Corruption Bureau was established in order to meet the need for an independent body to investigate and prosecute corruption cases, including within the police force, but according to the US Department of State, the PCCB’s record of convictions has been approximately 1 percent of allegations through the last seven years. [279] Further, many cases of extortion are never reported to the PCCB. A PCCB official told Human Rights Watch that members of marginalized groups should feel free to come forward and file complaints, but the bureau itself has done no outreach to build the trust of marginalized communities. [280]
The apparent good will of a number of government officials on addressing human rights and access to health care for key populations is undermined when government officials make intolerant statements, perhaps in order to gain political capital. In March 2013, a Zanzibar government official publicly called for citizens to stand together against homosexuals. According to a UN official, in a context in which mob violence is common, such statements risk inciting violence. [281] Government officials’ public statements about harm reduction for people who use drugs, however, have been more positive: for instance, in March 2013, President Kikwete visited Muhimbili Hospital’s methadone clinic and publicly expressed support for it. [282]
To ensure that Tanzania realizes its goals of protecting marginalized groups from the spread of HIV, and to protect the basic rights of all Tanzanians, good will is not enough. Concrete steps should be taken to reform discriminatory laws and practices; ensure accountability for state actors who violate rights; and train police, health workers, judicial officials and others on the application of human rights to LGBTI people, sex workers, and people who use drugs.
IX. Full Recommendations
To President Kikwete and the Government of Tanzania
- Publicly call for an end to police abuse against sex workers, people who use drugs, and lesbian, gay, bisexual, transgender, and intersex people.
- Establish an independent civilian policing oversight authority, mandated to receive complaints regarding police misconduct, carry out investigations, and refer such complaints to prosecutors.
- Ensure that organizations representing marginalized groups, including LGBTI people and sex workers, are able to register in accordance with Tanzanian law.
- Ratify the Convention against Torture and Other Cruel, Inhuman and Degrading Treatment or Punishment.
- Devote sufficient resources to the Ministry of Health and Social Welfare to strengthen Tanzania’s child protection system, including through implementation of the National Costed Plan of Action for Most Vulnerable Children.
To the Parliaments of Tanzania and Zanzibar
- Begin the process of decriminalizing consensual same-sex conduct by drafting amendments that would remove articles 154 and 157 from the Tanzania Penal Code, and articles 150 and 153 from the Zanzibar Penal Code. Revision to the Zanzibar Penal Code should also remove article 158, prohibiting the “union” of same-sex couples, which violates freedom of association.
- Begin the process of decriminalizing consensual adult sex work by drafting a bill to modify or remove article 176(a) of the Tanzania Penal Code and 181(a) of the Zanzibar Penal Code, which criminalize sex work, as well as other laws related to sex work that may infringe on human rights, including laws on “harbouring prostitutes” and “living off the earnings of prostitution.”
- Exercise the oversight functions of the Parliamentary Standing Committee on Foreign Affairs, Defence and Security (Tanzania) and the Constitution, Justice and Governance Committee (Zanzibar) by investigating police abuse of marginalized groups.
- Through the Standing Committee on HIV/AIDS (Tanzania), conduct an investigation into instances of refusal of services and discrimination against key populations in accessing HIV/AIDS services.
- Review and reform existing laws that criminalize personal drug consumption and possession of drugs for personal use to ensure that the human rights of people who use drugs are protected and that drug laws do not increase vulnerability to HIV infection or impede access to HIV prevention, care or treatment. Introduce revisions to both penal codes that would criminalize rape of men and boys in order to ensure that all non-consensual sexual conduct is prohibited.
To the Ministry of Health and Social Welfare of the Republic of Tanzania, the Ministry of Health of Zanzibar, all Government Institutions Working on HIV/AIDS
- In line with the recommendations set forth by Tanzania’s Second National Multi-sectoral Strategic Framework on HIV/AIDS, publicly call for the decriminalization of same-sex conduct and consensual adult sex work.
- Issue orders to health workers that discrimination against members of marginalized groups, including sex workers, people who use drugs, and LGBTI people, will not be tolerated.
- Conduct inspections of health facilities to ensure that members of marginalized groups are not denied services or discriminated against.
- Develop a complaints mechanism through which members of marginalized groups can report cases of denial of service or discrimination.
- Conduct training for all health workers on key populations, including human rights training as well as training on specific health needs of these groups. Trainings should be carried out in partnership with civil society organizations representing key populations.
- Ensure that the new Strategic Framework on HIV and AIDS includes provisions specifying that all health centers and Voluntary Counseling and Testing centers should be accessible to key populations, and provides concrete plans for training health workers.
- Ensure that the new Strategic Framework on HIV/AIDS includes provisions on protection of the human rights of key populations.
- Ensure that condoms and water-based lubricant are made available and affordable for key populations, either through direct provision by the Ministry for Health, or though facilitating the work of NGOs in supplying them.
- Expand the availability of humane, effective treatment for drug addiction.
- Eliminate the requirement that victims of violence bring in a PF3 form signed by the police before receiving medical treatment.
- Implement the new National Costed Plan of Action for Most Vulnerable Children, which includes child victims of sexual exploitation in its target group. The plan aims to strengthen the capacity of communities and local government actors to protect most vulnerable children, and ensure their access to health, education, and other child protection services.
- Conduct training for Tanzanian media to improve their knowledge and understanding of key populations and their ability to report objectively and sensitively on issues concerning them.
To the Ministry of Justice and Constitutional Affairs of the Republic of Tanzania and the Commission on Constitutional Reform
- Ensure that the draft revision of the Constitution includes comprehensive provisions on equality and non-discrimination.
- Ensure the participation of marginalized groups in constitutional debates.
To the Ministry of Community Development, Gender and Children of the Republic of Tanzania and the Ministry of Social Welfare, Youth, Women and Children Development in Zanzibar
- Take specific steps to protect the rights of adult sex workers, including by establishing partnerships with organizations representing them.
- Take action to end commercial sexual exploitation and assist the victims, as part of your efforts to develop and implement the National Plan of Action to Prevent and Respond to Violence against Children. In particular, activities should include legal assistance, appropriate health and counseling services, and access to education, vocational training, or other social reintegration measures for victims. Activities should also include training for the police.
To the Tanzania Police and the Office of the Director of Public Prosecutions
- Issue orders to all police that no crime victim should be denied assistance, arrested, or harassed on the basis of their sexual orientation or gender identity, or their status as a sex worker or drug user. Publicly announce that members of at-risk populations can report crimes without facing the risk of arrest.
- Establish police liaisons to each of the at-risk communities discussed in this report. Liaisons should be police officers that have a track record of integrity and are trusted by these populations. They should be mandated to engage with key populations on building trust between the police and these communities, without using any information they gather in the course of their mandates against members of these communities.
- Investigate the police stations and police officers mentioned in this report in relation to human rights violations, and where necessary, undertake prosecutions or disciplinary measures.
- Issue orders to police that no one should be arrested for possession of materials related to harm reduction, such as clean needles or syringes and bleach to disinfect needles.
- Train officers responsible for “Gender Desks” at police stations on sexual orientation, gender identity, and the human rights of sex workers and children engaged in sex work.
- Arrest and prosecute members of the “police jamii,” Sungu Sungu, and other community-based security groups who violate the law.
- Strengthen oversight of community-based security groups, including by ensuring that they do not carry arms and do not use force.
- Ensure that anyone who uses, offers, obtains, procures or provides a child for the purposes of commercial sexual exploitation be prosecuted, including when the perpetrator is a police officer or other state agent.
- Ensure that children who are commercially sexually exploited or engaged in sex work are not prosecuted or penalized for having been party to illegal sex work.
- Ensure that police training on human rights is carried out regularly and rigorously, and that it includes training on the rights under international law of LGBTI people, sex workers, and people who use drugs.
To the Commission on Human Rights and Good Governance (CHRAGG)
- Publicly encourage LGBTI people, sex workers, and people who use drugs to report any cases of discrimination or violence to CHRAGG, and take appropriate actions in response to any such reports.
- Train all staff on tolerance, non-discrimination, and sensitivity to the needs of marginalized groups. Trainings should be carried out in collaboration with members of marginalized groups.
- Designate one commissioner to take responsibility for handling cases of human rights violations against members of key populations.
- Conduct a nationwide study on discrimination against key populations, in partnership with civil society organizations representing them.
To the Prevention and Combating of Corruption Bureau (TAKUKURU)
- Mandate outreach officers to liaise with sex workers, people who use drugs, and LGBTI people in order to collect information about extortion, including extortion of sex, affecting these communities.
- Initiate prosecutions against police officers found to be involved in extorting money and sex from members of marginalized groups.
To the Drug Control Commissions of Tanzania and Zanzibar
- Review existing laws that criminalize personal drug consumption and possession of drugs for personal use, in consultation with UNAIDS and other experts, to ensure that drug laws are consistent with the goals of reducing the spread of HIV and protecting human rights.
To United Nations Agencies Operating in Tanzania, including UNAIDS, UNDP, UNFPA, UNICEF, and UN Women
- Engage in public and private advocacy with the Tanzanian government about the rights of persons of marginalized groups under international law.
- Organize discussions with government officials on recent literature, including UN-backed research, demonstrating that criminalization of sex work and same-sex conduct imposes obstacles to preventing and treating HIV.
- Document human rights violations against sex workers, LGBTI people, and people who use drugs. Report on these violations to the government of Tanzania and in other appropriate settings, such as the Universal Periodic Review at the UN Human Rights Council.
- Conduct training for Tanzanian media to improve their knowledge and understanding of key populations and ability to report objectively and sensitively on issues concerning them.
- Ensure that UN-funded training of police, justice officials, and health officials includes training on the human rights of marginalized groups.
To Donor Governments and Institutions Supporting HIV/AIDS Programs or Human Rights Programs in Tanzania
- Support the development of membership organizations among sex workers, LGBTI people, and people who use drugs, such that these persons can have collective institutional voices.
- Ensure that funding directed to HIV/AIDS in Tanzania includes funds specifically aimed at the health needs of key populations, and closely monitor how such funding is used.
- Ensure that mainstream human rights organizations and lawyer’s associations that receive donor funding are attentive to the human rights of sex workers, LGBTI people, and people who use drugs.
- Provide funding to initiatives in support of children who are victims of commercial sexual exploitation, including the National Costed Plan of Action for Most Vulnerable Children and the National Plan of Action to Prevent and Respond to Violence against Children.
- Engage in public and private advocacy with the Tanzanian government about the rights of persons of marginalized groups under international law.
- Ensure that donor-funded training of police, justice officials, and health officials includes training on the human rights of marginalized groups.
Acknowledgments
This report was researched by Neela Ghoshal, researcher in the Lesbian, Gay, Bisexual, and Transgender (LGBT) Rights Program at Human Rights Watch; Eluka Kibona, consultant to the LGBT Rights Programs at Human Rights Watch; Abdilah Diwani, executive secretary of WASO Coalition; and Geoffrey Mashala, member of WASO Coalition. Ally Semsella and Peter Celestin, also of WASO Coalition, assisted with some interviews, as did Edward Nsajigwa, director of the Nyerere Human Rights Centre.
The report was written by Neela Ghoshal. It was edited by Graeme Reid, director of the LGBT Rights Program at Human Rights Watch; Rona Peligal, deputy director of the Africa Division; Juliane Kippenberg, Senior Researcher in the Children’s Rights Division; Liesl Gerntholtz, director of the Women’s Rights Division; Joe Amon, director of the Health and Human Rights Division; Aisling Reidy, Senior Legal Advisor; and Danielle Haas, senior editor in the Program Office. José Luis Hernández, associate in the LGBT Rights Program at Human Rights Watch provided editorial and production coordination and formatted the report. Additional production assistance was provided by Grace Choi, publications director, and Fitzroy Hepkins, mail manager. This report was partially translated into Kiswahili by Oloo Ochieng’, Naomi Ogutu, and Willy Buloso.
Many individuals in Tanzania played an invaluable role in providing guidance for this research. These included John Kashiha of Tanzania Sisi Kwa Sisi Foundation; Pade Edmund of Stay Awake Network Activities; Oliver Ndalu of Young Women Solidarity Organization; Sophia Lugilahe of the Warembo Forum; Habiba Hashimu of KBH Sisters; Dr. Emmanuel Kandusi of the Centre for Human Rights Promotion; Sylvester Mapinduzi and Elizabeth Tobias of Population Services International (PSI); Usu Mallya of the Tanzania Gender Networking Programme (TGNP); Sandrine Pont and Ancella Voets of Médecins du Monde; Suleiman Mauly of ICAP; Amandine Oleffe of UNAIDS; Dr. William Kafura of TACAIDS; and Onesmo Paul Kasale Olengurumwa of the Tanzania Human Rights Defenders Coalition.
[1] “UNAIDS, “Monitoring and evaluation of key populations at higher risk for HIV,” http://www.unaids.org/en/dataanalysis/datacollectionandanalysisguidance/monitoringandevaluationofkeypopulationsathigherriskforhiv/ (accessed May 8, 2013).
[2] Tanzania Commission for AIDS (TACAIDS), “HIV/AIDS in Tanzania,” http://www.tanzania.go.tz/hiv_aids.html (accessed April 3, 2013).
[3] Jacques Morisset, Waly Wane, and Isis Gaddis, “HIV/Aids: Still Claiming Too Many Lives,” post to Africa Can … End Poverty (blog), February 12, 2013, http://blogs.worldbank.org/africacan/hivaids-still-claiming-too-many-lives (accessed April 3, 2013).
[4] National AIDS Control Programme (NACP), “HIV and AIDS in Tanzania: Information about the Control of HIV and AIDS in Tanzania,” http://www.nacptz.org/ (accessed April 3, 2013).
[5] Morisset, Wane, and Gaddis, “HIV/Aids: Still Claiming Too Many Lives.”
[6] TACAIDS et. al, “Tanzania: HIV/AIDS and Malaria Indicator Survey 2011-2012,” March 2013, p. 103.
[7] Morisset, Wane, and Gaddis, “HIV/Aids: Still Claiming Too Many Lives.”
[8] The Global Fund to Fight AIDS, Tuberculosis and Malaria, “Tanzania,” http://portfolio.theglobalfund.org/en/Country/Index/TNZ (accessed April 3, 2013). Global Fund disbursements go to the Tanzanian government as well as to NGOs and civil society organizations working to address HIV/AIDS.
[9] PEPFAR, “Partnership to Fight HIV/AIDS in Tanzania,” http://www.pepfar.gov/countries/tanzania/ (accessed April 3, 2013).
[10] PEPFAR, “Five-Year Partnership Framework in Support of the Tanzanian National Response to HIV and AIDS, 2009‐2013, Between The Government of the United Republic of Tanzania and the Government of the United States of America,” March 4, 2010, http://www.pepfar.gov/documents/organization/138931.pdf, pp. 6-7. However, only 40% of the population with advanced HIV infection is on ART, compared to 82% in Zambia, 72% in Kenya, 67% in Malawi, and 54% in Uganda. See Morisset, Wane and Gaddis, “HIV/Aids: Still Claiming Too Many Lives.”
[11] UNAIDS, “Monitoring and evaluation of key populations at risk for HIV,” http://www.unaids.org/en/dataanalysis/datacollectionandanalysisguidance/monitoringandevaluationofkeypopulationsathigherriskforhiv/ (accessed April 3, 2013). See also Glossary of Terms. The key populations addressed in this report are not the only hard-to-reach populations; other groups also require heightened attention in Tanzania’s efforts to address HIV-AIDS, including pregnant HIV-positive women in rural areas, who have low levels of access to services to prevent mother-to-child transmission. Tanzania’s new National Multi-sectoral Strategic Framework on HIV/AIDS for 2013-2017 sets forth strategies to address these other hard-to-reach groups as well as key populations.
[12] National AIDS Control Programme, “HIV Behavioral and Biological Surveillance Survey Among Female Sex Workers in Dar es Salaam, 2010,” 2012, on file with Human Rights Watch.
[13] UNAIDS/WHO, “Epidemiological Fact Sheets on HIV/AIDS and Sexually Transmitted Infections: United Republic of Tanzania – 2004 update,” http://data.unaids.org/Publications/Fact-Sheets01/tanzania_en.pdf (accessed April 3, 2013). Information on HIV prevalence among sex workers in Dar es Salaam is available since the mid-1980s. HIV prevalence among sex workers tested increased from 29 percent in 1986 to 49.5 percent in 1993. In 2001, nearly 70 percent of sex workers tested in Mbeya were HIV positive.”
[14] “Preliminary Results from MSM Studies in Dar es Salaam,” Joyce Nyoni, Jasmine Shio and Michael W. Ross, power point presentation on file with Human Rights Watch; Human Rights Watch interview with Dr. Melchizedek Leshabari, Dar es Salaam, May 15, 2012.
[15] Eric A. Ratliff et. al., “An Overview of HIV Prevention Interventions for People Who Inject Drugs in Tanzania,” Advances in Preventive Medicine, Volume 2012, p. 1.
[16] Tanzania is a union between two former British colonies, Tanganyika, and Zanzibar, which became independent in 1961 and 1963 respectively and merged as Tanzania in 1964, with Zanzibar maintaining some autonomy.
[17] Zanzibar AIDS Commission, “UNGASS Country Progress Report, Zanzibar,” January 30, 2008, http://www.unaids.org/en/dataanalysis/knowyourresponse/countryprogressreports/2008otherentities/zanzibar_2008_country_progress_report_en.pdf (accessed May 9, 2013); see also Zanzibar AIDS Commission, “HIV Prevalence in Zanzibar and Tanzania,” http://www.zac.or.tz/national-hiv-response/hiv-prevalence-in-zanzibar (accessed May 9, 2013).
[18] The Revolutionary Government of Zanzibar, “Zanzibar National HIV Strategic Plan II (ZNSP-II), 2011-2016.” Another widely cited study from Zanzibar reports an HIV prevalence rate of 12.3% among men who have sex with men; see Dahoma et. al., “HIV and Related Risk Behavior Among Men Who Have Sex with Men in Zanzibar, Tanzania: Results of a Behavioral
Surveillance Survey,” AIDS and Behavior, December 8, 2009, DOI 10.1007/s10461-009-9646-7, http://www.deepdyve.com/lp/springer-journals/hiv-and-related-risk-behavior-among-men-who-have-sex-with-men-in-NvOUd0vhH7.
[19] UNAIDS, “Guidance Note 2012: Key Programmes to Reduce Stigma and Discrimination and Increase Access to Justice in National HIV Responses,” http://www.unaids.org/en/media/unaids/contentassets/documents/document/2012/Key_Human_Rights_Programmes_en_May2012.pdf (accessed May 31, 2013), p. 5. See also The World Bank, “Increased Targeting of Key Populations Can Accelerate End of Global HIV Epidemic,” November 28, 2012, http://www.worldbank.org/en/news/press-release/2012/11/28/increased-targeting-key-populations-can-accelerate-end-global-hiv-epidemic (accessed May 31, 2013).
[20] Global Commission on HIV and the Law, “HIV and the Law: Risks, Rights & Health,” July 2012, http://www.hivlawcommission.org/resources/report/FinalReport-Risks,Rights&Health-EN.pdf (accessed May 31, 2013).
[21] The Revolutionary Government of Zanzibar, “Zanzibar National HIV Strategic Plan II (ZNSP-II), 2011-2016,” p. 23.
[22] Tanzania Penal Code, Chapter 16 of the Laws (Revised), 1981, http://www.un.org/depts/los/LEGISLATIONANDTREATIES/PDFFILES/TZA_penal_code.pdf, art. 154.
[23] Ibid., art. 157. According to Part I(3) of the Sexual Offences Special Provisions Act, 1998 "gross indecency" in Section 138A “means any sexual act that is more than ordinary but falls short of actual intercourse and may include masturbation and indecent physical contact or indecent behaviour without any physical contact.” Same sex relations between women are not mentioned in Tanzania’s penal code.
[24] Zanzibar Penal Decree Act No. 6 of 2004, House of Representative s of Zanzibar, http://defensewiki.ibj.org/images/9/90/Zanzibar_Penal_Code.pdf , sections 150, 153.
[25] Ibid., art. 158.
[26] According to a World Bank funded study, 116 countries and territories around the world criminalize some aspect of sex work. Kerrigan et.al, The Global HIV Epidemics Among Sex Workers, Washington, DC: World Bank, 2013,p. 285.
[27] Tanzania Penal Code, art. 176(a).
[28] Zanzibar’s Penal Decree Act No. 6 of 2004, section 140.
[29] The Laws of Tanzania, Chapter 96, The Drugs and Prevention of Illicit Traffic in Drugs Act, 1995, art. 17; Drugs and Prevention of Illicit Traffic Drugs Act, 2009 (Zanzibar), sections 15(1)(c), 15(2), 16.
[30] Drugs and Prevention of Illicit Traffic Drugs Act, 2009 (Zanzibar), section 16(1)(c).
[31] Written Laws (Miscellaneous Amendment) Act of 2011 (Zanzibar), “Amendment of the Drugs and Prevention of Illicit Traffic Drugs Act, No, 9 of 2009,” section 12.
[32] Prime Minister’s Office, United Republic of Tanzania, “The Second National Multi-sectoral Strategic Framework on HIV/AIDS, 2008-2012 (Second Edition),” (English version), October 2007, http://www.entersoftsystems.com/tacaids/documents/NMSF%20%202008%20-2012.pdf, p. 57. The Kiswahili version is available here: http://www.entersoftsystems.com/tacaids/documents/MKAKATI%20WA%20UKIMW%202008%20-2012.pdf; see p. 48.” The quoted text comes from the official English version of the NMSF-II. The Kiswahili version, as noted above, fails to call for decriminalization, only calling for an end to “scorning” the activities of sex workers and MSM.
[33] Human Rights Watch interview with Dr. Salash Toure, Arusha, former Regional Medical Officer of Arusha, December 4, 2012.
[34] Human Rights Watch and WASO interview with a representative of a local HIV/AIDS organization, Arusha, December 4, 2012.
[35] Human Rights Watch interview with Umukulthum Ansell, director of ZAYEDESA, Zanzibar, September 13, 2012.
[36] Human Rights Watch interview with a representative of Tanzania Women Living with HIV/AIDS (TAWLWHIA), Mwanza, October 25, 2012.
[37] Human Rights Watch interview with a representative of Engender Health, Mwanza, October 25, 2012.
[38] Human Rights Watch interview with Dr. Joyce Nyoni, Dar es Salaam, September 14, 2012.
[39] Human Rights Watch interview with CHRAGG officials, Dar es Salaam, May 14, 2012.
[40] Joyce E. Nyoni and Michael W. Ross, “Condom Use and HIV-related behaviors in urban Tanzanian men who have sex with men: A study of beliefs, HIV knowledge sources, partner interactions and risk behaviours,” AIDS Care, 2012, p. 5.
[41] Ibid.
[42] Human Rights Watch interview with Daudi L., Mwanza, October 26, 2012.
[43] Human Rights Watch interview with Kashif M., Mwanza, October 27, 2012.
[44] PSI, an international health organization, has plans to initiate an HIV prevention program aimed at sex workers in Arusha. Human Rights Watch interview with PSI staff, Arusha, December 3, 2012.
[45] Human Rights Watch interview with a Tanzanian human rights activist, Kampala, April 17, 2013.
[46] A recent series of attacks on churches in Tanzania called into question the country’s tradition of religious tolerance. “Religious clashes in Tanzania, problems in government,” InformAfrica, October 18, 2012, http://www.informafrica.com/breaking-news-africa/news-religious-clashes-in-tanzania-problems-in-governnment/ (accessed January 21, 2013).
[47] Human Rights Watch interviews with Sabas Masame, Director of Dogodogo Centre, Dar es Salaam, September 3, 2012; with Justa Mwaituka, director of KIWOHEDE, Dar es Salaam, September 3, 2012; and with a representative of a human rights organization working with refugees, Dar es Salaam, September 7, 2012. On albinism, see Under the Same Sun, “Children with Albinism in Africa: Murder Mutilation and Violence - A report on Tanzania, With parallel references to other parts of Sub-Saharan Africa,” June 19, 2012, http://www.underthesamesun.com/sites/default/files/UTSS%20report%20to%20UN%20-%20REPORT_0.pdf (accessed May 9, 2013).
[48] Katrina Manson, “Politics: Young activists bring a belief that things must change,” Financial Times, December 6, 2012, http://www.ft.com/intl/cms/s/0/02230122-3bcf-11e2-b45f-00144feabdc0.html (accessed December 8, 2012).
[49] Human Rights Watch interview with Edward Nsajigwa of the Nyerere Centre for Human Rights, Dar es Salaam, June 25, 2012.
[50] Human Rights Watch interviews with representatives of diplomatic missions in Tanzania, Dar es Salaam, May 2012.
[51] Tanzania Penal Code, art. 154.
[52] Human Rights Watch, This Alien Legacy: The Origins of "Sodomy" Laws in British Colonialism, December 17, 2008, http://www.hrw.org/reports/2008/12/17/alien-legacy-0.
[53] UHAI, “A People Condemned: The Human Rights Status of Lesbian, Gay, Bisexual, Transgender and Intersex Persons In East Africa, 2009-2010,” 2010, http://www.uhai-eashri.org/ENG/resources (accessed January 21, 2013).
[54] Global Gayz, “Gay Tanzania News and Reports,” http://archive.globalgayz.com/africa/tanzania/gay-tanzania-news-and-reports/#article1 (accessed January 13, 2013).
[55] Privatus Lipili, “New turn in homosexuality storm in Anglican church,” Guardian, March 2, 2007, http://www.bongo5.com/new-turn-in-homosexuality-storm-in-anglican-church-03-2007/;” Bishops & Homosexuality,” Tanzanian Affairs, September 1, 2008, Issue 91, Religion, http://www.tzaffairs.org/2008/09/bishops-homosexuality/ (accessed January 16, 2013).
[56] Human Rights Watch interviews with TGNP staff and Gender Festival participants, Dar es Salaam, May 2012.
[57] Human Rights Watch and WASO interview with Saidi W., Dar es Salaam, June 30, 2012.
[58] Human Rights Watch interviews with Gender Festival participants, Dar es Salaam, May 2012.
[59] Under this process, the human rights record of each member country of the UN is evaluated every four years by other countries, who make recommendations as to how the country under review might improve its human rights record. See http://www.ohchr.org/EN/HRBodies/UPR/Pages/UPRMain.aspx.
[60] UPR-INFO.ORG, “Responses to Recommendations: Tanzania,” http://www.upr-info.org/IMG/pdf/recommendations_to_tanzania_2012.pdf (accessed January 16, 2012).
[61] “Homosexuality? Not in Tanzania!” Daily News (Dar es Salaam), November 5, 2011, http://www.dailynews.co.tz/editorial/?n=25180 (accessed January 16, 2013).
[62] Ibid.
[63] See for instance International Gay and Lesbian Human Rights Commission (IGLHRC), “Tanzania: Arbitrary Arrests and Detentions of Gay and Lesbian Activists,” October 30, 2009, http://www.iglhrc.org/cgi-bin/iowa/article/takeaction/resourcecenter/993.html (accessed January 16, 2012).
[64] A gay student interviewed for this report was suspended from Baraa Secondary School, a public school in Arusha, for looking effeminate, while a lesbian said she was kicked out of her private secondary school when her sexual identity became known to the school director. Human Rights Watch and WASO interviews with Lester F., Arusha, December 3, 2012, and with Rebecca F., Dar es Salaam, May 15, 2012. Two lesbians in Dar es Salaam reported being evicted by their landlords: Human Rights Watch interviews with Rebecca F., Dar es Salaam, May 15, 2012, and with Ruqayya V., Dar es Salaam, July 24. 2012. Discrimination also takes place in the workplace: one gay man said he had an internship in a law office, but “they told me to look for something else when they realized I was gay.” Human Rights Watch interview with Terence G., Dar es Salaam, May 7, 2012.
[65] Human Rights Watch and WASO interview with a representative of a community-based organization, Tanga, September 6, 2012.
[66] Human Rights Watch interview, date and location withheld.
[67] Human Rights Watch and WASO interview with Ali L., Tanga, September 5, 2012.
[68] Human Rights Watch interview with Abdalla J., Dar es Salaam, May 8, 2012.
[69] Human Rights Watch and WASO interview with Nicholas Y., September 6, 0212.
[70] UHAI, an East African sexual health and rights organization, documented the case of a transgender woman, Auntie Vicky, who was severely mistreated by Tanzanian hospital personnel in 2009. UHAI reported hospital officials at Muhimbili University “had exposed Aunt Vicky’s naked body to their colleagues and civilians and photographed her while she was still unconscious in hospital and that those photographs have been widely disseminated.” UHAI, “A People Condemned,” http://www.uhai-eashri.org/ENG/resources?download=4:uhai-a-people-condemned (accessed May 31, 2013).
[71] See, for instance, Marian Stevens, Gender DynamiX, “Transgender access to sexual health services in South Africa: findings from a key informant survey,” http://www.genderdynamix.org.za/wp-content/uploads/2012/10/Transgender-access-to-sexual-health-services-in-South-Africa.pdf (accessed May 31, 2013), September 2012. The study concluded, “It is evident that currently health services are discriminatory and health workers provide sub-standard care to transgender persons.”
[72] Human Rights Watch and WASO interview with Saidi W., Dar es Salaam, June 30, 2012.
[73] Kerrigan et.al, The Global HIV Epidemics Among Sex Workers, pp. xxvii, xxxiii.
[74] Ibid., pp. 284-285.
[75] National AIDS Control Programme, “HIV Behavioral and Biological Surveillance Survey Among Female Sex Workers in Dar es Salaam, 2010,” July 2011, p. 31.
[76] Human Rights Watch interview with a representative of AMREF, Mwanza, October 26, 2012.
[77] Human Rights Watch interview with Dhuriya M., Itumbi (Chunya District), December 9, 2012.
[78] National AIDS Control Programme, “HIV Behavioral and Biological Surveillance Survey Among Female Sex Workers in Dar es Salaam, 2010,” July 2011, p. 41.
[79] Ibid., p. 14.
[80] United Republic of Tanzania, “Violence Against Children in Tanzania Findings from a National Survey 2009,” http://www.unicef.org/media/files/VIOLENCE_AGAINST_CHILDREN_IN_TANZANIA_REPORT.pdf (accessed May 31, 2013), pp. 75-76. The study did not address cases of boys engaged in sex work. Human Rights Watch and WASO are aware that such cases exist, but we did not interview any male underage sex workers while conducting research for this report.
[81] See ILO Convention 182 on Convention concerning the Prohibition and Immediate Action for the Elimination of the Worst Forms of Child Labour 1999, entry into force November 19, 2000, article 3; Optional Protocol to the Convention on the Rights of the Child on the sale of children, child prostitution and child pornography, General Assembly resolution A/RES/54/263, adopted May 25, 2000, entered into force on 18 January 2002, acceded to by Tanzania on April 24, 2003.
[82] The Law of the Child Act No. 21 of 20 November 2009, http://www.ilo.org/wcmsp5/groups/public/---ed_protect/---protrav/---ilo_aids/documents/legaldocument/wcms_151287.pdf (accessed May 31, 2013), art. 83.
[83] US Department of State, Bureau of Democracy, Human Rights, and Labor, “2012 Human Rights Reports: Tanzania,” April 19, 2013, http://www.state.gov/j/drl/rls/hrrpt/2012/af/204176.htm (accessed May 9, 2013).
[84] Form 3 is the equivalent to 9th grade in the US.
[85] Human Rights Watch interview with Rosemary I., Mbeya, December 7, 2012.
[86] Médecins du Monde, “Assessment of risk practices and infectious diseas among drug users in Temeke District, Dar es Salaam, Tanzania,” 2011, p. 17. According to Médecins du Monde, “There is currently estimated to be 25,000-50,000 PWID [people who inject drugs] in Tanzania, although anecdotally this number is placed even higher. ”See also Ashery Mkama, “Drug Addiction On Increase Countrywide,” Daily News (Dar es Salaam), December 29, 2012, http://allafrica.com/stories/201212310239.html (accessed May 9, 2013), citing Drug Control Commission estimates that 150,000 to 500,000 people are addicted to drugs in Tanzania.
[87] World Health Organization, “New treatment gives hope to East Africa’s drug users,” Bulletin of the World Health Organization, Volume 91, Number 2, February 2013, 81-156, http://www.who.int/bulletin/volumes/91/2/13-030213/en/index.html (accessed April 3, 2013).
[88] Médecins du Monde, “Assessment of risk practices and infectious disease among drug users in Temeke District, Dar es Salaam, Tanzania,” 2011, p. 10, 16.
[89] Human Rights Watch interview with Sandrine Pont, general coordinator and country representative, Médecins du Monde, Dar es Salaam, December 6, 2012.
[90] “Tanzania: Tackling Drug Abuse in The Islands,” IRIN, April 9, 2010, http://www.irinnews.org/Report/88757/TANZANIA-Tackling-drug-abuse-in-the-islands (accessed December 19, 2012).
[91] For more information on methadone treatment, see Human Rights Watch, Rehabilitation Required: Russia’s Human Rights Obligation to Provide Evidence-based
Drug Dependence Treatment, Volume 19, No. 7(D) November 2007, http://www.hrw.org/sites/default/files/reports/russia1107webwcover.pdf, pp. 107-108.
[92] World Health Organization, “New treatment gives hope to East Africa’s drug users,” Bulletin of the World Health Organization, Volume 91, Number 2, February 2013, 81-156, http://www.who.int/bulletin/volumes/91/2/13-030213/en/index.html (accessed April 3, 2013).
[93] Human Rights Watch interview with representatives of the Zanzibar Drug Control Commission, Zanzibar, July 16, 2012.
[94] Human Rights Watch interview with January H., Dar es Salaam, June 26, 2012.
[95] Human Rights Watch interview with Abdul P., Zanzibar, September 13, 2012.
[96] Human Rights Watch and WASO interviews with female sex workers, Arusha, December 4, 2012.
[97] Legal and Human Rights Centre, 2013, pp. 21-22
[98] Legal and Human Rights Centre, 2013, pp. 24-25. According to the US State Department, “The LHRC reported in October that no police officer or other official security personnel had been convicted for extrajudicial killing of civilians since 2002,” “2012 Human Rights Reports: Tanzania,” April 19, 2013.
[99] 92 per cent of Tanzanians believe that the police force is corrupt, according to a recent survey conducted by the Afrobarometer and Policy Research for Development (REPOA). Respondents ranked the police as the most corrupt public institution in Tanzania. REPOA and Afrobarometer, “PROGRESS ON MKUKUTA*: Results from the Afrobarometer Round 5 Survey in Tanzania,” November 21, 2012, http://www.afrobarometer.org/files/documents/media_briefing/tan_r5_presentation1_21nov12.pdf, p. 18, 23 (accessed May 9, 2013).
[100] Human Rights Watch interview with a representative of a foreign aid agency, Dar es Salaam, June 27, 2012.
[101] Human Rights Watch interview with a representative of a human rights organization, Dar es Salaam, September 7, 2012; “MPs Join Public in Uproar Against Alleged Traffic Police Corruption,” Daily News (Dar es Salaam), June 30, 2012, http://allafrica.com/stories/201207020103.html (accessed May 9, 2013)
[102] Human Rights Watch interview with Deputy Police Commissioner Rashid Ali Omar, Dar es Salaam, September 10, 2012.
[103] Human Rights Watch interview with Suleiman R., Dar es Salaam, June 26, 2012.
[104]Maskani is a Kiswahili slang term used to signify an outdoor location for using drugs.
[105] Human Rights Watch interview with Zeitoun Y., Dar es Salaam, July 6, 2012.
[106] Human Rights Watch interview with Mwajuma P., Dar es Salaam, July 3, 2012.
[107] Human Rights Watch interview with Ally H., Dar es Salaam, September 15, 2012.
[108] Human Rights Watch interview with Ally H., Dar es Salaam, September 15, 2012.
[109] Human Rights Watch interview with Fazila Y., Dar es Salaam, July 18, 2012.
[110] Ibid.
[111] Human Rights Watch interview with Mickdad J., Dar es Salaam, July 3, 2012.
[112] Ibid.
[113] Human Rights Watch interview with John Elias, Dar es Salaam, June 26, 2012.
[114] Ibid.
[115] Ibid.
[116] Human Rights Watch interview with Edward Nsajigwa, director of the Nyerere Centre for Human Rights, Dar es Salaam, June 25, 2012.
[117] Human Rights Watch interview with a CHRAGG official, Dar es Salaam, April 8, 2013. On June 25, 2012, a Human Rights Watch researcher visited Elias’s home to speak with him, only to find that CHRAGG representatives had just picked him up in a vehicle to take him to the hospital. They had left a letter with Elias’s father, indicating the case was being investigated. Human Rights Watch has a copy of the letter on file, which is dated “HB/S/3/11/12/IGP/DSM of 7 September 2011.”CHRAGG did not respond to email inquiries from Human Rights Watch sent on August 28, 2012, and on March 28, 2013, as to what specific steps the commission was taking to address the case.
[118] Human Rights Watch interview with Musa E., Mbeya, December 12, 2012.
[119] Human Rights Watch interview with Omary Q., Zanzibar, May 17, 2012.
[120] Human Rights Watch interview with Nasir O., Zanzibar, May 17, 2012.
[121] Human Rights Watch interview with Sharifa Z., Zanzibar, September 13, 2012.
[122] Human Rights Watch interview with Suhayla F., Zanzibar, September 13, 2012.
[123] Human Rights Watch interview with Collins A., Dar es Salaam, June 22, 2012.
[124] Human Rights Watch interview with Collins A., Dar es Salaam, June 22, 2012.
[125] Human Rights Watch and WASO interview with Lester F., Arusha, December 3, 2012.
[126] Human Rights Watch and WASO interview with Lester F., Arusha, December 3, 2012.
[127] Human Rights Watch interview with Mariam H., Dar es Salaam, July 24, 2012.
[128] Human Rights Watch interview with Walid A., Zanzibar, September 13, 3012.
[129] Human Rights Watch interview with Alex N., Dar es Salaam, May 8, 2012.
[130] Human Rights Watch and WASO interview with Jessie L., Dar es Salaam, June 28, 2012.
[131] Human Rights Watch interview with Halima Y., Dar es Salaam, April 12, 2013.
[132] Human Rights Watch interview with Amanda Z., Dar es Salaam, April 12, 2013.
[133] Human Rights Watch and WASO interview with Ramazani H., Dar es Salaam, June 27, 2012.
[134] Human Rights Watch and WASO interview with Wilson N., Dar es Salaam, June 30, 2012.
[135] Human Rights Watch interview with Alamisi V., Mbeya, December 7, 2012.
[136] Human Rights Watch interview with Jenifer A., Mbeya, December 7, 2012.
[137] Human Rights Watch interview with Khadija J., Mbeya, December 7, 2012.
[138] Ibid.
[139] Human Rights Watch interview with Adimu S., Mbeya, December 7, 2012.
[140] Human Rights Watch interview with Rosemary I., Mbeya, December 7, 2012.
[141] Human Rights Watch and WASO interview with Ruby C., Mwanza, October 25, 2012.
[142] Human Rights Watch and WASO interview with Bishara A., Mwanza, October 26, 2012.
[143] Human Rights Watch interview with Harun Z., Dar es Salaam, June 26, 2012.
[144] Human Rights Watch and WASO interview with Ilham K., Dar es Salaam, July 4, 2012.
[145] Human Rights Watch interview with Evelyn D., Dar es Salaam, July 18, 2012.
[146] Human Rights Watch and WASO interview with Edwin J., Dar es Salaam, June 22, 2012.
[147] Human Rights Watch and WASO interview with Henry O., Mwanza, October 27, 2012.
[148] Human Rights Watch and WASO interview with Ilham K., Dar es Salaam, July 4, 2012.
[149] See François Ayissi et al. v. Cameroon, Working Group on Arbitrary Detention, Opinion No. 22/2006, U.N. Doc. A/HRC/4/40/Add.1 at 91 (2006), on file with Human Rights Watch.
[150] Human Rights Watch and WASO interview with Mohammed R., Dar es Salaam, July 5, 2012.
[151] Human Rights Watch and WASO interview with Victor G., Dar es Salaam, May 8, 2012.
[152] Human Rights Watch and WASO interview with Joseph S., Dar es Salaam, July 5, 2012.
[153] Human Rights Watch and WASO interview with Hussein M., Dar es Salaam, July 5, 2012.
[154] Human Rights Watch interview with Hamisi K., Zanzibar, September 13, 2012.
[155] Human Rights Watch interview with Hayat E., Dar es Salaam, July 24, 2012.
[156] Human Rights Watch interview with Mwajuma P., Dar es Salaam, July 3, 2012.
[157] One such militia group is the mgambo, a militia trained by the Tanzanian armed forces. We received little information about rights abuses by the mgambo.
[158] “Zanzibar Falls Victim to the International Heroin Trade,” VOA, March 4, 2012, http://www.voanews.com/content/zanzibar-falls-victim-to-the-international-heroin-trade-141414703/181120.html (accessed December 19, 2012).
[159] See Horace Campbell, “Popular Resistance in Tanzania: Lessons from the Sungu Sungu,” History research seminar series, 1987, on file with Human Rights Watch.
[160] The United Republic of Tanzania, Act No. 9 of 1989, “An Act to amend laws pertaining to the powers and operations of People’s Militia.”
[161] US Department of State, Bureau of Democracy, Human Rights and Labor, “Country Reports on Human Rights Practices for 2011: Tanzania,” http://www.state.gov/documents/organization/186460.pdf, p. 7 (accessed January 23, 2013).
[162] Human Rights Watch interview with Police Commissioner Paul Chagonja, acting inspector general of police, Dar es Salaam, September 10, 2012.
[163] Human Rights Watch interview with Alfie N., Dar es Salaam, June 25, 2012.
[164] Human Rights Watch interview, Dar es Salaam, June 25, 2012.
[165] Human Rights Watch interview with Alfie N., Dar es Salaam, June 25, 2012.
[166] Human Rights Watch interview with the victim’s mother, Dar es Salaam, June 25, 2012.
[167] Ibid.
[168] Human Rights Watch interview with Médecins du Monde employees, Dar es Salaam and by telephone, December 6, 2012.
[169] Human Rights Watch interview with Rashid E., Dar es Salaam, June 26, 2012. Human Rights Watch observed Rashid E.’s crooker finger, and broad, black marks on his hand, which were consistent with being beaten by a panga.
[170] Human Rights Watch interview with Mwanahamisi K., Dar es Salaam, June 25, 2012.
[171] Ibid.
[172] Human Rights Watch interview with Angela G., Dar es Salaam, July 24, 2012.
[173] Human Rights Watch interview with Susan N., Dar es Salaam, July 24, 2012.
[174] Human Rights Watch interview with Rosemary I., Nadia O., and Asha W., Mbeya, December 7, 2012.
[175] Human Rights Watch interview with John Badia Olwasi, director of CADAAG, Arusha, December 3, 2012.
[176] Human Rights Watch interview with a local activist, Mwanza, October 27, 2012.
[177] Human Rights Watch interview with an outreach worker, Zanzibar, May 17, 2012.
[178] Ibid.
[179] Human Rights Watch interview with Idris Z., Zanzibar, May 17, 2012.
[180] Human Rights Watch interview with Abdilah D., Dar es Salaam, May 9, 2012.
[181] Ibid.
[182] Human Rights Watch interview with Ally H., Dar es Salaam, September 15, 2012.
[183] Ibid.
[184] Human Rights Watch interview with Asha W., Mbeya, December 7, 2012.
[185] Human Rights Watch interview with Mwamini K., Dar es Salaam, May 15, 2012.
[186] Human Rights Watch and WASO interview with Louisa T., Mwanza, October 25, 2012.
[187] Human Rights Watch interview with Mickdad J., Dar es Salaam, July 3, 2012.
[188] Legal and Human Rights Centre has documented dozens of cases of mob justice in Tanzania; a recent report found that “most affected people of this archaic mode of community punishment are pick pocketers, petty thieves, suspected witches and other people believed to be source [sic] of problem to the community.” LHRC, 2013, pp. 26-31.
[189] Human Rights Watch interview with Watende A., Dar es Salaam, July 6, 2012.
[190] Human Rights Watch interview with Jamal P., Zanzibar, May 17, 2012.
[191] Human Rights Watch and WASO interview with Abdalla J., Dar es Salaam, May 8, 2012.
[192] Human Rights Watch and WASO interview with Rahim R., Dar es Salaam, May 8, 2012.
[193] Human Rights Watch and WASO interview with Ramazani H., Dar es Salaam, June 27, 2012.
[194] Human Rights Watch and WASO interview with Wilson N., Dar es Salaam, June 30, 2012.
[195] Human Rights Watch and WASO interview with Ismail P., Dar es Salaam, June 27, 2012.
[196] According to an official at the Ministry of Community Development, Gender, and Children, 417 Gender Desks had been established throughout the country by April 2013. However, the official acknowledged that officers who had received training to run the Gender Desks had not received training on sex workers’ needs. Human Rights Watch interview with Anna Maembe, Deputy Permanent Secretary, Ministry of Community Development, Gender, and Children, Dar es Salaam, April 8, 2013.
[197] Human Rights Watch interview with Geoffrey Kiangi, acting director of Preventive Services, Ministry of Health and Social Welfare, September 10, 2012.
[198] Human Rights Watch interview with representatives of the Zanzibar AIDS Control Programme, Zanzibar, May 17, 2012.
[199] Human Rights Watch interview with an LGBT rights activist, Dar es Salaam, May 7, 2012.
[200] Human Rights Watch telephone interview with Richard Killian, Country Representative of Engender Health in Tanzania, October 25, 2012.
[201] Email communication from a Médecins du Monde official to Human Rights Watch, March 18, 2013.
[202] Human Rights Watch interview with Christian B., Mbeya, December 12. 2012.
[203] Human Rights Watch interview with John Badia Olwasi, CADAAG director, Arusha, December 3, 2012.
[204] Human Rights Watch interview with a representative of AMREF, Mwanza, October 26, 2012.
[205] Human Rights Watch and WASO interviews with MSM, Dar es Salaam, June 2012; Human Rights Watch interview with Dr. Simon Yohana, director of PASADA, Dar es Salaam, July 6, 2012.
[206] Human Rights Watch and WASO interview with Collins A., Dar es Salaam, June 22, 2012.
[207] Human Rights Watch interview with Alex N., Dar es Salaam, May 8, 2012.
[208] Human Rights Watch and WASO interview with Yusuf G., Dar es Salaam, June 30, 2012.
[209] Human Rights Watch interview with Ally Semsella and Peter Celestin, Dar es Salaam, April 8, 2013.
[210] Human Rights Watch interview with Jamal P., Zanzibar, May 17, 2012.
[211] Human Rights Watch interview with representatives of the Zanzibar Drug Control Commission, Zanzibar, May 16, 2012.
[212] Human Rights Watch interview with an LGBT rights activist, Zanzibar, May 17, 2012.
[213] Human Rights Watch interview with Dr. Ramadhan Issa Hassan, MARPs specialist at Mnazi Mmoja Hospital, Zanzibar. September 13, 2012.
[214] Human Rights Watch and WASO interview with Lester F., Arusha, December 3, 2012.
[215] Human Rights Watch and WASO interview with Carlos B., Dar es Salaam, June 27, 2012.
[216] Human Rights Watch and WASO interview with Ismail P., Dar es Salaam, June 27, 2012.
[217] Human Rights Watch and WASO interview with Mohammed R., Dar es Salaam, July 5, 2012.
[218] Human Rights Watch and WASO interview with Peter E., Dar es Salaam, June 27, 2012.
[219] Human Rights Watch and WASO interview with Ismail P., Dar es Salaam, June 27, 2012.
[220] Human Rights Watch interview with Hayat E., Dar es Salaam, July 24, 2012.
[221] Human Rights Watch interview with Mwajuma P., Dar es Salaam, July 3, 2012.
[222] Human Rights Watch interview with Mickdad J., Dar es Salaam, July 3, 2012.
[223] Human Rights Watch and WASO interview with a representative of a community-based organization, Tanga, September 6, 2012.
[224] Human Rights Watch and WASO were unable to identify the legal or regulatory source of the PF3 requirement. A police official told Human Rights Watch that she believed the PF3 requirement was set forth in the Criminal Procedure Code, but it is not. The Ministry of Health and Social Welfare did not respond to a letter from Human Rights Watch, delivered by hand on April 8, 2013, inquiring as to the legal status of the PF3 form.
[225] Human Rights Watch interview with Deputy Police Commissioner Rashid Ali Omar, Dar es Salaam, September 10, 2012.
[226] Ibid.
[227] Human Rights Watch interview with Suleiman R., Dar es Salaam, June 26, 2012.
[228] Human Rights Watch interview with Susan N., Dar es Salaam, July 24, 2012.
[229] Human Rights Watch and WASO interview with Walter S., Mwanza, October 27, 2012.
[230] Human Rights Watch interview with Mwamini K., Dar es Salaam, May 15, 2012.
[231] Human Rights Watch and WASO interview with Jamila H., Dar es Salaam, July 4, 2012.
[232] Human Rights Watch interview with Maureen B., Dar es Salaam, July 24, 2012.
[233] Human Rights Watch interview with Dalili S., Dar es Salaam, July 24, 2012.
[234] Florence Mugarula, “Tanzania: Ministry Moves to Assist Gender Violence Victims,” The Citizen (Dar es Salaam), December 18, 2011, http://allafrica.com/stories/201112191419.html (accessed February 11, 2013); email communication to Human Rights Watch from a representative of the UN Population Fund (UNFPA), June 5, 2013.
[235] Human Rights Watch interview with Mwamini K., Dar es Salaam, May 15, 2012.
[236] Human Rights Watch interview with Pili M., Dar es Salaam, May 15, 2012.
[237] Human Rights Watch and WASO interview with Melissa L., Arusha, December 4, 2012.
[238] Human Rights Watch interviews with a representative of ZASOSE, a community-based organization, and ICAP, an international NGO, Zanzibar, May 16, 2012.
[239] Human Rights Watch and WASO interview with Lester F., Arusha, December 3, 2012.
[240] Human Rights Watch interview with Christian B., Mbeya, December 12, 2012.
[241] Human Rights Watch and WASO interview with Ali L., Tanga, September 5, 2012.
[242] International Covenant on Civil and Political Rights (ICCPR), adopted December 16, 1966, G.A. Res. 2200A (XXI), 21 U.N. GAOR Supp. (No. 16) at 52, U.N. Doc. A/6316 (1966), 999 U.N.T.S. 171, entered into force March 23, 1976, acceded to by Tanzania on June 11, 1986. Articles 2 and 26 of the ICCPR affirm the equality of all people before the law and the right to freedom from discrimination. Article 17 protects the right to privacy. See also Toonen v. Australia, 50th Sess., Communication No. 488/1992, U.N. Doc CCPR/C/50/D/488/1992, April, 14, 1994, sec. 8.7.
[243] See François Ayissi et al. v. Cameroon, Working Group on Arbitrary Detention, Opinion No. 22/2006, U.N. Doc. A/HRC/4/40/Add.1 at 91 (2006), on file with Human Rights Watch.
[244] The African [Banjul] Charter on Human and Peoples’ Rights, adopted June 27, 1981, OAU Doc. CAB/LEG/67/3 rev. 5, 21I.L.M. 58 (1982), entered into force October 21, 1986, acceded to by Tanzania, February 18, 1984, article 2. See the African Commission on Human and People’s Rights, Zimbabwe Human Rights NGO Forum v. Zimbabwe, sec. 169, AHRLR 128 (ACHPR 2006).
[245] Constitution of the United Republic of Tanzania (last amended 1985) [United Republic of Tanzania], April 26, 1977, http://www.unhcr.org/refworld/docid/3ae6b50c4.html, (accessed 21 January 2013), art. 9. Use of capitalization in the quoted section follows the original.
[246] Ibid., art. 13.
[247] Ibid., art. 16.
[248] ICCPR, art. 17.
[249] ICCPR art.9; African [Banjul] Charter on Human and Peoples' Rights, adopted June 27, 1981, OAU Doc. CAB/LEG/67/3 rev. 5, 21 I.L.M. 58 (1982), entered into force October 21, 1986, art. 4, 6.
[250] Constitution of the United Republic of Tanzania (last amended 1985) [United Republic of Tanzania], April 26, 1977, http://www.unhcr.org/refworld/docid/3ae6b50c4.html (accessed 21 January 2013), art. 15(2)a.
[251] See the Law of the Child Act No. 21 of 20 November 2009, http://www.ilo.org/wcmsp5/groups/public/---ed_protect/---protrav/---ilo_aids/documents/legaldocument/wcms_151287.pdf (accessed May 3, 2013), art. 83; UN General Assembly, Convention on the Rights of the Child, 20 November 1989, United Nations, Treaty Series, vol. 1577, p. 3, http://www.unhcr.org/refworld/docid/3ae6b38f0.html (accessed May 31, 2013), art. 34; International Labour Organization (ILO), Worst Forms of Child Labour Convention, C182, 17 June 1999, C182, http://www.unhcr.org/refworld/docid/3ddb6e0c4.html (accessed 31, 2013), art. 3(b); and the African Charter on the Rights and Welfare of the Child, OAU Doc. CAB/LEG/24.9/49 (1990), entered into force Nov. 29, 1999., art. 27.
[252] National Costed Plan of Action for Most Vulnerable Children, October 2012, p. 2, on file with Human Rights Watch.
[253] ICCPR art.9; African [Banjul] Charter on Human and Peoples' Rights, adopted June 27, 1981, OAU Doc. CAB/LEG/67/3 rev. 5, 21 I.L.M. 58 (1982), entered into force October 21, 1986, art. 4, 6.
[254] ACHPR, art. 5; ACCPR art. 7 and 10.
[255] Convention against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment (Convention against Torture), adopted December 10, 1984, G.A. res. 39/46, annex, 39 U.N.GAOR Supp. (No. 51) at 197, U.N. Doc. A/39/51 (1984), entered into force June 26, 1987.
[256] Constitution of the United Republic of Tanzania (last amended 1985) [United Republic of Tanzania], April 26, 1977, http://www.unhcr.org/refworld/docid/3ae6b50c4.html (accessed May 31, 2013), art. 13(6)e.
[257] Ibid., art. 13(6)d.
[258] African [Banjul] Charter on Human and Peoples' Rights , op. cit., art. 16; International Covenant on Economic, Social and Cultural Rights (ICESCR), adopted December 16, 1966, G.A. Res. 2200A (XXI), 21 U.N. GAOR Supp. (No. 16) at 49, U.N. Doc. A/6316 (1966), 993 U.N.T.S. 3, entered into force January 3, 1976, ratified by Tanzania on June 11, 1976, art. 12; CEDAW, adopted December 18, 1979, G.A. Res. 34/180, U.N. Doc. A/34/46, entered into force September
3, 1981 and acceded to by Tanzania on August 20, 1985, article 12.
[259] See UN Committee on Economic, Social and Cultural Rights, General comment No. 20: Non-discrimination in economic, social and cultural rights (art. 2, para. 2, of the International Covenant on Economic, Social and Cultural Rights), July 2, 2009, para. 32. While article 12 guarantees the right to health, article 2(2) protects individuals from discrimination in the application of all rights guaranteed by the covenant. General Comment 20 clarifies that discrimination is prohibited on the basis of sexual orientation and gender identity.
[260] Committee on Economic, Social and Cultural Rights (CESCR), The Right to the Highest Attainable Standard of Health, (Art 12), E/C.12/2000/4, (August. 11, 2000) General Comment no. 14, on the normative content of article 12 of the ICESCR, para 9.
[261] The Beckley Foundation Drug Policy Programme, “Recalibrating the Regime: The Need for a Human Rights-Based Approach to International Drug Policy,” Report Thirteen, March 2008, http://www.hrw.org/legacy/pub/2008/hivaids/beckley0308.pdf (accessed May 31, 2013), pp. 33-34.
[262] Eastern Africa National Networks of AIDS Service Organizations (EANNASO), “The East African Legislative Assembly passes the EAC HIV & AIDS Prevention and Management Bill, 2012,” undated press release (April 2012), http://www.eannaso.org/index.php?option=com_content&view=article&id=48%3Apress-realease-eac-aids-law&catid=73%3Aeac-hiv-bill&Itemid=56&lang=en (accessed January 3, 2013).
[263] East African Community HIV & AIDS Prevention and Management Bill, 2012, http://www.eannaso.org/index.php?option=com_docman&task=cat_view&Itemid=10&gid=74&orderby=dmdate_published&ascdesc=DESC&lang=en (accessed January 3, 2013), section 7(h) and 11(d). However, the East African Legislative Assembly’s diffidence in addressing the needs of key populations, and the politicized nature of this important health issue, are evidenced by the fact that the EALA refused to spell out what constituted “most-at-risk populations” in the text of the bill. A proposal by some drafters to clarify that the term referred specifically to men having sex with men, sex workers and people who inject drugs was rejected by government officials involved in the drafting process, who argued that the bill should not “recognize or legitimize conduct which is expressly criminalized” by national laws; see Notes to the Draft East African Community HIV and AIDS Prevention and Management Bill, 2010, http://www.eannaso.org/index.php?option=com_docman&task=cat_view&Itemid=10&gid=74&orderby=dmdate_published&ascdesc=DESC&lang=en (accessed January 3, 2013). The bill is thus weaker in its approach to MARPs than national legislation in Tanzania, Kenya, Rwanda, and Burundi.
[264] East African Community HIV & AIDS Prevention and Management Bill, 2012, section 38(1).
[265] Ibid., section 13(b). The section refers specifically to “quality female and male condoms;” however, water-based lubricant would also qualify as a recognized protective method. See, for instance, the World Health Organization (WHO) and UNAIDS, The Male Latex Condom: 10 Condom Programming Fact Sheets, http://www.unaids.org/en/media/unaids/contentassets/dataimport/publications/irc-pub01/jc003-malecondom-factsheets_en.pdf (accessed June 5, 2013), p. 7.
[266] African Union, Protocol to the African Charter on Human and People's Rights on the Rights of Women in Africa, 11 July 2003, http://www.africa-union.org/root/au/Documents/Treaties/Text/Protocol%20on%20the%20Rights%20of%20Women.pdf (accessed May 31, 2013), art. 14(1)d.
[267] ICCPR articles 2, 7, 17.
[268] Maputo Protocol, art. 3(4).
[269] Ibid., art. 4(2)a.
[270] Ibid., art. 4(2)e.
[271] Tanzania penal code, art. 131(1); Zanzibar Penal Decree Act No. 6 of 2004, section 126(1).
[272] Tanzania penal code, art. 130(1); Zanzibar Penal Decree Act No. 6 of 2004, section 125(1).
[273] Laws of Tanzania, Chapter 239, The Prevention and Combating Corruption Act No. 11/2007 (PCCA), section 25.
[274] Human Rights Watch interview with a PCCB official, Dar es Salaam, September 11, 2012; PCCA, section 52.
[275] Human Rights Watch interview with Elice Mapunda, Dar es Salaam, April 10, 2013.
[276] Human Rights Watch interview with William Kafura, Dar es Salaam, April 8, 2013.
[277] Human Rights Watch interview with Anna Maembe, Dar es Salaam, April 8, 2013.
[278] REPOA and Afrobarometer, “PROGRESS ON MKUKUTA*: Results from the Afrobarometer Round 5 Survey in Tanzania.”
[279] US Department of State, Bureau of Democracy, Human Rights, and Labor, “2012 Human Rights Reports: Tanzania.”
[280] Human Rights Watch interview with a PCCB official, Dar es Salaam, September 11, 2012.
[281] Human Rights Watch interview with a UN official, Dar es Salaam, April 8, 2013.
[282] Human Rights Watch interview with a UN official, Dar es Salaam, April 12, 2013; US Embassy in Dar es Salaam, “President Kikwete Visits CDC Site,” March 26, 2013, http://tanzania.usembassy.gov/ph_03262013.html (accessed May 9, 2013).